Nutrition Knowledge, Attitudes, and Dietary Intake of Women of Reproductive Age in Bundabunda Ward, Zambia
Allison M. Grech1, Robyn Alders2, Ian Darnton-Hill3, Brigitte Bagnol4, Doreen Hikeezi5, Fiona O'Leary1
2.School of Veterinary Science and School of Life and Environmental Sciences and The Charles Perkins Centre, The University of Sydney, New South Wales 2006, Australia.
3.The Boden Institute of Obesity, Nutrition, Exercise and Eating Disorders, University of Sydney, NSW, 2006, Australia.
4.The South Africa and Kyeema Foundation, Brisbane, Australia and The University of the Witwatersrand, Johannesburg, South Africa.
5.Department of Food Science and Technology, School of Agricultural Sciences, University of Zambia, Lusaka, Zambia.
Citation :Grech AM, Alders R, Hill ID, Bagnol B, Hikeezi D, O'Leary FM. Nutrition Knowledge, Attitudes and Dietary Intake of Women of Reproductive Age in Women in Bundabunda Ward, Zambia. Clin J Nutr Diet 2018;1(2):1-12.
Forty percent (%) of Zambian children under age 5 were stunted in 2013. Stunting begins with a woman's pre-pregnancy nutrition status and is often associated with poor dietary diversity, including low intake of animal-source foods (ASFs). This study assessed food attitudes, dietary intake of women of reproductive age (WRA), and costs of key nutrients in Bundabunda Ward, Zambia. A mixed-method approach was used, including participatory observation, focus-group discussions with WRA (nulliparous adolescents and pregnant, breastfeeding, and multiparous women), interviews with community health workers (CHWs), and nutritional analysis of WRA's diets (n = 33). The study found WRA and CHWs considered nutrition to be important, but a lack of financial resources, inflexible complementary feeding advice, and competing priorities compromised their dietary quality. All WRA's diets were high in maize and other plant-based foods, and relatively low in ASFs and wild foods. WRA were unlikely to meet their metabolic demands for some amino acids, namely, lysine and tryptophan. Mean iron intake in adolescents was inadequate and calcium intake across groups met less than 50% of requirements (recommended nutrient intake). However, mean intake of energy, protein, zinc, and vitamin A across all groups appeared adequate compared to the recommended intake for lifestage. Further efforts on community and national levels, including strengthening the teaching capacity of CHWs in nutrition; increasing the availability, accessibility, and utilization of ASFs; and further development of context-specific food-based guidelines, are necessary to ameliorate food security challenges that underpin the ongoing high prevalence of micronutrient deficiencies and stunting in Bundabunda Ward and similar contexts.
Dietary intake, infant nutrition, maternal nutrition, stunting, Zambia
INTRODUCTION
As an indicator of chronic undernutrition, stunting reflects the inability of individuals to reach their growth potential and is increasingly considered the most consequential form of undernutrition globally [1,2]. With multiple short-, medium-, and long-term sequelae, including linear growth retardation, neurodevelopmental impairment, elevated susceptibility to infection,[3] and an increased risk of metabolic disease,[4] stunting compromises the learning and economic capacity of individuals and impedes their ability to escape intergenerational cycles of poverty [5-7].
The process of stunting begins with a woman's preconceptional nutrition status, continuing in utero and into infancy [6-8]. These "first 1,000 days" between conception and a child's second birthday represent a period of critical developmental importance. Poor dietary diversity, including low intake of animal-source foods (ASFs), often with concomitant exposure to infectious disease, can compromise availability of protein and micronutrients including iron, vitamin A, folate, zinc, and calcium, all of which are critical for optimal growth and development [6-11].
A mother's own birth weight,[12,13] her eventual stature, and subsequent health and societal influences,[14] including nutritional status before pregnancy, cumulatively influence infant birth size and disease risk. Post-natally, suboptimal breast- and complementary feeding practices contribute to ongoing, often permanent, growth impairment [5,7,15]. Efforts to reduce stunting prevalence should therefore aim to optimize nutrient stores in young women before pregnancy, continuing throughout the life course [16,17].
Despite an aim to reduce stunting prevalence to 30% in the National Food and Nutrition Strategic Plan for Zambia (2011-2015), data from the 2013-2014 Zambia Demographic and Health Survey indicated that 40% of Zambian children under age 5 were stunted [18]. Vitamin A and iron deficiency affected more than 50% of children under 5 years. Likewise, iron-deficiency anemia affected 36% of pregnant women[17,19] and 29% of breastfeeding women [20]. A 2013 food consumption survey conducted in women and children in two provinces in Zambia showed that 15% and 87% of children under 5 were also deficient in zinc and vitamin B12, respectively. Vitamin B12 deficiency also affected 95% of women surveyed [21].
