Growth Hormone Treatment in Dent Disease: A Case Report
Elisa Guidoni1, Federica Lotti1, Ursula Geronzi1, Maddalena Cioni1, Salvatore Grosso1, Giovanna Municchi1
Citation : Guidoni E, Lotti F, Geronzi U, Cioni M, Grosso S, Municchi G. Growth Hormone Treatment in Dent Disease: A Case Report. Clinical Research in Diabetes and Endocrinology 2018;1(1):1-4.
Dent's disease is a rare X-linked renal tubulopathy characterized by low-molecular-weight proteinuria, hypercalciuria, nephrocalcinosis, nephrolithiasis, and progressive renal failure. Common features are also rickets or osteomalacia, growth retardation, and short stature. We report the case of a boy affected by Dent's disease, treated with recombinant human growth hormone (GH). Dent's disease was diagnosed at 6.5 years of age on the basis of the inactivating mutation in CLCN5 gene. The boy had also dysmorphisms, mild mental retardation, and short stature (<-3 SD), in addition to the typical renal alterations of the syndrome. Target height was 180 cm (0.6 SD). GH therapy was started at a chronological age of 11 years and 6 months, with a bone age (Greulich and Pyle method) of 9 years; growth velocity was 3.4 cm/year (-2.6 SD) and creatinine clearance 81 ml/min/1.73 m2 (normal range 89-165). After 6 months of GH treatment (40 mcg/kg/day), height increased from 124.5 cm (-3.4 SD) to 128.8 cm (-3.1 SD), insulin-like growth factor I (IGF-I) levels increased from 57.8 ng/ml (88-770) to 150 ng/ml, and creatinine clearance was 75 ml/min/1.73 m2 (70-120 range for >12 years). After 1 year on GH therapy, height was 132 cm (-2.9 SD), growth velocity 7.5 cm/year (3.2 SD), bone age 10 years, IGF-I level 177 ng/ml, and creatinine clearance 109 ml/min/1.73 m2. After 2 years on GH therapy, height was 138.5 cm (-2.8 SD), growth velocity 6.5 cm/year (-0.1 SD), bone age 10.5 years, IGF-I level 393 ng/ml, and creatinine clearance 119 ml/min/1.73 m2. Our preliminary findings showed beneficial effect of GH treatment on growth velocity and renal function parameters. Further, follow-up is needed to confirm these preliminary positive results. GH treatment should be considered in children with Dent's disease and short stature since extremely positive effects on linear growth and renal function can be obtained. Only three patients with Dent's disease treated with GH have been reported in the literature, all showing encouraging results. Unfortunately, the small number of patients reported does not allow to draw definitive conclusions on the beneficial effect of GH treatment.
disease, growth hormone treatment, growth hormone
INTRODUCTION
Dent's disease refers to a group of X-linked renal tubular disorders including X-linked recessive nephrolithiasis, X-linked recessive hypophosphatemic rickets, and idiopathic low-molecular-weight (LMW) proteinuria with hypercalciuria and nephrocalcinosis [1-4]. It is a rare disorder, about 250 affected families have been described in literature, but the prevalence of this condition could be underestimated due to the extreme variability of the clinical presentation [5].
Dent's disease 1 (approximately 60% of patients) is caused by mutations affecting the CLCN5 gene, located on chromosome Xp11.22, which encodes for the ClC-5 chloride channel [6-8].
Dent's disease 2 (about 15% of patients) is caused by disorders in the OCRL gene, located on chromosome Xq25, which encodes a PIP2 5-phosphatase, and it is usually mutated in patients with Lowe syndrome [9-11]. About 25% of patients with clinical features of Dent's disease do not have CLCN5/OCRL mutations, implicating the involvement of other genes [9,12,13].
Diagnosis is based on the presence of three criteria without other known causes of proximal tubule dysfunction: LMW proteinuria, hypercalciuria, and at least one of the following: Nephrocalcinosis, nephrolithiasis, hematuria, hypophosphatemia, chronic kidney disease, or family history consistent with X-linked inheritance. Molecular genetic analysis confirms the diagnosis [13,14].
