Prolonged Pleural Effusion following Liver Biopsy in a 10-Year-Old Girl
K. Karavdic1, V. Sarajlic2, E. Kovac-Vidakovic3, M. Melunovic3
2.Department of Radiology, Institute for Radiology, Clinical Center of University Sarajevo, Bolnicka 25, 71000 Sarajevo, Bosnia and Herzegovina.
3.Department for Gastroenterohepatology, Pediatric Clinic, Clinical Center of University Sarajevo, Patriotske lige 81, 71000 Sarajevo, Bosnia and Herzegovina.
Citation : Karavdic K, Sarajlic V, Kovac-Vidakovic E, Melunovic M. Prolonged Pleural Effusion following Liver Biopsy in a 10-Year-Old Girl. Asclepius Med Case Rep 2018;1(2):1-3.
Pleural effusions in patients with liver disease are common. Bilious pleural effusion can occur following percutaneous biopsy if the pleura is traversed. We reported the case of a 10-year-old girl who had a liver biopsy. After this procedure, the girl had a pleural effusion during the 20-day period we were treated with the chest tube. After this period, the chest tube was removed and the patient continued conservative gastroenterological treatment for liver cirrhosis.
Biopsy, effusion, liver
INTRODUCTION
Percutaneous liver biopsy is the gold standard for grading and staging of liver disease which has been used for >100 years. Pulmonary complications post-liver biopsy is considered to be rare, and this can occur if needle biopsy passed in the costophrenic angle above the reflection of between the parietal and the visceral pleura. The patients can develop pneumothorax and hemothorax and also hydrothorax can be developed in cirrhotic patient with ascites by passage of ascitic fluid through the puncture site on diaphragm [1]. The incidence of pneumothorax and/or pleural effusion occurs in the range of 0.08-0.28% and the symptoms usually mild and pulmonary collapse not exceeding 10% [2]. Hemothorax post-liver biopsy is also rare with incidence of 0.18-0.49% and this can be managed conservatively and rarely need thoracotomy [3].
CASE REPORT
A girl, 10 years old, received at the gastroenterohepatology department of pediatric clinic due to the problems which started 3 years ago. The mother complained that her daughter was weak in weight. The girl complained of a pain in the lower part of the stomach that had ripped to the right of the arcus costalis, which appeared in longer walking or running. Microbiological analysis revealed a parasite in the stool. She has elevated body temperature, up to 39°C, once monthly. There are elevated values of liver enzymes (transaminases). Previous diagnostic methods exclude mononucleosis and brucellosis.
Physical examination of the abdomen palpated the liver to 2 cm. Ultrasound was done: The liver expressed rough and inhomogeneous structures of parenchyma. Laboratory reception values: Elevated transaminase values, aspartate aminotransferase (AST) = 88 U/L (reference values 15-37 U/L), alanine aminotransferase (ALT) = 161 U/L (reference values 30-65 U/L), gamma-glutamyl transferase = 119 (5-55 normal values), and normal bilirubin values.
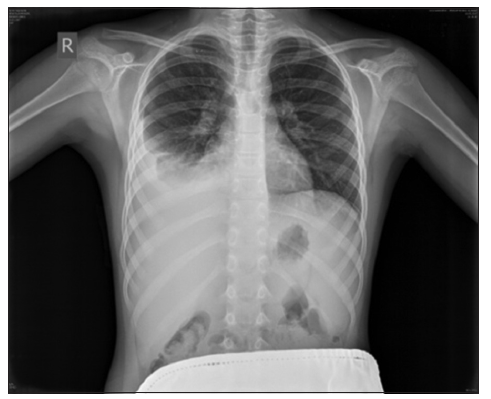
Ultrasound of the thyroid gland: Both glandular lobes are the appropriate positions, the parenchyma of both lobules is a diffuse coarse structure with no visible signs of increased vascularization. The volume of the right lobule is about 2.25 ml (13 ml X 11 ml X 30 ml) and the left lobus 2 ml (12 ml X 10 ml X 31 ml), the thyroid gland is volumetric normal. Chest X-ray before procedure was normal [Figure 1].

