A Rare Case Report: Subcapsular Hepatic Hematoma as a Complication of Preeclampsia
Merve Kole, Emre Kole, Sumeyye Kanbay
Citation : Kole M, Kole E, Kanbay S. A Rare Case Report: Subcapsular Hepatic Hematoma as a Complication of Preeclampsia. Asclepius Med Case Rep 2018;1(2):1-3.
Due to preeclampsia and hemolysis, elevated liverenzymes, and low platelet count (HELLP) in spontaneous pregnancy, spontaneous subcapsular hepatic hematoma can present as a life-threatening rare complication. In this case, we present a case of rare preeclampsia, which progressed to subcapsular hepatic hematoma. A 41-year-old female patient applied to the emergency ward 5 days after cesarean with high blood pressure and right upper quadrant (RUQ) pain. Abdominal examination showed abdominal tenderness in the RUQ; TA: 200/100, pulse: 88, fever: 36.8, SS: 20, and SO2: 99 were measured. Gynecologic ultrasound was normal. Since computed tomography of the abdomen showed hyperdense areas containing subcapsular hematoma of the right liver upper lobe (13 cm X 11 cm X 18 cm), "subcapsular hematoma developing after preeclampsia" was diagnosed. Abnormal liver function tests in pregnancy range from mild elevation of liver enzymes to severe deterioration in liver function. Subcapsular liver hematoma developing secondary to preeclampsia and HELLP syndrome is a rarely encountered case which must be kept in mind. It happens with clinically non-specific findings such as nausea, vomiting, and abdominal distension associated with RUQ pain spreading to the epigastric or shoulder. Early diagnosis reduces morbidity and mortality.
Hemolysis; elevated liverenzymes; and low platelet count, preeclampsia, subcapsular hepatic hematoma
INTRODUCTION
Subcapsular hepatic hematoma is the accumulation of blood between the capsule of Glisson and the liver parenchyma. Clinically non-specific findings such as nausea, vomiting [1-3]. Preeclampsia is a multisystemic disease. Cardiovascular system, central nervous system and genito-urinary system are affected in patients with preeclampsia. But all systems can be affected at a certain level [4].
CASE REPORT
A 41-year-old gravida 2, parity 2, 5 days after the cesarean applied to the emergency service with the complaint of hypertension and pain in the right upper quadrant (RUQ). Her medical history showed 21 pack year history of smoking. When she applied, her vital signs were measured as TA: 200/100, pulse: 88, fever: 36.8, SS: 20, and SO2: 99. In the examinations of the patient, Hg: 10.2, platelet: 3,82,000; white blood cells: 15,000, urea: 54, Kr: 0.7, aspartate aminotransferase (AST): 931, alanine aminotransferase (ALT): 694, lactate dehydrogenase: 945 TIT à+3, and the protein were present. In the examination of the abdomen, sensitivity was observed in the RUQ.
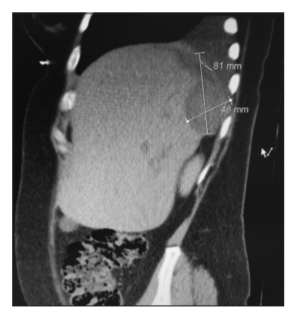
Abdominal computed tomography (CT) showed hyperdense areas containing subcapsular hematoma of the right liver upper lobe (13 cm X 11 cm X 18 cm size), in the right lobe of liver compatible with atelectasis of the right lower lobe [Figure 1].

The patient was admitted to Kocaeli University Obstetrics and Gynecology Department with the pre-diagnosis of subcapsular hepatic hematoma as a complication of preeclampsia.
In the gynecologic ultrasound, "uterine involution was natural; endometrium: 4 mm; pouch of Douglas: Natural; and fundus examination: Normal" were evaluated; general surgery; gastroenterology and pulmonary consultations were requested; since the C-reactive protein (CRP) values were high, antibiotic treatment started after consultation with infectious diseases physician.
The patient was assessed by general surgery specialist, and unless there is no decrease in HG, taking a conservative approach decision was given. Pulmonary specialist suggested that lobar atelectasis of the right lung was due to the pressure, and he recommended daily follow-up of the liquid taken in and out that it must remain neutral and oxygen mask and radiological follow-up.
Gastroenterology was consulted, due to suspicion of ischemic hepatitis, ELISA test was asked. During hospital follow-up under oxygen mask when SO2: 87 was measured (decreased), intensive care unit consultation was requested and the patient was transferred to Intensive Care Unit for intensive treatment and observance (15.07.16).