In the early stages, children are usually asymptomatic, they may manifest only LMW proteinuria and/or hypercalciuria [15].
Progression to end-stage renal disease occurs between ages 30 and 50 years in 30-80% of patients [16].
Common clinical features are rickets, growth retardation, and short stature [17].
About 50% of patients with Dent disease 2 present mild intellectual disability [9,18].
No guidelines have been established for Dent's disease treatment. The aims of therapy with thiazide diuretics, angiotensin-converting enzyme (ACE) inhibitors, and angiotensin receptor blockers are to prevent nephrolithiasis and nephrocalcinosis and delay the progression of chronic kidney failure [19,20].
Vitamin D and phosphorus supplementations are used to prevent bone secondary complications [2].
To date, few reports suggest a positive effect of growth hormone (GH) therapy on growth failure and short stature without adverse events on kidney function [21,22].
CASE REPORT
The boy was referred to the Pediatric Endocrinology Outpatient Clinic of the University of Siena at the chronological age (CA) of 11.5 years for short stature. The patient's family history was negative for short stature and delayed puberty: Maternal grandfather had nephrolithiasis, paternal grandmother had tibia vara, and a first-degree cousin had mental retardation of unknown origin. The patient was born at term following an uneventful pregnancy with birth weight and length at 10°-25° percentile. His medical history revealed an orthopedic evaluation for bilateral tibia vara at 3 years of age, with diagnosis of rickets and replacement therapy with 25-hydroxycholecalciferol (10 mcg/die) and orthotics. Neurological and neuropsychiatric evaluations were performed at 6 years of age for dysmorphisms and hyperactivity. These investigations revealed the presence of hypophosphoremia, hypercalciuria, LMW proteinuria, and non-selective aminoaciduria, in addition to mild mental retardation (IQ 70) and attention deficit hyperactivity disorder. Subsequent nephrologic and genetic evaluations led to the diagnosis of Dent's disease 1, caused by an inactivating mutation in CLCN5 gene.
After 5 years on conventional treatment with hydrochlorothiazide and ACE inhibitor and potassium replacement therapy, the boy was referred at the CA of 11.5 years for an endocrine evaluation for short stature.
Height was 124.5 cm (-3.4 SD), target height 180 cm (0.6 SD), growth velocity 3.4 cm/year (-2.6 SD), and weight 28 kg (-2.0 SD); testes were prepubertal, with no pubic or axillary hair. The boy presented dysmorphisms: Triangular facies with severe prognathism, crossbite, low forehead and low-set ears, pectus excavatum, and disproportions of the lower limbs (right >left about 2 cm) with bilateral tibia vara. Cardiorespiratory and abdominal examination revealed no abnormalities, heart rate was 90/min, and blood pressure was 95/60 mmHg.
Baseline investigations showed normal blood count, electrolytes, and liver function. Evaluation of renal function showed serum creatinine, calciuria, phosphaturia, and creatininuria within the normal range. Creatinine clearance (Schwartz formula) was 81 ml/min/1.73m2 (89-165 range for 2-12 years).
Serum-free thyroxine, thyroid-stimulating hormone, and parathyroid hormone were normal. Follicle-stimulating hormone, luteinizing hormone, and testosterone were within prepubertal limits. 25-OH Vitamin D level was 22.8 ng/ml (20-30 insufficiency); therefore, Vitamin D replacement therapy was started. Insulin-like growth factor I (IGF-I) showed very low level of 57.8 ng/ml (88-770). Bone age (Greulich and Pyle method) was 9 years. GH therapy (40 mcg/kg/day) was started at a CA of 11 years and 6 months, in addition to the conventional treatment.
The planned follow-up includes auxological evaluation every 3 months during the first 6 months of GH therapy and then every 6 months: Serum measurement of glucose, glycated hemoglobin, iron, transferrin, ferritin, liver function, creatinine, electrolytes, calcium, phosphorus, 25-OH Vitamin D, and IGF-1 every 6 months; bone age every year.
