Cervical Vagal Schwannoma: A Case Report and Literature Review
Bouzbouz Anas, Laababsi Rabii, Allouane Mohamed Amine, Abdul Hakeem Bushra, Rouadi Sami, Abada Reda Lah, Roubal Mohamed, Mohamed Mahtar
Citation : Anas B, Rabii L, Amine AM, Bushra AH, Sami R, Lah AR, Mohamed R, Mahtar M. Cervical Vagal Schwannoma: A Case Report and Literature Review. Asclepius Med Case Rep 2018;1(2):1-3.
Schwannoma is a rare benign mesenchymal tumor, developed exclusively from Schwann's sheath cells. In 25% of cases, it occurred in the neck. We report through this case the suggestive radiological signs, the histological features, as well as the therapeutic approach. A 60-year-old female admitted in our department for an isolated right-sided lateral cervical swilling that had been evolving for 10 months. Computed tomography showed a large mass of the right carotid bifurcation, pushing back the elements of the jugular carotid complex. The surgery had consisted in a complete excision of the mass. Histopathological and immunohistochemical analysis had concluded to a schwannoma. The post-operative follow-up was simple without any complications. The schwannoma of the vagus nerve is a rare tumor described in the literature. It is often discovered as an isolated lateral cervical mass, gradually increasing in volume. Imaging is considered the most useful diagnostic modality for revealing schwannoma that will be confirmed afterward, by the histological study of the operative specimen. Regardless of the large cases of post-operative complications such as dysphonia, the main treatment is surgical.
Cervical computed tomography, cervicotomy, schwannoma, vagus nerve
INTRODUCTION
Schwannoma is a benign mesenchymal tumor developed exclusively from Schwann sheath cells that surrounded the nerve fibers of the peripheral nervous system. The neck region is the most common site for schwannomas (25%) and often developed from the vagus nerve [1].
The diagnosis of schwannoma is essentially based on imaging (computed tomography [CT] and magnetic resonance imaging [MRI]). The treatment is surgical despite the considerable risk of definitive functional problems.
We report a recent case of cervical schwannoma of the vagus nerve, and we propose a question update through a review of the literature.
CASE REPORT
A 60-year-old female without any particular pathological history, presented with a 10-month history of a right lateral cervical tumefaction increasing gradually in size.
The physical examination had found an upper lateral cervical mass, non-tender, mobile, and without any inflammatory signs. It was not associated with any other symptoms such as dysphonia, dysphagia, pain, or weight loss.
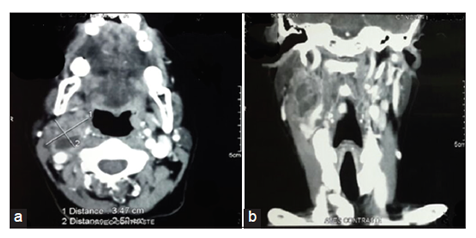
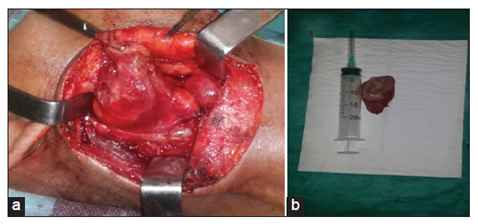
An enhanced cervical CT revealed a well-circumscribed, homogenous, heterodense, and largely cystic mass of the right carotid bifurcation, filling the ipsilateral parapharyngeal space, measuring 50 mm X 30 mm X 21 mm, with medial displacement of the external carotid artery and the internal jugular vein and posterior-lateral displacement of the internal carotid artery. It also pushes back the parotid gland and the sternocleidomastoid muscle. The CT shows the presence of a small hypodense lesion in the left tonsillar space measuring 20 mm X 12 mm, with moderate enhancement post-contrast [Figure 1]. Otherwise, the patient could not afford an MRI the mass was excised through a transverse right cervical skin incision [Figure 2].