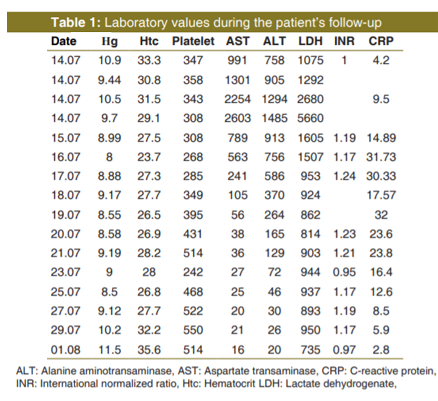
Patient stayed in the ICU for 5 days; daily Hg; International Normalized Ratio (INR); KCFT follow-up [Table 1], and hematomas were subjected to follow-up ultrasound scan every 3 days. When the general condition of the patient stabilized, the patient was transferred to the service and medical treatment was continued; Antibiotherapy and posteroanterior chest X-ray were followed up with abdominal ultrasonography (USG). The hemoglobin level of the patient did not decrease; liver function test showed regression. After cardiology consultation, antihypertensive therapy was administered. Abdominal USG showed that hematoma area decreased gradually. Bronchoscopy was performed on 02.08.16, recommended by the pulmonology; external compression in the right lower lobe, all lobes, and segment mouths were reported as open.
On the 20th day of hospitalization, the general condition of the patient was good; vital signs were stabilized. With the control of cardiology, gynecology, and pulmonary polyclinics, she was discharged from the hospital.
When the patient came for the control 2 weeks later, Hg: 12.5, hematocrit: 41.5, AST: 12, ALT: 11, INR: 1.16, and CRP: 2.96 were measured. Abdominal US showed; the right lower lobe of the liver was assessed to have a heterogeneous area (approximately 11 cm * 7 cm in size) and 3 cm of fluid in its vicinity, which could not be clearly defined. 1 month later control in the abdominal CT of the patient, old hematoma area (3.5 cm * 8 cm size) was observed in the liver right upper lobe [Figure 2].
DISCUSSION
Subcapsular hepatic hematoma is the accumulation of blood between the capsule of Glisson and the liver parenchyma. It was first described by Abercombie in 1844 [1]. The etiopathogenesis still remains unclear [2]. An interesting hypothesis is based on the formation of fibrin thrombus within the hepatic arteries and sinusoid capillaries which in turn leads to periportal necrosis, intrahepatic hemorrhage, and finally subcapsular hematoma [3]. When evaluating the subcapsular liver hematoma (SLH) as histopathological and intraparenchymal hemorrhage, common microaneurysms with periportal or focal parenchymal necrosis is observed [4].
Clinically non-specific findings such as nausea, vomiting, and abdominal pain accompany the RUQ pain spreading to the epigastric or shoulder. Abdominal ultrasound is used as the first non-invasive option [3].
CT and magnetic resonance imaging can be used as diagnostic tools. Hemodynamically stable patients should be followed up conservatively by means of intensive medical support with infused fluid and replacement of blood products.
In most cases, the right liver lobe is affected [4]. Hemolysis, elevated liverenzymes, and low platelet count (HELLP) syndrome occurs in about 0.5-0.9% of all pregnancies [5]. It occurs due to the delayed diagnosis of preeclampsia.
In most cases, HELLP syndrome occurs before delivery. As a complication of HELLP syndrome, disseminated intravascular coagulation is frequently encountered in 15-20% of the cases.
In some cases, to control the bleeding in the liver, percutaneous transcatheter hepatic artery embolization is performed. When the patient is unstable, immediate surgical intervention is mandatory. To the bleeding area, collagen-based agents in combination with a procoagulant substance may be applied or drainage of perihepatic space can be done.
Sibai reported a 13-year retrospective review of three patients with SLH. Two of them were managed conservatively and discharged from hospital. The other patient underwent hepatic resection and had mortality due to multiple organ failure [5].
SLH secondary to preeclampsia and HELLP syndrome is a rare clinical entity which must kept in mind [6-8]. Follow-up for these patients is important. If the patient's vital signs are stable, conservative management is the preferred treatment method. Early detection decreases morbidity and mortality.
References
- Abercombie J. Cases of hemorrhage of the liver'. Lond Med Gaz 1844;34:792.
- Manas KJ, Welsh JD, Rankin RA, Miller DD. Hepatic hemorrhage without rupture in preeclampsia. N Engl J Med 1985;312:424-6.
- Cernea D, Dragoesceu A, Novac M. HELLP syndrome complicated with postpartum subcapsular ruptured liver hematoma and putscher like retinopathy. Case Reports Obstetr Gynecol1012;2012:4.
- Dessole S, Capobianco G, Virdis P, Rubattiu G, Cosmi E, Porcu A. Hepatic rupture after ceserian section in apatient with HELLP Syndrome; A case report and review of the literature. Arch Gynecol Obstetr 2007;276:189-92.
- Haram K, Svendsen E, Abildgaard U. The HELLP syndrome: Clinical issues and management. A Review. BMC Pregnancy Childbirth 2009;9:8.
- Sibai BM. The HELLP syndrome (hemolysis, elevated liver enzymes, and low platelets): Much ado about nothing? Am J Obstet Gynecol 1990;162:311-6.
- Karateke A, Silfeler D, Karateke F, Kurt R, Guler A, Kartal I, et al. HELLP syndrome complicated by subcapsular hematoma of liver: A Case report and review of the literature. Case Rep Obstet Gynecol 2014;2014:585672.
- Seren G, Morel J, Jospe R, Mahul P, Dumont A, Cuileron M, et al. HELLP syndrome and ruptured subcapsular hepatic haematoma. Case report and therapeutic options. Ann Fr Anesth Reanim 2006;25:1067-9.