She was referred from pediatric clinic to radiology department for liver biopsy. The indication for biopsy was diffuse liver disease and the laboratory findings. The biopsy was performed under the ultrasound guidance, with the patient in supine position and deep analgosedation. The liver was of normal size, and the biopsy site was ninth intercostal space, in the medioaxillary line. The coaxial 18G biopsy needle was used (SuperCore Biopsy Instrument with Coaxial Introducer Needle, 18ga X 9 cm, Argon Medical Devices, USA) and three tissue samples were taken for pathology analysis. The procedure went smoothly with only one pass through the liver capsule, the patient woke-up soon after the procedure and sent back to pediatric clinic.
Only a few hours later, the patient started complaining about pain and short breath, and the chest X-ray revealed a pleural effusion on the right site [Figure 2]. The computed tomography (CT) finding confirmed that and showed a more volatile liver. The liver parenchyma is rough. The chest CT shows extensive pleural effusion on the right side. Pleural effusion had characteristics of an exudate, with high level of lactate dehydrogenase (LDH) 247 U/L, total bilirubin 14.5 nmol/L, cholesterol 2.0 mmol/L, and triglycerides 0.54 mmol/L. The presence of bilirubin confirmed that it was a bilious effusion, caused by the trauma of the pleura during the biopsy procedure. Pathohistological findings of liver biopsy showed cirrhosis of the liver.
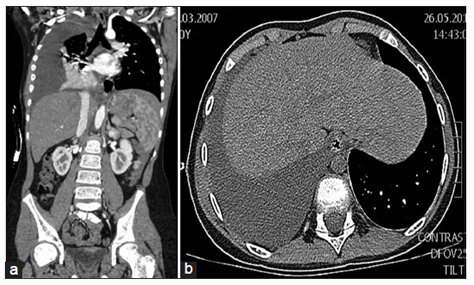
The CT finding shows a more volatile liver. The liver parenchyma is rough. The chest CT shows extensive pleural effusion on the right side.
Figure 3 CT finding shows a more volatile liver, liver parenchyma is rough and extensive pleural effusion on the right side. Pleural effusion had characteristics of an exudate, with high level of LDH 247 U/L, total bilirubin 14.5 nmol/L, cholesterol 2.0 mmol/L, and triglycerides 0.54 mmol/L. The presence of bilirubin confirmed that it was a bilious effusion, caused by the trauma of the pleura during the biopsy procedure. It was understood as a post-biopsy complication, caused by inadvertent injury of pleura by the biopsy needle. Pathohistological findings of liver biopsy showed cirrhosis of the liver.
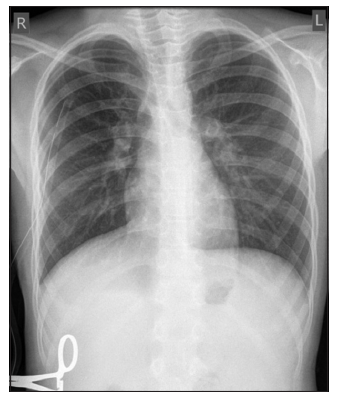
The pleural puncture is performed and about 200 ml of clear yellow liquid contents are obtained. The control X-ray again shows radiological signs of pleural effusion and is indicated by the chest tube placement in general anesthesia. The overall condition is satisfactory and the daily secretion on the chest tube is about 400-500 ml. Control chest X-ray showed a satisfactory finding [Figure 4].
An antibiotic therapy of cefazolin is ordered, the fluid content is microbiologically sterile. Pleural effusion had characteristics of an exudate, with high level of LDH 247 U/L, total bilirubin 14.5 nmol/L, cholesterol 2.0 mmol/L, and triglycerides 0.54 mmol/L. The presence of bilirubin confirmed that it was a bilious effusion, caused by the trauma of the pleura during the biopsy procedure. It was understood as a post-biopsy complication, caused by inadvertent traversion of pleura by the biopsy needle.