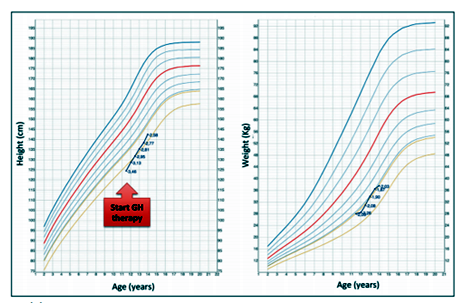
After 6 months of GH therapy and Vitamin D replacement treatment, in addition to hydrochlorothiazide and ACE inhibitor and potassium replacement, height was 128.8 cm (-3.1 SD), IGF-I level increased to 150 ng/ml, and creatinine clearance was 75 ml/min/1.73 m2 (70-120 range for >12 years). After 1 year on GH and Vitamin D replacement therapy, height was 132 cm (-2.9 SD), growth velocity was 7.5 cm/year (3.2 SD), bone age was 10 years, IGF-I level was 177 ng/ml, 25-OH Vitamin D was 56 ng/ml (normal values 30-100), and creatinine clearance was 109 ml/min/1.73 m2. After 2 years on GH and Vitamin D replacement therapy, height was 138.5 cm (-2.8 SD), growth velocity was 6.5 cm/year (-0,1 SD), bone age was 10.5 years, IGF-I level was 393 ng/ml, 25-OH Vitamin D was 64.6 ng/ml, and creatinine clearance was 119 ml/min/1.73 m2.
At the last evaluation at 14 years of age, height was 142.6 cm (-2.6 SD), weight was 37.6 kg (-2.0 SD), and pubertal status was Tanner Stage 3 [Figure 1].
CONCLUSION
To the best of our knowledge, there are only three reports on GH therapy in children with Dent's disease and growth retardation [21,22]. Sheffer-Babila et al. reported the case of two brothers, 10 and 13.5 years old, affected by Dent's disease and GH deficiency. After 2 years on GH therapy, they showed an excellent growth response; they showed also an improvement of tubular resorption phosphate while the estimated glomerular filtration rate was stable [21].
Samardzic et al. described the case of a 7-year-old boy with Dent's disease, rickets, and short stature treated with GH therapy. In the first 2 years, the patient showed a great improvement of growth velocity and no relevant changes in creatinine clearance, which remained normal [22].
During the first 2 years on GH therapy, our patient grew at an average rate of 7 cm/year (1.8 SD). Bone age did not accelerate and the patient started pubertal development. Renal function showed an improvement of the creatinine clearance (calculated with Swartz formula) from 81 ml/min/1.73m2 (89-165 range for 2-12 years) to 119 ml/min/1.73 m2 (70-120 range for >12 years).
Our preliminary findings showed beneficial effects of GH treatment on growth velocity and renal function parameters. Further, follow-up is needed to confirm these preliminary positive results.
GH treatment should be considered in children affected by Dent's disease and short stature, even in the absence of reduced GH secretion, because it may have extremely positive effects on linear growth and renal function.
The few patients with Dent's disease treated with GH reported in the literature showed encouraging results, in particular, on growth velocity. Unfortunately, their small number and the short follow-up do not allow to draw conclusions on the beneficial effect of GH treatment.
References
- Wrong OM, Norden AG, Feest TG. Dent's disease; A familial proximal renal tubular syndrome with low-molecular-weight proteinuria, hypercalciuria, nephrocalcinosis, metabolic bone disease, progressive renal failure and a marked male predominance. QJM 1994;87:473-93.
- Wrong OM, Norden AG, Feest TG. Dent's disease; A familial proximal renal tubular syndrome with low molecular weight proteinuria, hypercalciuria, nephrocalcinosis, metabolic bone disease, progressive renal failure and a marked male predominance. QJM 1994;87:473-93.
- Lloyd SE, Pearce SH, Fisher SE, Steinmeyer K, Schwappach B, Scheinman SJ, et al. A common molecular basis for three inherited kidney stone diseases. Nature 1996;379:445-9.