While supplementation and food fortification have played an important role in addressing micronutrient deficiencies in Zambia, they require ongoing reinforcement [22,23] as their sustainability is challenged by funding, supply and access issues, low acceptability, and/or poor compliance [14]. Interventions to optimizediets should focus on locally available foods (including wild foods, which can be highly nutritious), consider seasonal differences in food access and optimize the use of local resources, including health-care staff, in order that they are acceptable, sustainable, and therefore effective [24-27].
This study was nested within a larger project entitled "Strengthening food and nutrition security through family poultry and crop integration in Tanzania and Zambia," which seeks to test opportunities to enhance women's role in improving household nutrition and reducing childhood undernutrition [25]. The aims of this study were to investigate the nutrition beliefs and behaviours of women of reproductive age (WRA), determine the nutritional adequacy of WRA's diets and propose flexible, acceptable, and feasible food-based recommendations (FBRs) to optimize diets for WRA using food available during the dry and hot season, in Bundabunda Ward, Zambia.
METHODS
Fieldwork was conducted in Bundabunda Ward, 150 km Northeast of Lusaka, within agroecological zone one (annual rainfall of less than 800 mm) [18]. The total population of Bundabunda Ward was estimated to be 14,305 people, the majority of whom earned income through smallholder agriculture and subsistence farming [17]. The Chinyunyu Rural Health Centre (CRHS) has a catchment population of 10,274 and is the primary site of ante- and post-natal care delivery in the Ward [28]. The site had not previously been involved in a nutrition research intervention.
In Zambia, the overall literacy rate was 70.2% (60.5% in rural and 83.8% in urban areas) with 73.2% of men and 67.3% of women being literate [29]. In Bundabunda Ward, the Soli and Nyanja languages are commonly spoken [30].
The broader project to which this study contributes, "Strengthening food and nutrition security through family poultry and crop integration in Tanzania and Zambia," previously received ethics approval by the Tropical Disease Research Centre Ethics Review Committee in Zambia (#2811) and the University of Sydney Human Ethics Research Committee (#2014/209).
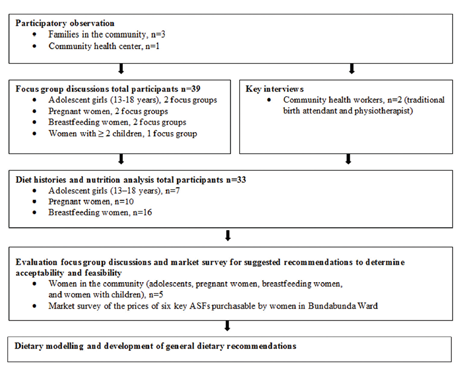
A mixed-method approach was used. Qualitative and quantitative data collection occurred during September 2015, in the hot and dry season (July to late October), when food insecurity was expected to be greatest [31]. Data were collected in four phases. Phase 1 consisted of unstructured observations of meals consumed in households; phase 2 comprised key informant interviews with community health workers (CHWs) and focus groups with WRA; phase 3 included collection of dietary data using the research diet history method; and phase 4 involved a food basket market survey.
Stratified purposeful and convenience sampling methods were used [32]. Community leaders from the Ward identified participants (nulliparous adolescents, pregnant women, breastfeeding women, and women with ≥1 child over 2 years of age) for phase 1 of meal observations. WRA attending the health center for clinic visits were recruited for focus group discussions (FGDs) and dietary intake interviews. CHW employed at the health centers and responsible for providing nutrition advice to women were recruited for in-depth interviews.
All qualitative data were collected using questionnaire frameworks developed by researchers with previous experience working in Zambia, a trained nutrition researcher, and an experienced translator. FGDs were used to investigate nutrition knowledge, sources of information, and food behaviors of WRA both before and during pregnancy and throughout breastfeeding and weaning. FGD was undertaken using a semi-structured interview method, were audio-recorded and translated. All FGD transcriptions were read thoroughly and codes and themes developed using an iterative process. Recruitment and data collection were conducted until thematic saturation was achieved [33]. In-depth interviews with health staff were designed to elicit information on the perceived nutrition issues, modes, and range of nutrition advice provided to WRA, before and during pregnancy and throughout breastfeeding and weaning. Interviews used a standard discussion guide, and a list of guiding questions and probes, and were recorded, translated and transcribed.
