Worsening Tension Pneumocephalus from Late Post-traumatic Ventriculo-bronchial Fistula Due to Hyperbaric Oxygen Therapy
Zaid Tayyem1, Brenda Pulgarin1, Elena Schmidt2, Julius Gene Latorre2
2.Department of Neurology, Neurocritical Care Service, Upstate Medical University, Syracuse, NY 13210, USA
Citation : Tayyem Z, Pulgarin B, Schmidt E, Latorre JG. Worsening Tension Pneumocephalus from Late Post-traumatic Ventriculo-bronchial Fistula Due to Hyperbaric Oxygen Therapy. Asclepius Med Case Rep 2018;1(2):1-3.
The objective of the study was to report a case of tension pneumocephalus presenting as status epilepticus and outcome of treatment following emergency hyperbaric oxygen therapy. The data were collected from electronic medical record. The study was a case report. The data were extracted from medical record review and literature search. A 41-year-old male presented with status epilepticus and was found to have pneumocephalus within the cerebral venous sinuses. Before presentation he was complaining of intermittent hemoptysis attributed to a lung injury from a remote trauma due to a stab wound in the chest. At the time of his chest injury, he underwent multiple operations. His recovery was complicated by formation of left ventricular aneurysm and ventriculopleural fistula which was successfully repaired 5 years before presentation. Before determining the exact etiology of pneumocephalus, the patient was emergently treated with hyperbaric oxygen therapy (HBOT) to help with the management of intractable status epilepticus. During the HBOT therapy, the patient developed hemodynamic instability and the therapy was aborted. Repeat computed tomography (CT) scan showed worsening pneumocephalus with massive brain swelling and herniation. An echocardiogram showed bubbles crossing the left ventricle to the aorta. A CT thorax showed evidence of communication between the left ventricle and lung parenchyma at the site of the Gore-Tex confirming a ventriculo-bronchial fistula. Despite aggressive measures to control intracranial hypertension, the patient deteriorated and was declared brain dead. In cases of pneumocephalus where the exact cause is not well documented, an extensive investigation is recommended to ascertain the etiology before the institution of hyperbaric oxygen therapy.
Cerebral air embolism, hyperbaric oxygen therapy, neurocritical care, pneumocephalus, status epilepticus, ventriculo-bronchial fistula
INTRODUCTION
Massive cerebral air embolism seen on computed tomography (CT) scan is rare with only a small number of cases reported[1]. We report a case of massive cerebral air embolism causing tension pneumocephalus that worsened after hyperbaric oxygen therapy. The etiology of air embolism was later determined to be due to the development of a ventriculo-bronchial fistula after an injury related to a remote stab wound to the chest.
CASE REPORT
A 41-year-old male presented to a tertiary care center with intractable convulsive status epilepticus.
The patient was stabbed in the chest injuring the left ventricle some 11 years ago. He underwent multiple operations to repair the injury and subsequently developed a left ventricular aneurysm with ventriculopleural fistula. This was resected and repaired employing the double patch technique using Gore-Tex. The Gore-Tex eventually eroded the lung sub-parenchyma causing a fistula and massive hemoptysis. This was successfully repaired surgically. Following repair, the patient was asymptomatic for several years. However, a few months before presentation he suffered a low degree of hemoptysis. Bronchoscopies showed blood in the lingula, where the lung parenchyma had been damaged by the fistula. Left ventriculogram was done showing no evidence of recurrent fistula or aneurysm. The hemoptysis was attributed to bronchiectatic lung aggravated by continued smoking. His treatment included antibiotics, bronchial artery embolization, and admonitions to stop smoking. Despite these measures, the patient's hemoptysis persisted.
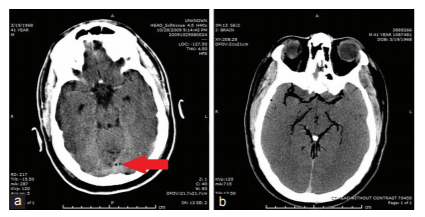
A few days prior, the patient presented to an outside hospital after a new onset generalized seizure. Despite treatment with multiple anti-epileptic medications, the seizures continued and progressed to status epilepticus prompting the patient to be intubated and started on a midazolam drip. He was then referred and transferred to our institution for further management. A CT scan of the head from outside hospital was reported as no acute pathology, but on review, cerebral air embolism was found along the superior sagittal sinus [Figure 1a]. A maxillofacial CT showed no evidence of a facial fracture or sinus erosion and the pneumocephalus was emergently treated with hyperbaric oxygen therapy.
