Metastatic Prostate Cancer Presenting as a Virchow's Node
Joshua K Phillips*, Anthony Sabo, Robert Naraine, Lou Lyras, Peter Devito
Citation : Phillips JK, Sabo A, Naraine R, Lyras L, Devito P. Metastatic Prostate Cancer Presenting as a Virchow's Node. Asclepius Med Case Rep 2018;1(1):1-3.
Prostate cancer remains the most common non-cutaneous malignancy in American men and the third leading cause of cancer-associated mortality. Prostate cancer presenting as a metastatic lesion to the supraclavicular region is rare while most present with genitourinary symptoms. We present a case of a 50-year-old Caucasian male who presented with supraclavicular lymphadenopathy as the primary symptom. After excisional biopsy was consistent with adenocarcinoma, he underwent double endoscopy as well as computed tomography (CT) scans to aid in identifying the primary lesion which was unsuccessful while also presenting at follow-up with a tender nodule over the left shoulder. It was not until after restaining the biopsy specimen for prostate-specific antigen (PSA) and obtaining PSA levels did we identify the prostate as the primary site. This case report reiterates the importance of PSA levels and immunohistochemical staining on unknown neck masses.
Immunohistochemical, prostate, prostate-specific antigen, supraclavicular
INTRODUCTION
The presence of supraclavicular lymphadenopathy generally raises suspicion of neoplasms or inflammatory processes originating in the head and neck with approximately 1% of malignant solid tumors of the head and neck having their primary site below the clavicle with breast and melanoma being the most common [1]. The common prostate cancer rarely produces metastatic disease to the supraclavicular region. However, an increasing number of cases have been reported of primary adenocarcinoma of the prostate spreading to the supraclavicular region raising the index of suspicion [2-8]. Prostate cancer remains the most common non-cutaneous malignancy in American men and the third leading cause of cancer-associated mortality [9]. We present a case of metastatic adenocarcinoma of the prostate with initial presentation as the left-sided neck mass.
CASE REPORT
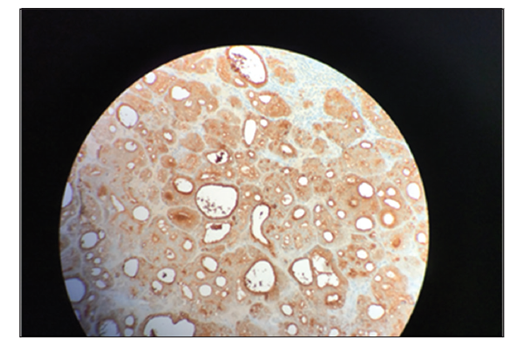
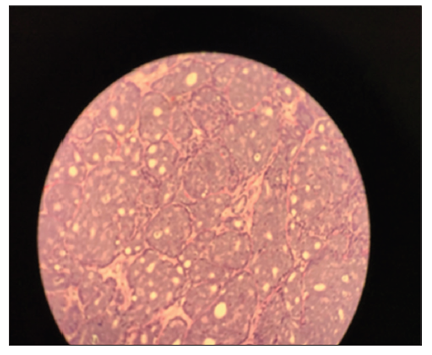
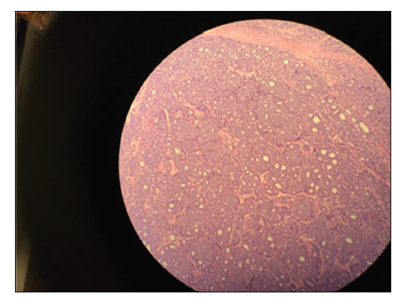
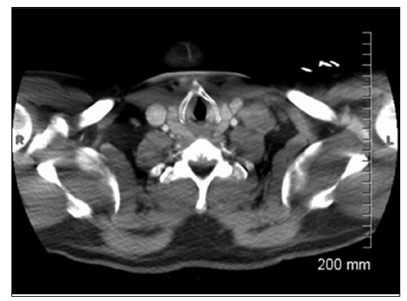
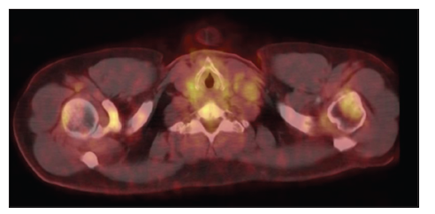
A 50-year-old Caucasian male presented to an outpatient surgery office with complaints of night sweats for a year as well as the left-sided cervical lymphadenopathy. He reported fatigue but endorsed no weight loss. Medical history was unremarkable, aside from hypothyroidism. Family history was significant for non-Hodgkin's lymphoma as well as breast cancer. Physical examination revealed an approximately 3 cm lymph node in the left supraclavicular space with no other palpable lymphadenopathies. He was then taken for excisional biopsy of this left supraclavicular lymph node, and initial pathology revealed adenocarcinoma [Figures 1-3]. He was then referred for endoscopy to rule out a gastrointestinal primary. The esophagogastroduodenoscopy was normal and colonoscopy revealed a hyperplastic polyp at 50 cm and a small rectal polyp. At the time of presentation for endoscopy, it was noted that the patient was complaining of the left shoulder pain and a palpable