Anatomopathological examination of the operative specimen revealed a fusocellular tumor proliferation made of spindleshaped elements with moderately eosinophilic cytoplasm and discretely hyperchromic nuclei or sites of moderate uncommon cytonuclear aspect, without mitosis. These cells combine into entangled bundles dissociated by clusters of foamy and siderophages histiocytes, giving rise to a remodeled schwannoma. It was confirmed by immunohistochemical study showing an intense and diffuse positivity to the S100 proteins (PS100). The post-operative follow-up was simple without any abnormalities.
DISCUSSION
Nerve's cervical tumors have been described since 1742 after the discovery of the carotid glomus by Von Haller, the first description of neck's schwannoma was made by Ritter in 1899 [2].
This is a benign nerve sheath tumor that occurs along the length of the nerves. It is a solitary, slowly growing tumor generally observed in patients between 20 and 70 years old. The frequency is the same in both sexes [3]. These tumors occur in the region of the head and neck in 25% of cases, the intracranial location (vestibular nerve) is the most common [1,4]. Schwannoma usually presents as a laterally increasing cervical tumefaction, isolated, and asymptomatic, but it may cause by its size non-specific symptoms such as dysphagia, dysphonia, and odynophagia.
In the literature, the positive diagnosis of cervical Schwannoma is based primarily on imaging, including computed tomography (CT) and magnetic resonance imaging (MRI). These examinations make it possible to locate the tumor to show its characteristics, its relationships with the neurovascular elements and to make the differential diagnosis with a non-vascularized lymphadenopathy, a carotid glomus, a paraganglioma of the vagus nerve or a congenital cyst [2,3].
The cytological study after a needle aspiration is often with non-contributory results [5].
Macroscopically, the tumor takes a spherical form, the net capsule is formed from the epinerve. Microscopically, we observe a fibrous capsule within the Antoni A and B areas. Antoni A regions are composed of more densely arranged cells with specific areas of palisading nuclei arranged in rows; Antoni B regions are tended to be more hypocellular, with a loose and disorderly arrangement. The proliferation index is weak. In immunohistochemical study, the PS 100 is positive in all schwannomas and neurofibromas [6]. In general, schwannomas prognosis is excellent, local recurrence is rare, but it can occur resulting from an incomplete surgical excision. The degeneration of a benign schwannoma is impossible, since, it is right from the beginning benign or malignant [2].
CONCLUSION
The schwannoma of the vagus nerve is a rare tumor described in the literature. It is often discovered as a solitary lateral cervical mass, slow-growing in size. Imaging is considered the most requisite diagnostic modality for revealing schwannoma that will be confirmed thereafter by the histological study. The treatment of choice is surgical, despite several postoperative problems such as dysphonia.
References
- Nao EE, Dassonville O, Bozec A, Sudaka A, Marcy PY, Vincent N, et al. Cervical sympathetic chain schwannoma. Eur Ann Otorhinolaryngol Head Neck Dis 2012;129:51-3.
- Kim SH, Kim NH, Kim KR, Lee JH, Choi HS. Schwannoma in head and neck: Preoperative imaging study and intracapsular enucleation for functional nerve preservation. Yonsei Med J 2010;51:938-42.
- Furukawa M, Furukawa MK, Katoh K, Tsukuda M. Differentiation between schwannoma of the vagus nerve and schwannoma of the cervical sympathetic chain by imaging diagnosis. Laryngoscope 1996;106:1548-52.
- Chiofalo MG, Longo F, Marone U, Franco R, Petrillo A, Pezzullo L. Cervical vagal schwannoma. A case report. Acta Otorhinolaryngol Ital 2009;29:33-5.
- Colreavy MP, Lacy PD, Hughes J, Bouchier-Hayes D, Brennan P, O'Dwyer AJ, et al. Head and neck schwannomas: A 10-year review. J Laryngol Otol 2000;114:119-24.
- Enzinger FM, Weiss SW, editors. Benign Tumors of Peripheral Nerves. Soft Tissue Tumors. 3rd ed. Saint-Louis: Mosby; 1995. p. 821-72.