Synchronous Primary Cancers of the Endometrium and Ovary and Breast Cancer: A Case Report
Emre Kole, Merve Kole
Citation : Kole E, Kole M. Synchronous Primary Cancers of the Endometrium and Ovary and Breast Cancer: A Case Report. Asclepius Med Case Rep 2018;1(2):1-3.
Pleural effusions in patients with liver disease are common. Bilious pleural effusion can occur following percutaneous biopsy if the pleura is traversed. We reported the case of a 10-year-old girl who had a liver biopsy. After this procedure, the girl had a pleural effusion during the 20-day period we were treated with the chest tube. After this period, the chest tube was removed and the patient continued conservative gastroenterological treatment for liver cirrhosis.
Biopsy, effusion, liver
INTRODUCTION
Multiple primary cancers are usually defined as synchronous malignancies if the interval between them is less or equal to 6 months. If the interval is longer, the tumors are called metachronous. Besides this, to be able to characterize the multiple primary malignancies (MPM), diagnosis criteria according to Warren and Gates must meet these three criteria: (a) Confirmation of malignant histology on index and secondary tumor; (b) there should be minimum 2-cm distance of normal mucosal between tumors. If the tumor appears in the same location, the diagnostic interval must be 5 -year apart; and (c) the probability that one of the tumors is metastasized from the other must be excluded [1,2]. In the same case, the incidence rate of multiple primary malignant tumors ranged from 0.7% to 11.7% [3]. The formation of the second tumor occurs as a result of a series of complex interactions. The first tumor increases the risk of developing secondary tumor. Furthermore, smoking, alcohol intake, environmental factors, and genetic mutations increase the risk of developing secondary tumor [4]. Determination of these cases is important to elucidate the underlying etiology.
CASE REPORT
A 51-year-old, gravida 3, parity 3 patient presented to the polyclinic with the complaint of postmenopausal bleeding. Ultrasonographic assessment of the uterus revealed that the uterus size was increased. The right and left ovaries were normal size. Endometrial thickness was 17 mm. The story of the patient revealed that her last menstrual period was 7 years ago, and after this, she did not have any bleeding. Her medical history showed a postmenopausal with atypical hyperplasia. The vital signs of the patient were stable. There was no known disease in her medical history, except for chronic hypertension.
Previously, she did not undergo any surgical intervention except that she had two cesarean deliveries. The patient had no history of smoking and drug use. The physical examination of the patient revealed that the abdomen and other system examinations were normal.
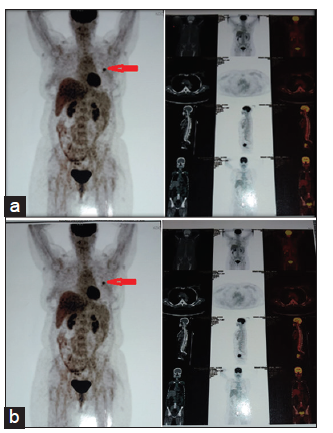
Vaginal speculum examination showed normal cervical and vaginal appearance, and active vaginal bleeding was observed. Therapeutic curettage was performed. Complete blood count performed in laboratory examination showed that hemoglobin was 9.3 g/dl, platelet was 312000 mm3, and complete urinalysis testing result was normal. The patient was invited to the polyclinic to have cervical screening tests (smear tests). Smear results were reported as negative for intraepithelial lesion or malignancy. Diagnostic endometrial curettage results were endometrial polyp. The patient was administered levonorgestrel-releasing intrauterine system. Due to her prolonged heavy bleeding, her anemia could not be corrected, and surgical decision was made. The assessment of the patient during operation revealed that the uterus was 12 weeks and gestational size, right and left ovaries, and tubes had normal appearance. Total abdominal hysterectomy and bilateral salpingo-oophorectomy were done. The patient's post-operative follow-up proved that general condition of the patient was good and did not have any post-operative complications, and the patient was discharged. Pathology result was observed as complex atypical hyperplasia of the endometrium-based focal well-differentiated Grade I endometrial adenocarcinoma. The tumor did not exceed the endometrium' no myometrial invasion or cervical invasion was identified. The left ovary was reported as a moderately differentiated granulosa cell tumor extending 9 mm until the capsule but not exceeding it. Then, 3 months later, the patient underwent total body positron emission tomography (PET). As a result of the patient's PET performed after 3 months, on monitoring mass in the left upper outer quadrant of the breast, lumpectomy and sentinel lymph node biopsy were performed. Pathological result showed high-grade invasive ductal carcinoma, and sentinel lymph node biopsy result was observed as tumor emboli. ER + and PR+ ve HER-2/ neu 4B5 + were measured. The patient was given 4 cycles of doxorubicin + cyclophosphamide and paclitaxel. Afterward, after 33 cycles of RT treatment, the patient was given follow-up care. PET imaging was performed and observed normal [Figure 1].
