A Rare Case Report: Atypical Leiomyoma Invasive to Fallopian Tube
Emre Kole, Merve Kole, Fureyya Zilal Hocagil
Citation : Kole E, Kole M, Hocagil FZ. A Rare Case Report: Atypical Leiomyoma Invasive to Fallopian Tube. Asclepius Med Case Rep 2018;1(2):1-3.
Uterine leiomyoma is the most common tumor of the female genital tract. Apart from typical cases of leiomyomas, symplastic/ bizarre or atypical leiomyomas (ALMs), also known as pleomorphic leiomyomas, are also encountered. In general, they show a benign behavior. In some cases, intrauterine or extrauterine recurrences can be seen. The most important is immunohistochemically making a differential diagnosis of leiomyosarcoma. Histopathological evaluation of a 42-year-old female patient who underwent laparoscopic hysterectomy and bilateral salpingo-oophorectomy due to 21-cm leiomyomas in the uterus, atypical, multiple nuclei, hyperchromatic, pleomorphic atypical bizarre cells was observed at multifocal foci. Mitosis was rarely seen (2/10 high power fields). P53 was negative. ALMs are one of the rare tumor variants whose smooth muscle histologically resembles leiomyosarcoma. To exclude leiomyosarcoma in these tumors, a multidisciplinary approach is required among the clinics as well as histopathological criteria.
Immunohistochemistry, leiomyoma, leiomyosarcoma, uterus
INTRODUCTION
Atypical leiomyomas (ALMs) are characterized by moderately to severely pleomorphic atypical tumor cells with low mitotic counts. Despite the worrisome histologic features, most tumors show benign behavior [1].
Pathologic interpretation should be made with clinical and radiological evaluation because hypersales in histopathological examination, necrosis, nuclear atypia, mitosis, and intravenous growth can be seen in variant of benign leiomyomas [2]. ALMs have not been associated with coagulative cell necrosis or a mitotic index of 10 high-power fields (HPFS) and a cytotoxic excess of 10 mitoses per atypia.
These atypical cells frequently have large cytoplasmic pseudonuclear inclusions; hyperchromatic nuclei expanded with a pronounced chromatin condensation. Atypical cells are mostly located multifocal and diffuse. They are usually clinically benign, but sometimes, they can recur because, in some cases, tumor of low malignant potential must be suspected [3].
CASE REPORT
A 42-year-old, gravida 4, parity 3 patient applied to the clinic with complaints of irregular menstruations. Ultrasonographic examination of the patient revealed a right adnexal mass measuring about 20 cm X 16 cm. The vital signs of the patient were stable. There was no known chronic disease in patient's medical history. She did not have any past surgical history. The patient was without a history of cigarette smoking and drug use. The physical examination of the patient revealed that the wart and other system examinations of the patient were normal. Abdominal examination was soft, unresponsive, and lacking sensitivity, and uterine and mass sizes were 30 weeks' gestation. Vaginal speculum examination showed normal appearance of the cervix and vagina. Smear was obtained from the patient, and diagnostical curettage was performed. Magnetic resonance imaging (MRI) of the abdomen was planned. In the laboratory, complete blood count showed that hemoglobin was 12.5 g/dl, platelet was 240000 mm3, and complete urinalysis test was normal. CA125 levels were 37 U/mL. The smear result of the patient was reported as negative for intraepithelial lesion or malignancy. The diagnostic endometrial curettage was reported to be in secretory phase endometrium. Since MRI result was in compliance with the subserous myoma, surgical operation was decided. In assessing the patient during the operation, it was observed that, due to tumoral mass, the uterus was deviated to the left, large conglomerate mass enclosing the right fallopian tube and ovary. After the ureteral dissection to the right iliac fossa obliterating fatty tissue, total abdominal hysterectomy with bilateral salphingo oophorectomy was performed.
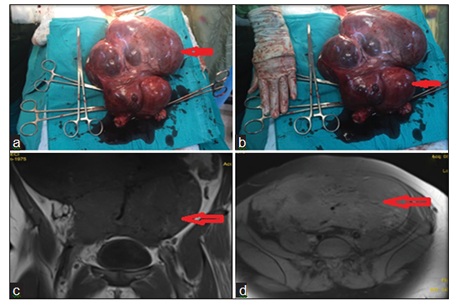
Bilateral pelvic lymph node dissection (PLND) and omentectomy were performed due to the presence of malignancy in operation. Due to the presence of suspected malignancy in operation, bilateral PLND and omentectomy were performed. Since the patient's post-operative follow-up was free from any distress, the patient was discharged. In the pathological result of approximately 2500 g weight mass, tumor was observed to invade the right tubule and bypassing the serosa, transformed to peritoneal fatty plan [Figure 1]. At the same time, during the microscopic examination, it was observed that it consists of atypical cells expressing pleomorphism, vascular structures, and hypercellular. Significant mitosis and necrosis were not observed in the sections. Immunohistochemical evaluation, smooth muscle antibody: Positive, Desmin: Positive, Kaldesmon: Positive, CD10: Positive, Ki-67: positive in rare tumor cells. Finally, it was reported as an atypical leiomyoma with no potential for malignancy. Omentum and the involvement of lymph nodes were not observed. No recurrence was observed in the follow-up period of the patient.