- Thakker RV. Pathogenesis of dent's disease and related syndromes of X-linked nephrolithiasis. Kidney Int 2000;57:787-93.
- Devuyst O, Thakker RV. Dent's disease. Orphanet J Rare Dis 2010;5:28.
- Gunther W, Luchow A, Cluzeaud F, Vandewalle A, Jentsch TJ. ClC-5, the chloride channel mutated in dent's disease, colocalizes with the proton pump in endocytotically active kidney cells. Proc Natl Acad Sci U S A 1998;95:8075-80.
- Devuyst O, Christie PT, Courtoy PJ, Beauwens R, Thakker RV. Intra-renal and subcellular distribution of the human chloride channel, CLC-5, reveals a pathophysiological basis for dent's disease. Hum Mol Genet 1999;8:247-57.
- Hara-Chikuma M, Wang Y, Guggino SE, Guggino WB, Verkman AS. Impaired acidification in early endosomes of clC-5 deficient proximal tubule. Biochem Biophys Res Commun 2005;329:941-6.
- Hoopes RR Jr., Shrimpton AE, Knohl SJ, Hueber P, Hoppe B, Matyus J, et al. Dent disease with mutations in OCRL1. Am J Hum Genet 2005;76:260-7.
- Sekine T, Nou K, Iyengar R, Fu XJ, Matsuo M, Tanaka R, et al. OCRL1 mutations in patients with dent disease phenotype in Japan. Pediatr Nephrol 2007;22:975-80.
- Utsch B, Bokenkamp A, Benz MR, Besbas N, Dotsch J, Franke I, et al. Novel OCRL1 mutations in patients with the phenotype of dent disease. Am J Kidney Dis 2006;48:942.e1-14.
- Cho HY, Lee BH, Choi HJ, Ha IS, Choi Y, Cheong HI. Renal manifestations of dent disease and Lowe syndrome. Pediatr Nephrol 2008;23:243-9.
- Hoopes RR Jr., Raja KM, Koich A, Hueber P, Reid R, Knohl SJ, et al. Evidence for genetic heterogeneity in dent's disease. Kidney Int 2004;65:1615-20.
- Edvardsson VO, Goldfarb DS, Lieske JC, Beara-Lasic L, Anglani F, Milliner DS, et al. Hereditary causes of kidney stones and chronic kidney disease. Pediatr Nephrol 2013;28:1923-42.
- Claverie-Martin F, Ramos-Trujillo E, Garcia-Nieto V. Dent's disease: Clinical features and molecular basis. Pediatr Nephrol 2011;26:693-704.
- Scheinman SJ. X-linked hypercalciuric nephrolithiasis: Clinical syndromes and chloride channel mutations. Kidney Int 1998;53:3-17.
- Bokenkamp A, Bockenhauer D, Cheong HI, Hoppe B, Tasic V, Unwin R, et al. Dent-2 disease: A mild variant of Lowe syndrome. J Pediatr 2009;155:94-9.
- Shrimpton AE, Hoopes RR Jr., Knohl SJ, Hueber P, Reed AA, Christie PT, et al. OCRL1 mutations in dent 2 patients suggest a mechanism for phenotypic variability. Nephron Physiol 2009;112:27-36.
- Raja KA, Schurman S, D'Mello RG, Blowey D, Goodyer P, Van Why S, et al. Responsiveness of hypercalciuria to thiazide in dent's disease. J Am Soc Nephrol 2002;13:2938-44.
- Blanchard A, Vargas-Poussou R, Peyrard S, Mogenet A, Baudouin V, Boudailliez B, et al. Effect of hydrochlorothiazide on urinary calcium excretion in dent disease: An uncontrolled trial. Am J Kidney Dis 2008;52:1084-95.
- Sheffer-Babila S, Chandra M, Speiser PW. Growth hormone improves growth rate and preserves renal function in dent disease. J Pediatr Endocrinol Metab 2008;21:279-86.
- Samardzic M, Pavicevic S, Ludwig M, Bogdanovic R. Effect of growth hormone replacement therapy in a boy with dent's disease: A case report. J Med Case Rep 2011;5:400.