DISCUSSION
In relation to various factors such as increase in the number of treatment options, surveillance increase in some types of cancer, increased use of cytotoxic agents, and ionizing radiation, the prevalence of MPM has increased.
In the literature, studies in synchronous and metachronous tumors are generally retrospective studies. Especially according to Warren and Gates criteria, it is classified as synchronous or metachronosis. The prevalence of multiple primary tumors was reported as 0.73% in the study of Haddow et al [5-10]. Synchronous endometrial and over-cancer have been reported in 5-10% of all patients in the literature [11,12].
We aimed to present this study as the first case of the synchronous occurrence of breast cancer with this tumor. Endometrial cancer is the most common form of female pelvic malignancy with a lifetime risk of 4%. It is usually diagnosed at an early stage. It constitutes only 2% of cancer-related deaths and has a good prognosis. The most common age at diagnosis is 65 and 75 years, and the median age is 69 years. On the other hand, approximately 10% of women diagnosed with endometrium cancer are under 50 years of age. In women with endometrium cancer, the prevalence of synchronous ovarian carcinoma risk and hereditary non-polyposis colon cancer syndrome has increased [13-15].
In a surveillance, epidemiology, and end results program database analysis, synchronous cancers represented < 3% of the 56,986 epithelial ovarian cancer cases [16]. In literature review, synchronous breast, ovarian, and endometrial cancer have not yet been reported. Genetic and epigenetic factors are regarded as important in the pathologic physiology of carcinoma. Genetic research to be performed on these patients plays an important role in determining the etiology.
As a result, the incidence of multiple primary tumors has increased with increased survival of cancer patients and life expectancy worldwide, environmental or occupational exposures to chemical and physical agents. In these cases, we believe that multidisciplinary approach, especially genetic research, will lead to the better understanding of the pathophysiology of cancer.
References
- Aydiner A, Karadeniz A, Uygun K, Tas S, Tas F, Disci R, et al. Multiple primary neoplasms at a single institution: Differences between synchronous and metachronous neoplasms. Am J Clin Oncol 2000;23:364-70.
- Derwinger K, Gustavsson B. A study of aspects on gender and prognosis in synchronous colorectal cancer. Clin Med Insights Oncol 2011;5:259-64.
- Coleman MP. Multiple primary malignant neoplasms in england and wales, 1971-1981. Yale J Biol Med 1986;59:517-31.
- Ng AK, Kenney LB, Gilbert ES, Travis LB. Secondary malignancies across the age spectrum. Semin Radiat Oncol 2010;20:67-78.
- Hemminki K, Boffetta P. Multiple primary cancers as clues to environmental and heritable causes of cancer and mechanisms of carcinogenesis. IARC Sci Publ 2004;157:289-97.
- Wynder EL, Mushinski MH, Spivak JC. Tobacco and alcohol consumption in relation to the development of multiple primary cancers. Cancer 1977;40:1872-8.
- Carey TE. Field cancerization: Are multiple primary cancers monoclonal or polyclonal? Ann Med 1996;28:183-8.
- Haddow AJ, Boyd JF, Graham AC. Multiple primary neoplasms in the Western hospital region, Scotland: A survey based on cancer registration data. Scott Med J 1972;17:143-52.
- Warren S, Gates O. Multiple primary malignant tumors: A survey of the literature and statistical study. Am J Cancer 1932;16:1358-414.
- Haddow AJ, Boyd JF. Multiple primary neoplasms in the western hospital region, scotland: A survey based on cancer registration data. Scott Med J 1972;17:143-52.
- Chui MH, Ryan P, Radigan J, Ferguson SE, Pollett A, Aronson M, et al. The histomorphology of lynch syndrome-associated ovarian carcinomas: Toward a subtype-specific screening strategy. Am J Surg Pathol 2014;38:1173-81.
- Heitz F, Amant F, Fotopoulou C, Battista MJ, Wimberger P, Traut A, et al. Synchronous ovarian and endometrial cancer - an international multicenter case-control study. Int J Gynecol Cancer 2014;24:54-60.
- Jamison PM, Altekruse SF, Chang JT, Zahn J, Lee R, Noone AM, et al. Site-specific factors for cancer of the corpus uteri from SEER registries: Collaborative stage data collection system, version 1 and version 2. Cancer 2014;120 Suppl 23:3836-45.
- Oranratanaphan S, Manchana T, Sirisabya N. Clinicopathologic variables and survival comparison of patients with synchronous endometrial and ovarian cancers versus primary endometrial cancer with ovarian metastasis. Asian Pac J Cancer Prev 2008;9:403-7.
- Rodriguez AM, Schmeler KM, Kuo YF. Disparities in endometrial cancer outcomes between non-hispanic white and hispanic women. Gynecol Oncol 2014;135:525-33.
- Williams MG, Bandera EV, Demissie K, Rodriguez-Rodriguez L. Synchronous primary ovarian and endometrial cancers: A population-based assessment of survival. Obstet Gynecol 2009;113:783-9.