DISCUSSION
Uterine leiomyomata and benign smooth muscle tumors of the uterus are the most common tumors in women genital tract. While most of the leiomyomas are seen as typical leiomyomas, sometimes it is also possible to encounter with atypical variants of leiomyomas. Among these variants, although ALMs or also called symplastic/bizarre or pleomorphic leiomyoma generally shows benign behavior, intrauterine or extrauterine recurrences are possible. Some authors even regard leiomyosarcoma as a precursor lesion due to histologically similar structures to leiomyosarcomas. ALMs are characterized by focal, multifocal, or diffuse moderate-to-severe pleomorphic, atypical bizarre cells. While tumor cells show low mitotic counts (< 7/10 HPF), they do not present coagulative tumor cell necrosis. In ALMs, the average tumor size was 6.8 cm and the average patient age was 42.5 years. In these cases, the initial diagnostic procedure was hysterectomy or myomectomy. Atypical leiomyoma has a low rate of extrauterine and intra-abdominal recurrence by 2%. For this reason, patients must be monitored for recurrent disease [4]. In our case, tumor size was 21 cm, and the patient was 42 years old. After the post-operative hysterectomy, histopathological diagnosis was made. In the differential diagnosis of leiomyosarcoma, immunohistochemical analysis is important. P16 and p21 positivity supports leiomyosarcoma. When we have evaluated p16 and p21 in uterine smooth muscle tumors to determine whether p16 and p21 have a potential value in the differential diagnosis of problematic cases, we found that p16 and p21 were negative [5] Bcl-2 protein is an apoptosis-inhibiting gene product which prevents the course of apoptotic cell death in various cells. Bcl-2, in the differential diagnosis, more frequent and stronger expression is observed in leiomyosarcoma compared to the leiomyomas. Bcl-2-positive leiomyosarcoma with better clinical results shows that this protein is a good prognostic factor [6] In our case, Bcl-2 expression was positive. In these cases, immunohistochemically another marker p53 negativity can provide guidance in terms of sarcomatous change and aggressiveness [7]. Since, in our case, we also have p53 negativity and assessed together with other clinical and radiological findings, it was evaluated to be atypical leiomyoma.
As a result, in the differential diagnosis of ALMs and leiomyosarcomas, multidisciplinary pathologist radiologist and gynecologist must decide together and immunohistochemical evaluation is particularly important.
References
- Sung CO, Ahn G, Song SY, Choi YL, Bae DS. Atypical leiomyomas of the uterus with long-term follow-up after myomectomy with immunohistochemical analysis for p16INK4A, p53, ki-67, estrogen receptors, and progesterone receptors. Int J Gynecol Pathol 2009;28:529-34.
- Prayson RA, Hart WR. Pathologic considerations of uterine smooth muscle tumors. Obstet Gynecol Clin North Am 1995;22:637-57.
- Ip PP, Cheung AN, Clement PB. Uterine smooth muscle tumors of uncertain malignant potential (STUMP): A clinicopathologic analysis of 16 cases. Am J Surg Pathol 2009;33:992-1005.
- Ly A, Mills AM, McKenney JK, Balzer BL, Kempson RL, Hendrickson MR, et al. Atypical leiomyomas of the uterus: A clinicopathologic study of 51 cases. Am J Surg Pathol 2013;37:643-9.
- Unver NU, Acikalin MF, Oner U, Ciftci E, Ozalp SS, Colak E, et al. Differential expression of P16 and P21 in benign and malignant uterine smooth muscle tumors. Arch Gynecol Obstet 2011;284:483-90.
- Bodner K, Bodner-Adler B, Kimberger O, Czerwenka K, Mayerhofer K. Bcl-2 receptor expression in patients with uterine smooth muscle tumors: An immunohistochemical analysis comparing leiomyoma, uterine smooth muscle tumor of uncertain malignant potential, and leiomyosarcoma. J Soc Gynecol Investig 2004;11:187-91.
- Hewedi IH, Radwan NA, Shash LS. Diagnostic value of progesterone receptor and p53 expression in uterine smooth muscle tumors. Diagn Pathol 2012;7:1.