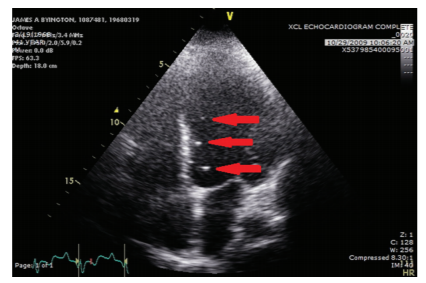
A short while into the hyperbaric oxygen treatment the patient developed hypotension and tachycardia. The treatment was aborted, and a repeat CT scan showed significantly increased pneumocephalus and diffuse brain swelling [Figure 1b]. He was immediately transported to the Neuro-ICU, and osmotic therapy started. An echocardiogram, performed because of elevated troponins, showed an ejection fraction of 10-15% and bubbles crossing the left ventricle to the aorta with no clear origin [Figure 2]. A CT Thorax showed evidence of communication between the left ventricle and lung parenchyma at the site of the Gore-Tex confirming a ventriculo-bronchial fistula. Despite supportive measures, the patient continued to decompensate eventually leading to brain death.
DISCUSSION
Pneumocephalus in the absence of a recent intracranial or intrathecal procedure is a significant radiographic finding and should prompt investigation to identify the cause[2]. Air embolisms are usually iatrogenic or a complication of trauma[3]. The patient had a remote history of trauma but had not suffered any recent trauma or surgical procedure before presenting to the hospital. A CT scan is useful for determining the location and volume of cerebral air embolism. However, CT demonstration of air in almost all the major cerebral arteries is extremely rare[4]. Prior case reports have documented that false ventricular aneurysms may be asymptomatic and can lead to delayed complications, including fistulation into the bronchial tree leading to massive hemoptysis and air embolism[5]. Penetrating chest injuries may produce a bronchopulmonary venous fistula and arterial air embolism with the mortality rate of 66% in one series of nine patients[6]. The only current treatment for tension pneumocephalus is hyperbaric oxygen therapy[7]. There have been no clinical trials into the use of hyperbaric oxygen in air embolism, but one case series of arterial gas embolism showed significant improvement of symptoms with hyperbaric oxygen treatment[8].
This case highlights the detrimental consequence of positive pressure ventilation and hyperbaric oxygen therapy in exacerbating the air embolism in patients with ventriculo-bronchial fistulas. The increased oxygen gradient at an elevated atmospheric pressure, in this case, resulted in large amounts of air entering the systemic circulation and eventually the patient's intracranial vessels resulting in an increase in ICP. Furthermore, as he already had an area of injury in the lung parenchyma, positive pressure ventilation may have produced pulmonary barotraumas leading to a greater predisposition for cerebral air embolism[9]. As the amount of air in the intracerebral vessels increased, a concurrent increase in ICP occurred leading to trans tentorial herniation.
CONCLUSION
In cases of pneumocephalus where the exact cause is not well documented, an extensive investigation is recommended to ascertain the etiology before the institution of hyperbaric oxygen therapy.
References
- 1. Hwang SL, Lieu AS, Lin CL, Liu GC, Howng SL, Kuo TH, et al. Massive cerebral air embolism after cardiopulmonary resuscitation. J Clin Neurosci 2005;12:468-9.
- Cruz-Flores S, Diamond AL, Leira EC. Cerebral air embolism secondary to intra-aortic balloon pump rupture. Neurocrit Care 2005;2:49-50.
- Syed ON, Weintraub D, DeLaPaz R, Connolly ES. Venous air emboli from intravenous catheterization: A report of iatrogenic intravascular pneumocephalus. J Clin Neurosci 2009;16:1361-2.
- Hwang TL, Fremaux R, Sears ES, MacFadyen B, DSc BH, Mader JT, et al. Confirmation of cerebral air embolism with computerized tomography. Ann Neurol 1983;13:214-5.
- Jensen ME, Lipper MH. CT in iatrogenic cerebral air embolism. AJNR Am J Neuroradiol 1986;7:823-7.
- Yamaki T, Ando S, Ohta K, Kubota T, Kawasaki K, Hirama M, et al. CT demonstration of massive cerebral air embolism from pulmonary barotrauma due to cardiopulmonary resuscitation. J Comput Assist Tomogr 1989;13:313-5.
- Banagale RC. Massive intracranial air embolism: A complication of mechanical ventilation. Am J Dis Child 1980;134:799-800.
- Estrera AS, Pass LJ, Platt MR. Systemic arterial air embolism in penetrating lung injury. Ann Thorac Surg 1990;50:257-61.
- Benson J, Adkinson C, Collier R. Hyperbaric oxygen therapy of iatrogenic cerebral arterial gas embolism. Undersea Hyperb Med 2003;30:117-26.