Broken Heart Syndrome: A Stress Response
A. H. Yurvati
Citation : Yurvati AH. Broken Heart Syndrome: A Stress Response. Asclepius Med Case Rep 2018;1(2):1-3.
Takotsubo cardiomyopathy, also known as broken heart syndrome, stress cardiomyopathy, or apical ballooning syndrome, is described as a type of emotional or physical stress response that may mimic acute coronary syndrome (ACS) or myocarditis. It is a form of reversible left ventricular dysfunction with characteristic apical ballooning, contributing to its' name, along with diagnostic proof on coronary catheterization or angiography of the absence of significant coronary artery stenosis classically expected in ACS. The damage seen is typically transient, appearing to completely resolve within months with very low percentage of long-term sequelae or recurrence.
Cardiomyopathy, Stress cardiomyopathy, Taktosubo cardiomyopathy
INTRODUCTION
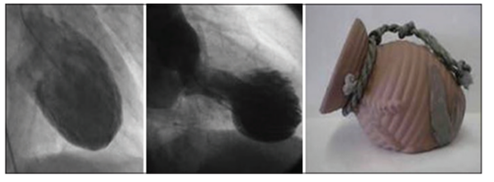
Takotsubo cardiomyopathy accounts for around 2% of all presentations suspicious for myocardial infarct or myocarditis [1]. It was first recognized in Japan, in 1990, so named for the Takotsubo pot [Figure 1] used to trap octopus and first reported in the United States in 1998 [2]. It is now widely recognized throughout much of the world, with publications rapidly increasing since 2001 [3]. Acute coronary syndrome (ACS) and myocarditis are important red flag differential diagnoses one must consider when there is suspicion for Takotsubo cardiomyopathy, as the latter is a diagnosis of exclusion, and the former must be ruled out.
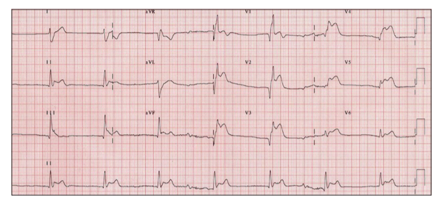
Although there has been lack of consensus, there are diagnostic criteria most recently proposed by the Mayo Clinic in 2004 [3]. They include (1) transient, most often stress induced, dysfunctional kinetic changes in the left midventricle involving >1 arterial distribution that may or may not have apical association; (2) diagnostic proof through cardiac catheterization or angiography of the absence of significant stenosis or plaque rupture; (3) new ST-segment or T-wave changes on electrocardiogram (ECG) reported to be without reciprocal changes [Figure 2] or serum cardiac enzyme elevation; and (4) prior rule out of myocarditis and/ or pheochromocytoma [3].
Patients present with the typical symptoms of ACS and/or myocarditis, such as chest pain, dyspnea, ST-segment and T-wave changes without reciprocal changes on ECG and, although not usually to the extent as true ACS, elevated serum cardiac enzymes, and catecholamines. While not directly naming Takotsubo cardiomyopathy, reported reversible left ventricular dysfunction in a case of pheochromocytoma [3]. Rarely, patients may even present with increasingly morbid ECG changes such as ventricular fibrillation and cardiogenic shock [4].
