Surgical Management of an Intraparenchymal Chest Tube with Thoracoplasty and Primary Lung Repair
Katelin T. Holmes1, A. H. O-Yurvati2
2.Department of Surgery, Medical City Fort Worth Medical Center, Fort Worth, Texas, USA.
Citation : Holmes KT, O-Yurvati AH. Surgical Management of an Intraparenchymal Chest Tube with Thoracoplasty and Primary Lung Repair. Asclepius Med Case Rep 2018;1(2):1-3.
Intraparenchymal placement of a chest tube into the lung is a known complication of tube thoracostomy. Patients with a history of prior lung surgery may be at a higher risk for such an event. The surgical management for this type of iatrogenic injury is rarely described in the literature. This case study illustrates a patient with a history of previous lung surgery who presented in shock with an intraparenchymal chest tube placement requiring emergency thoracotomy. A thoracoplasty was utilized to gain exposure in the chest due to adherence of the lung to the chest wall. This case report discusses iatrogenic lung injury with possible treatment options in patient populations with previous lung surgery.
Iatrogenic lung injury, intraparenchymal chest tube placement, lung repair, thoracoplasty, thoracotomy
INTRODUCTION
Chest tube thoracostomy is a commonly performed procedure in both general surgery and emergency medicine, though it is not without its own complications. Errors leading to mispositioned tubes, infection, and injury to the patient are not benign and must be considered along with their respective management strategies. The ideal surgical management of an intraparenchymal tube placement is not well described in the literature.
CASE REPORT
A 74-year-old female with known chronic obstructive pulmonary disease and a history of a right lower lobectomy for lung cancer presented to an emergency department for worsening dyspnea that had been present for several days. On arrival, she was noted to have a 90% oxygen saturation on room air and was conversationally dyspneic. A chest X-ray was performed that indicated a right hydropneumothorax. She agreed to undergo chest tube thoracostomy for her symptoms. A post-procedure X-ray indicated likely intraparenchymal placement of the tube into the lung. She quickly began exhibiting signs of clinical decompensation including worsening respiratory status requiring high- flow oxygen through a non-rebreather mask, hemoptysis, and hypotension. She was transferred to our facility for cardiothoracic surgical evaluation.
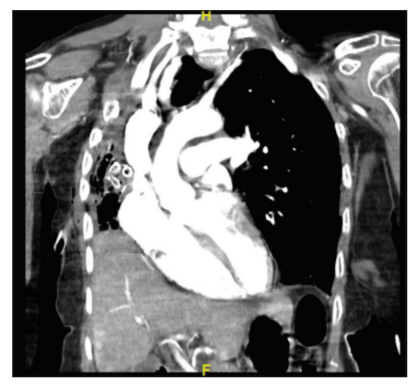
On arrival, she was noted to have altered mental status, respiratory failure requiring BiPAP, persistent hemoptysis, and was hypotensive. Laboratories were drawn on arrival and compared with her outside hospital laboratories, which revealed that her hemoglobin had decreased by 2 g/dL over the course of 2 h. A chest computed tomography (CT) was performed and confirmed intraparenchymal chest tube placement into the right lung, nearly abutting the heart [Figure 1].
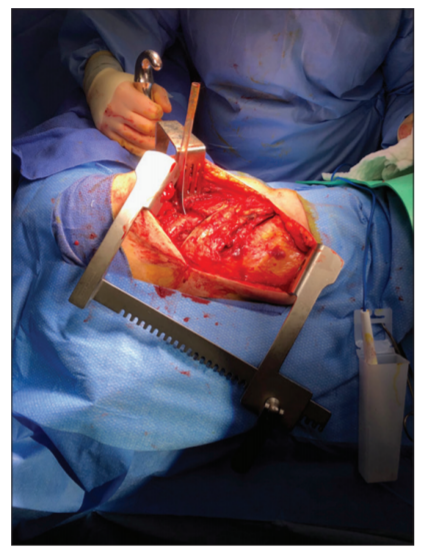
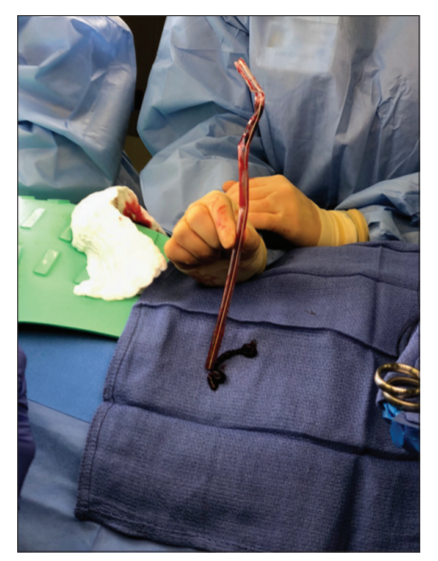
The patient was exhibiting signs of shock with a known iatrogenic injury. The differential diagnosis included active bleeding, bronchopleural fistula, or unresolved pneumothorax. Due to her worsening clinical state, she was emergently taken to the operating room for a right thoracotomy. In the operating room, a posterolateral thoracotomy incision was made and the ribs were exposed. The chest tube was visible entering an intercostal space directly into the chest cavity. Due to the patient's previous lung surgery, the patient's lung was completely fixed to the chest wall and unable to be mobilized. To repair the pulmonary laceration, a thoracoplasty was performed with two rib segments removed to expose the lung and the chest drain was extracted intact [Figures 2 and 3]. A purse-string suture was placed around the chest tube entrance site and was tied down after its removal. Additional mattress sutures were placed overlying this repair site. A pleural air leak sealant was applied over the site of injury for reinforcement. A small pleural drain was left overlying the injury to evaluate for a persistent bronchopleural fistula.
