A Rare Case Report: Partial Molar Pregnancy with a Live Fetus
Emre Kole, Merve Kole, Gulseren Yucesoy
Citation : Kole E, Kole M, Yucesoy G. A Rare Case Report: Partial Molar Pregnancy with a Live Fetus. Asclepius Med Case Report 2018;1(1):1-2.
Twin molar pregnancy with a hydatidiform mole and a coexisting live fetus is a rare occasion. Molar pregnancies are generally associated with vaginal bleeding, normally elevated beta-human chorionic gonadotropin, hyperthyroidism, singlet lutein cysts, and preeclampsia. However, in partial molar pregnancy, these cases are less often observed. Due to the delayed removal of molar tissue, the risk of gestational trophoblastic neoplasm is another source of concern. In the present study, we present a case of partial molar pregnancy and live fetus, together with hyperthyroidism and abdominal hemorrhage, resulting in molar pregnancy abortion.
Hyperthyroidism, live fetus, partial hydatidiform mole, twin molar pregnancy
INTRODUCTION
Gestational trophoblastic diseases caused by fetal trophoblastic tissue are a heterogeneous group of neoplasia. Mole hydatiform is a benign form of the disease with a variable potential for malignant transformation. In mole hydatiform, according to histocytopathological and clinical structure, it is classified into two groups as partial or complete mol. Partial form is characterized by villous edema and trophoblastic hyperplasia at mild, moderate, and focal level [1,2] In many partial mole cases, as a result of insemination of one ovum with two sperms, generally fetal chromosomal triploid is present in most of them (while two-thirds are 47 XXX and one-third is 47 XXX). Partial molar association with a live fetus is seen in 0.005-0.01% of pregnancies [3-5]. In these cases, miscarriage (also known as spontaneous abortion) rate is high. However, 40% of cases may result in live births. In cases that want to continue their pregnancy, since the risk of gestational trophoblastic neoplasia is not more than 21% and the risk will not change as the pregnancy progresses, the pregnancy can be allowed to continue on condition that the fetus and the mother are monitored closely [6].
CASE REPORT
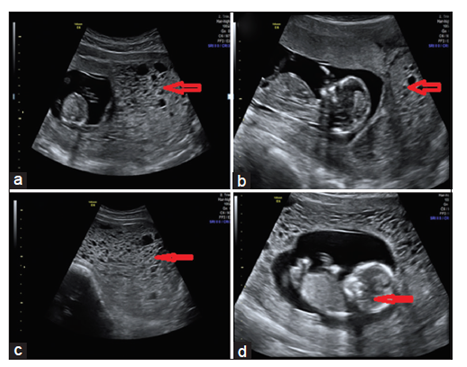
During her policlinic control, in our 21 years 14 weeks and 2 days primigravida, a dichorionic diamniotic twin pregnancy was observed on obstetric ultrasonography. While one of the twin pregnancies was a live fetus, its twin was discovered to be molar pregnancy [Figure 1]. There was no vaginal bleeding in the patient complaining of abdominal pain. The vital signs of the patient were stable. There was no known chronic disease in her medical history. Previously, she did not have any operations. The patient had no history of smoking and drug use. Her blood type was Rh positive. The physical examination of the patient revealed that the abdomen and other system examinations were normal. In the abdominal examination, the abdomen was soft, unresistant, and tender and the uterus was the size of 24 gestational weeks. Vaginal examination performed with speculum showed cervical os closed, no bleeding, and no amnion fluid. In the laboratory, complete blood count showed that hemoglobin was 11.5 g/dl, platelet was 150,000 mm3, and complete urine test was normal. Beta-human chorionic gonadotropin (hCG) level was 554,810 mIU/mL. Thyroid function tests were compatible with thyrotoxicosis in thyroid-stimulating hormone: 0.005 mIU/L (n: 0.465-4.6), FT3: 9.02 pg/mL (n: 2.79-5.27), and FT4: 3.47 ng/dL (n: 0.78-2.19). No features were found in the PAAC graphic image. The patient describing abdominal pain was admitted for observation. On the 4th day of admission, obstetric ultrasonography was performed on a patient who had sudden onset of abdominal pain and severe vaginal bleeding. In vaginal examination, a live fetus was observed. Furthermore, its twin hydatidiform mole was observed to be aborted. Surgical intervention with blood transfusion was decided to be applied to the gravida who had abundant vaginal bleeding. Under general anesthesia, after the aspiration of the moles by vacuum curettage accompanied by an infusion of oxytocin to the patient, evacuation curettage was done to its twin. Surgery was terminated once bleeding was not observed. On the 2nd post-operative day of the patient, when beta-hCG level dropped to 178456, and since the active bleeding could not be observed, she was put under the clinical observation. Histopathology of the patient was reported as partial molar hydatidiform mole. During follow-up, when post-operative beta-hCG level did not become negative but plateaued. Intramuscular injection of folinic acid (0.1 mg/kg for 4 cures with 2 days intervals) with methotrexate (0.1 mg/kg 4 cures with 2 day intervals) was administered. When the follow-up Beta-hCG got negative, the patient was treated with monthly follow-up.