CASE REPORT
A 76-year-old Caucasian female presented to her primary care provider for a follow-up on recent complaints of shortness of breath and dyspnea on exertion, consistent with a diagnosis of pneumonia. The patient had completed a course of Levaquin and steroids, and she was given a ProAir inhaler to use as needed for shortness of breath. On review of systems, the patient continued to endorse productive cough, epigastric pain, and dysphagia, but she no longer endorsed fever or chills. The patient denied chest pain, palpitations, syncope, or near-syncopal events. Medical history was significant for dyslipidemia, hypertension, hypothyroidism, migraines, depression, gastroesophageal reflux disease, and cardiac diastolic dysfunction. Records suggested that the patient had an inferolateral myocardial infarct in the remote past, although the exact timing is unclear at present. Prior echocardiograms, with the most recent >1 year prior, were only significant for impaired diastolic dysfunction and mild tricuspid and mitral regurgitation. The most recent cardiac catheterization on record was from 4 years before presentation, which showed an ejection fraction (EF) of 60%, 20% blockage in the proximal and midleft anterior descending artery, and a 30% blockage in the midright circumflex artery. The patient has been postmenopausal for near 20 years, and her medications included Simvastatin, Losartan, Klor-Con, Synthroid, Imitrex, Bupropion, Protonix, and low-dose aspirin. Prior surgical and family history included gastric bypass surgery and coronary artery disease at an age < 60 years, respectively. Precise social history is currently unavailable, although there is mention of tobacco use of unspecified quantity or duration.
On physical examination, vitals were stable and otherwise only significant for decreased breath sounds and wheezing bilaterally. Cardiac examination was within normal limits, although the patient was recently sent for further studies due to previous findings by the patient's cardiologist of an irregular heart rhythm and I/VI systolic murmur at the left sternal border. Pertinent examinations and imaging include an ECG proving a 1st degree heart block and a computed tomography angiogram (CTA) of the chest showing mild atelectasis in the left lower lobe of the lung. This CTA also resulted in the discovery of a very large hiatal hernia in the midline and left lower chest to include much of the stomach, a large amount of intra-abdominal fat, and a small knuckle of the small bowel with no indications of obstruction or gangrene. The patient's cardiologist also ordered a Lexiscan nuclear stress test, which showed an EF of 57% and mild ST-segment changes in the inferior and lateral regions during stress periods, but it was interpreted as overall normal perfusion and function. Pulmonary function testing was also suggested, but the results are unavailable at this time.
The patient returned within 1 week complaining of chest pain and epigastric pain radiating to the back in addition to increased shortness of breath and dyspnea on exertion. These symptoms were aggravated by bending over, cold and hot liquids, fatty food intake, large meals, exercise, and heavy lifting, and they were mildly improved by the proton-pump inhibitor, Protonix. At this point, the patient was referred to a cardiothoracic surgeon, and it was decided that the patient would undergo a Belsey Mark IV through the left thoracotomy to repair the patient's large hiatal hernia.
Approximately one and 1½ months after the patient's prior episode of pneumonia, the Belsey Mark IV procedure was scheduled. The patient was cleared by cardiology and anesthesia before the procedure. The morning of the procedure, the pre-operative assessment, and line access proved uneventful, and there appeared to be no impediment to proceeding to the operating room (OR) for the hiatal hernia repair. The patient was brought to the OR by the surgical team, moved to the operating table, prepared, and successfully inducted under general anesthesia, although the official anesthesia record is currently unavailable. A double-lumen endotracheal tube was placed successfully, as the need may have arisen to deflate the left lung during the procedure. The patient was positioned in the left lateral recumbent position and safely secured in place. The patient was then prepped, first with chlorhexidine, then betadine soap and paint. Within 1-2 min after the surgical prep was completed, the patient became bradycardic and suddenly went into ventricular fibrillation. All parties were immediately notified and the emergency response system was activated. As the team was attempting to reposition the patient to supine, anesthesia was attempting to do chest compressions while in the recumbent position. In the meantime, the patient, again suddenly, self- converted backs to sinus rhythm. The morbid heart rhythm only lasted for, at most, 20 s before self-correcting.
The hiatal hernia repair was immediately canceled, to be rescheduled in the future. Anesthesia was reversed, and the patient was taken for cardiac catheterization shortly thereafter. The results of the procedure showed < 50% blockages in any given coronary artery, leading to the diagnosis of Takotsubo cardiomyopathy.