abnormality over his left acromioclavicular joint. Accordingly, a computed tomography (CT) scan [Figure 4] of his chest was obtained; however, it was not successful in identification of a primary lesion. He was referred for expert hematology and oncology consultation. Final pathology revealed metastatic cancer of prostate origin after immunohistochemical staining for prostate-specific antigen (PSA). He was started on Casodex, Lupron, and Taxotere. PSA was initially noted to be over 900. He subsequently underwent PET scan [Figure 5] that identified diffuse osseous and lymphatic involvement and probable subcutaneous involvement of the liver and lung parenchymal disease.
DISCUSSION
Adenocarcinoma of the prostate remains the highest incidence non-cutaneous neoplasia in males with an estimated 19% in 2017. About one in seven males will receive this diagnosis in their lifetime with 60% occurring after the age of 65 years. Of those diagnosed, it is estimated that 1 in 39 will die, falling behind lung, and colorectal malignancies [9,10]. In America, In America, African-American males have a slightly higher incidence and mortality rate than caucasian males. The incidence increased rapidly in the 1990s due to the initiation of screening for prostate cancer but declined over the last several years [11]. Of note, the United States Preventive Services Task Force longer recommends routine screening for prostate cancer due to no significant reduction in mortality [12].
The most common presentation is an asymptomatic patient with an incidental finding on routine digital rectal examination or an elevated PSA, or voiding difficulties. Other signs include hematuria, urinary retention, bone pain, and perineal pain [4].
Findings from the CONCORD-2 study showed that the most significant predictor of mortality in prostatic adenocarcinoma was the presence of distant metastases [11]. This correlates with a study performed at autopsy of 1589 patients by Bubendorf et al [13]. The 5-year survival of local and regional disease being 99.9% and 93.7%, respectively, but falls significantly to < 30% with distant metastatic disease in all races. Prostate cancer most commonly spreads to regional lymph nodes and axial skeleton followed by the lungs, liver, bladder, adrenal glands, and kidneys. Lymphatic spread beyond the pelvic cavity and retroperitoneum are uncommon [2-4,7]. Prostate cancer metastasis to supraclavicular nodes is quite rare with an estimated incidence of < 1% [7,14]. In a review of 11 cases of supraclavicular lymphadenopathy due to primary prostatic adenocarcinoma, Jones and Anthony demonstrated that all cases involved the left side (Virchow's node)[6]. These findings are supported by other case reports [4,7,14].
Multiple theories for the unorthodox spread of prostate cancer to supraclavicular lymph nodes have been proposed. One such theory is through hematogenous spread through Batson's venous plexus which allows communication of deep pelvic veins with thoracic veins [2,3]. However, this theory does not explain the significant bias toward the left-sided lesions. Park et al. proposed that the left bias maybe be due to spread through rich lymphatic network of the retroperitoneum to the cisterna chyli and from there to the thoracic duct on the left side [2]. This theory appears to be consistent with other reports [3,4,13].