DISCUSSION
40% of the partial molar cases can be recognized despite the paralytic molar, obstetric ultrasonography. Rarely, a placenta and a fetus are present in these cases [6]. Partial moles usually have an abnormal karyotype. Partial mole and a live fetus with a triploid chromosome are usually present with fetal anomalies [7]. Especially if pregnancy is desired, the management of live fetal in molar pregnancies is difficult. Vejerslev noted that ultrasonographic examination of the placenta and fetal karyotype could be achieved after prenataltesting [8]. In this case, prenatal tests could not be performed because an urgent surgery decision was made. Jones and Lauersen, even in the presence of a live fetus, suggest therapeutic abortion in partial molar cases [9]. Progression of mole hydatidiforms to malignant disease is variable. While in the complete mole with coexisting fetus, it is 56-62%, and in partial moles with a viable fetus, it is %4 [10]. Although live fetus births have been reported in the literature, to avoid catastrophic complications such as preeclampsia and lifethreatening bleeding, termination of the pregnancy should be considered as the first option.
REFERENCES
- Szulman AE, Surti U. The syndromes of hydatidiform mole. II. Morphologic evolution of the complete and partial mole. Am J Obstet Gynecol 1978;132:20-7.
- Watson EJ, Hernandez E, Miyazawa K. Partial hydatidiform moles: A review. Obstet Gynecol Surv 1987;42:540-4.
- Sauerbrei EE, Salem S, Fayle B. Coexistent hydatidiform mole and live fetus in the second trimester: An ultrasound study. Radiology 1980;135:415-7.
- Ohama K, Ueda K, Okamoto E, Takenaka M, Fujiwara A. Cytogenetic and clinicopathologic studies of partial moles. Obstet Gynecol 1986;68:259-62.
- McDonald TW, Ruffolo EH. Modern management of gestational trophoblastic disease. Obstet Gynecol Surv 1983;38:67-83.
- Lindholm H, Flam F. The diagnosis of molar pregnancy by sonography and gross morphology. Acta Obstet Gynecol Scand 1999;78:6-9.
- Guven ES, Ozturk N, Deveci S, Hizli D, Kandemir O, Dilbaz S, et al. Partial molar pregnancy and coexisting fetus with diploid karyotype. J Matern Fetal Neonatal Med 2007;20:175-81.
- Vejerslev LO. Clinical management and diagnostic possibilities in hydatidiform mole with coexistent fetus. Obstet Gynecol Surv 1991;46:577-88.
- Jones WB, Lauersen NH. Hydatidiform mole with coexistent fetus. Am J Obstet Gynecol 1975;122:267-72.
- Bruchim I, Kidron D, Amiel A, Altaras M, Fejgin MD. Complete hydatidiform mole and a coexistent viable fetus: Report of two cases and review of the literature. Gynecol Oncol 2000;77:197-202.