The patient recovered well and was extubated the morning after surgery. Her pleural drain did not indicate a persistent leak and was removed on post-operative day 2. Her laboratories remained stable and she was eventually discharged from the hospital after a benign course of recovery.
DISCUSSION
While chest tubes in the lung parenchyma are documented in the literature, their sequela and management are much less discussed. One study examined the incidence of chest tubes placed into the lung parenchyma which was diagnosed in 9% of patients at their institution [1]. Interestingly, most of these were not diagnosed or suspected clinically or chest radiograph but by CT scans. A case series describes three examples of postmortem diagnosed pulmonary perforations secondary to the chest tube placement that was clinically unknown before death [2].
This complication is more commonly reported in neonatology literature due to presumed increased frequency of the complication related to the higher degree of difficulty often found in tube thoracostomies in premature infants. Wilson describes "stiff lung" syndrome in neonates associated with intraparenchymal chest tube placement diagnosed on autopsy [3]. The presumed increased the incidence of this type of complication is described secondary to the adherence of the lung to the chest wall, leading to perforation, compared to normal lung tissue whose pliability allows displacement with the insertion of the tube. That author recommends suspicion of the diagnosis when a pneumothorax or hemothorax fails to resolve after placement of a chest tube in an infant with "stiff lung syndrome". Certainly, this same index of suspicion could be applied to the adult population with a history of lung pathology such as thoracotomy, pleurodesis, or malignancy. Such a history of lung pathology undoubtedly complicates the operative planning of thoracic exploration and repairs due to scar tissue or friability of the tissues.
The management of lung perforation in the literature is scarcer as often these are either diagnosed postmortem or asymptomatic and do not require aggressive treatment. For example, there is a case report describing a successful repair of an iatrogenic lung perforation with thoracotomy and primary suture repair of the lung laceration on a neonate [4]. However, majority of other case reports describing this condition typically allude to need for thoracotomy for definitive repair, but the description of the surgical technique is limited.
Historically, thoracoplasty - a procedure to remove ribs to decrease the volume of the thoracic cavity was a treatment for tuberculosis which often led to empyema in the era before treatment existed. As tuberculosis became a medical rather than surgical disease, this procedure's commonality fell out of favor. Originally, the Schede thoracoplasty was described in Vienna in 1890 which removed the intercostal muscles, neurovascular bundle, and parietal pleura in addition to ribs over the infected part of the lung [5]. The modern thoracoplasty is limited to resection of the overlying ribs alone [5].
CONCLUSIONS
With a suspected relatively high rate of incidence in chest tube placements, the management of a pulmonary injury secondary to tube thoracostomy could easily be an encountered complication for thoracic or trauma surgeons. Applying basic surgical principles of patient resuscitation and early recognition of clinical deterioration are important components of the treatment plan. In patient populations with intrathoracic scar tissue and inability to manipulate the lung, a thoracoplasty and primary lung repair are practical options for definitive management.
REFERENCES
- Remerand F, Luce V, Badachi Y, Lu Q, Bouhemad B, Rouby JJ. Incidence of chest tube malposition in the critically ill: A prospective computed tomography study. Anesthesiology 2007;106:1112-9.
- Fraser RS. Lung perforation complicating tube thoracostomy: Pathologic description of three cases. Hum Pathol 1988;19:518-23.
- Wilson AJ, Krous HF. Lung perforation during chest tube placement in the stiff lung syndrome. J Pediatr Surg 1974;9:213-6.
- Gangitano ES, Pomerance JJ, Gans SL. Successful surgical repair of iatrogenic lung perforation in a neonate. J Pediatr Surg 1981;16:70-1.
- Pomerantz BJ, Cleveland JC, Pomerantz M. The schede and modern thoracoplasty. Oper Tech Thorac Cardiovasc Surg 2000;5:128-34.