Any neck mass in a patient over 40 years old should raise suspicion of malignancy as Balecki et al. found malignancy to be the most common cause in this age group in a review of 630 cases [15]. The vast majority of these malignancies have origins within the head and neck with < 1% originating below the clavicle [1]. However, due to the increasing number of reports of metastatic prostate cancer to the supraclavicular region, multiple studies recommend including adenocarcinoma of the prostate in the differential for supraclavicular lymphadenopathy of unknown origin. Diagnosis should be attained by immunohistochemical staining of biopsy with PSA stain [2-4,6,8].
CONCLUSION
Although the differential diagnosis is broad, prostate origin must be entertained in an elderly male presenting with supraclavicular lymphadenopathy. Metastatic cancers of the neck are more commonly from a squamous cell origin. In this case, we presented a patient with progressively enlarging the left supraclavicular lymphadenopathy. The importance of immunohistochemical staining with PSA cannot be understated.
REFERENCES
- Sagheb K, Menz A, Albrich S, Taylor K, Hess G, Walter C. Supraclavicular metastases from distant primary solid tumors: A retrospective study of 41 years. J Maxillofac Oral Surg 2017;16:152-7.
- Park E, Stroie F, McArdle B, Psutka S. Metastatic adenocarcinoma of prostate presenting as supraclavicular and bulky generalized lymphadenopathy with a benign digital rectal exam. Urol Case Rep 2017;13:128-30.
- Arumugam S, Kanakasabapathy S, Farman MJ. Combined androgen blockade responsive prostate carcinoma with extensive nodal metastases with Virchow's node. J Evol Med 2017;6:661-4.
- Lin YY, Lin DS, Kang BH, Lin YS. Neck mass as the first presentation of metastatic prostatic adenocarcinoma. J Chin Med Assoc 2011;74:570-73.
- Wang HJ, Chiang P, Peng J, Yu T. Presentation of prostate carcinoma with cervical lymphadenopathy: Report of 3 cases. Chang Gung Med J 2004;27:840-4.
- Jones H, Anthony PP. Metastatic prostatic carcinoma presenting as left sided cervical lymphadenopathy: A series of 11 cases. Histopathology 1992;21:149-54.
- Davarci M, Gokce A, Guven ED, Yalcinkaya F, Esen H, Sevine A. Metastatic prostate adenocarcinoma presenting with supraclavicular lymphadenopathy: A report of two cases. Contemp Oncol 2012;16:53-5.
- Pinaquy J, Allard J, Cornelis F, Pasticier G, De Clermont H. Unusual lymph node metastasis of prostate cancer detected with 18F-flourocholine PET/CT. Clin Nucl Med 2015;40:e255-57.
- American Cancer Society. About Prostate Cancer 2017. Atlanta, GA: American Cancer Society; 2017.
- Siegel R, Miller K, Jemal A. Cancer Statistics 2017. Cancer 2017;67:7-30.
- Steele CB, LI J, Hueng B, Weir HG. Findings from CONCORD-2 study. Cancer 2017;123:5160-77.
- Moyer VA. On behalf of the U.S. preventive services task force. screening for prostate cancer: U.S. preventive services task force recommendation statement. Ann Intern Med 2012;157:120-34.
- Bubendorf L, Schopfer A, Wagner V, Sautar G, Moch H, Gaser TC. Metastatic patterns of prostate cancer: An autopsy study of 1589 patients. Human Pathol 2000;31:578-83.
- Hematpour K, Bennett CJ, Rogers D, Head CS. Supraclavicular lymph node: Incidence of unsuspected metastatic prostate cancer. Eur Arch Otorhinolaryngol 2006;263:572-4.
- Balikci HH, Gurdal MM, Ozkul MH, Uvacin O, Kara N. Neck masses: Diagnostic analysis of 630 cases in Turkish population. Eur Arch Otorhinolaryngol 2013;270:2953-58.