DISCUSSION
As previously mentioned, Takotsubo cardiomyopathy may cause something of a conundrum for the physicians initially assessing the patient, as it nearly always presents with great similarity in physical examination, laboratory studies, and ECG to an acute myocardial infarction. It has a propensity to affect postmenopausal women, typically >50 years old, and seems to affect men only 10% of the time [1]. Familial inheritance has yet to have been proven and seemingly intuitive risk factors, such as hypertension, diabetes mellitus, smoking, and dyslipidemia, actually do not apply to this condition [2]. Only up to 5% of patients eventually have recurrence of the syndrome[4].
When considering that the diagnostic criteria include that damage must cross into at least two coronary artery distributions, it is no surprise that acute heart failure with resultant pulmonary edema and respiratory distress or failure can occur. At the worst, ventricular wall rupture is a significant concern, so patients should be admitted to the intensive care unit for up to 24 h [3]. Beta-blockers, angiotensin-converting enzyme inhibitors (ACE-I), and brief use of anticoagulants to protect against stroke are typically used in these situations, as beta-blockers and ACE-Is are cardioprotective and encourage quicker healing of the damaged myocardium [3].
The excessive levels of catecholamines released in times of emotional and physical stress, with neoplasms such as pheochromocytomas and in the exogenous dosing of adrenergic receptor stimulators become toxic to the cardiac myocytes, leading to cytological changes. Toxicity is thought to be the result of high intracellular Ca2+ concentrations secondary to adrenergic activation coupled with the naturally increased concentration of adrenergic receptors in the left ventricular apex [3]. In myocardial biopsies, there appears to be interstitial infiltrates consisting predominantly of leukocytes, mononuclear lymphocytes and macrophages, and contraction bands with myocardial fibrosis [1]. Occasionally, biopsies present with myocyte necrosis dissimilar from coagulation necrosis expected in cases of ACS [3].
Two physiologic mechanisms have been discussed. The first is a spontaneous multivessel coronary vasospasm, thought to be brought on by the increased load of catecholamines previously discussed. The second is a vulnerable plaque that ruptured and thrombosed within a coronary artery. The only downfall in the second theory is the region of damage in Takotsubo cardiomyopathy crosses more than one arterial distribution, which does not align with the pathophysiology of a thrombosed coronary artery. The former seems to be more likely the case.
CONCLUSION
This patient was a postmenopausal woman who experienced recent physical stress and had a somewhat significant cardiac history. While she was rightly cleared by cardiology, she had not had a recent echocardiogram, a coronary angiogram, or cardiac enzymes drawn before surgery. She had the hiatal hernia, which is a perfectly rational cause for chest pain and dyspnea, and she also had a recent, non-concerning nuclear stress test that would normally remove any suspicion of more serious cardiac injury. It is unclear if there is anything different that would or should have been done in this case, as well as there is no way to know if it was the increased stress from anesthesia induction or fear of surgery that led to this episode of ventricular fibrillation. It does seem apparent that the physical stress was undertaken during the previous episode of pneumonia. This case may refresh the awareness of other patients with similar history and presentation, and perhaps, help to keep this diagnosis in the back of the mind for a patient who has experienced recent physical and emotional stress.
References
- Salim SV, Khan AN, Mendoza CE, Ferreira AC, De Marchena E. Takotsubo cardiomyopathy, or broken-heart syndrome. Tex Heart Inst J 2007;34:76-9.
- Sharkey SW, Lesser JR, Maron BJ. Takotsubo (Stress) cardiomyopathy. Circulation 2011;124:E460-2.
- Akashi YJ, Goldstein DS, Barbaro G, Ueyama T. Takotsubo cardiomyopathy: A new form of acute, reversible heart failure. Circulation 2008;118:2754-62.
- Gianni M, Dentali F, Grandi AM, Sumner G, Hiralal R, Lonn E. Apical ballooning syndrome or takotsubo cardiomyopathy: A systematic review. Eur Heart J 2006;27:1523-9.