Laboratory values that are showed lower in serum albumin values = 24 g/l are controlled and human albumin is ordered for 20%, 3 days. The values of transaminases were decreased by AST = 59 and ALT = 84. Pediatric endocrinologist administered levothyroxinum natricum and 25 mg, due to the suspicion of hypofunction of the thyroid gland.
The amount of liquid on the chest tube was initially 400-500 ml daily. Gradually decreasing order after 20 days of drainage completely stopped and the thoracic drain was removed out.
Pathohistological findings of liver biopsy showed cirrhosis of the liver. Pediatric gastroenterologist orders silymarin 2 X 1 caps to regenerate liver function and Vitamin E. The patient continued to be treated on the gastroenterological department of pediatric clinic for liver cirrhosis caused by unknown cause.
DISCUSSION
Erlich is credited with the first liver aspiration in 1883, and subsequently, the first percutaneous liver biopsy for diagnostic purposes was reported in 1923.[4] The technique has been modified since then, and over the past 50 years, it has become a central investigation of hepatic disease. The low mortality (0.01-0.17%) and the relatively low morbidity of this procedure have meant that liver biopsy has become widely used [5]. The mortality and morbidity are low (0.01-0.17%) and due to that liver biopsy has become widely used. The puncture of lung, colon, kidney, and gallbladder together with pneumothorax, pleural effusion, and subcutaneous emphysema are well-recognized complications, which rarely require intervention [6].
The term bilothorax was first coined by Williams in 1971 in a case of blunt trauma resulting in a biliary fistulalization into the pleural space [7]. Fistula formation can occur through multiple etiologies. Bile salts are inherently alkaline and caustic to pleural and peritoneal tissue, corroding the posterior recess of the diaphragm in cases with bile leakage even without iatrogenic perforation. Diaphragmatic injury, either through blunt trauma or iatrogenic causes, can form a connection from the peritoneal to pleural space [8].
Conventional imaging modalities including chest radiograph, ultrasound, and CT can be used in establishing an accurate clinical diagnosis. Complete emergent drainage of a bilothorax is essential to prevent empyema and fibropurulent effusions.
CONCLUSION
- The diagnosis of pleural effusion requires a high degree of clinical suspicion after liver biopsy and should be considered after liver biopsy.
- The most specific finding is a pleural fluid to serum ratio of bilirubin >1.0.
- Complete emergent drainage of a pleural effusion after liver biopsy and administration of broad-spectrum antibiotics is essential to prevent empyema and fibropurulent effusions.
- Liver biopsy is the gold standard method and definitive diagnostic test for difficult cases of liver diseases.
References
- Zamcheck N, Sidman RI. Liver biopsy I. Its use in clinical and investigative medicine. N Engl J Med 1953;249:1020.
- . Chuah SY. Liver biopsy-past, present and future. Singapore Med J 1996;37:86-90..
- Campbell MS, Jeffers LJ, Reddy KR. Liver biopsy and laparoscopy. In: Schiff L, Schiff ER, editors. Diseases of the Liver. 10th ed. Philadelphia, PA: Lippincott William and Wikins; 2007. p. 62-83.
- Bingel A. Ueber die parenchympunktion der leber. Verh Dtsch Ges Inn Med 1923;35:210-2.
- Stotland BR, Lichtenstein GR. Liver biopsy complications and routine ultrasound. Am J Gastroenterol 1996;91:1295-6.
- Majid AA. Hemorrhage from the diaphragm: An unusual cause of hemothorax after liver biopsy. Am J Gastroenterol 1990;85:104-5.
- Chahal PS, Ready J. Hemothorax after percutaneous liver biopsy: An unusual complication. Am J Gastroenterol 2002;97:1068-9.
- Yeo WT, Tan LK, Dan YY, Wai CT. Delayed bleeding after liver biopsy: A dreaded complication. Singapore Med J 2008;49:76-80.