The structured diet history [34] is an interviewer-administered, detailed, retrospective dietary assessment method. It comprises a 24 hour recall and a food frequency questionnaire [35] using a standard format to elicit usual eating patterns, clarify quantities of dietary intake including portion size and frequency of consumption. Portion sizes were quantified using three different spoons of the same size and shape to those commonly used by WRA. Spoon volumes were converted to weights to the nearest gram using digital kitchen scales (Mainstays Slimline Digital Scale EK9150K). Vegetable oil intake was estimated at 5 mL per day per person, using information ascertained from mealtime observations and diet histories. This method was chosen as it has low respondent burden, and allowed collection of comprehensive usual intake data in non-literate individuals in one interview session. All the study participants provided written consent after explanation in their local language by the translator.
Nutritional adequacy of participants' diets was determined by applying Zambian food composition table (FCT) data to the diet history information [36,37] using Microsoft Excel. Where Zambian FCT data were incomplete, values were imputed from FCTs developed for Tanzania,[38] Mozambique,[39] and other African databases, where necessary [Supplementary Appendix].
Energy, protein, iron, zinc, calcium, and vitamin A intake were analyzed. Nutrient intake was expressed as a percentage (%) of requirements at each life stage (adolescence, pregnancy, and breastfeeding) as determined by the recommended nutrient intake (RNI) published by the World Health Organization (WHO) [40,41] The RNI is defined as the average daily dietary nutrient intake that is sufficient to meet the nutrient requirements of almost all (97.5%) of healthy individuals in a particular life stage, age, and gender group [40]. RNI for each life stage was determined using the WHO values using the following assumptions: Moderate physical activity level with additional requirements for pregnancy (average of additional needs across trimesters used) and lactation (0-6 months post-partum),[42] average body weight (adolescents 54.4 kg and adults 55 kg);[41] calcium requirements based on average daily animal protein intake 20-40 g;[41] iron requirements based 5-10% bioavailability; zinc RNI assuming moderate bioavailability (7.5%); and the highest requirement for pregnancy (third trimester) and lactation (0-3 months post-partum) [41].
A market survey was conducted on a food basket of six ASFs accessible in the dry and hot season using purchases from two stallholders and reports on usual prices by WRA. Using the basket of ASFs collected and FCT data, the cost per unit (100 g, mg or µg) of protein, iron, zinc, calcium, and vitamin A was analyzed per food.
RESULTS
The study flow chart and number of participants from the four phases of data collection can be found in Figure 1.
Observation sessions over three meal times with families of WRA in which food was prepared and consumed were conducted. A further four observations were carried out at one CRHS to appreciate the environment in which dietary information and nutrient supplementation are provided to WRA by CHWs.
Seven FGDs with 6-12 participants in each (total n = 49) were conducted until thematic saturation was reached. All participating WRA recognized the importance of adequate nutrition for good health across the life course, including the role of nutrition in supplying mothers with energy and "blood" for a healthy pregnancy. A pregnant woman stated, "...(Nutrition is important) to protect the baby and help the baby inside to grow well and fast and to help the mother herself to have energy during the delivery. Sometimes the women cannot push properly during delivery and the nurses cannot even help them enough, because the woman has not been eating well."
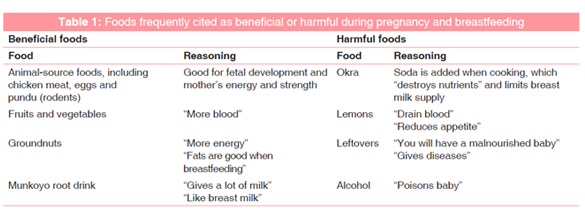
While some foods were commonly cited as either beneficial or harmful [Table 1], women also suggested a sense of intuition guided food intake during pregnancy and breastfeeding. A young nulliparous woman understood that the best foods to eat during pregnancy "...come to your heart, to your appetite,"while a breastfeeding woman suggested "there's no food that is not good. Sometimes no to meat, sometimes no to eggs, just up to you."All groups suggested that women have poor appetites during pregnancy, improving post-partum. A pregnant woman stated, "When you are breastfeeding, you are now eating too much food... it's like there is a big hole that has remained there, so you need to fill that hole so the baby can grow."
The importance of human breast milk for infants and the recommendation of exclusive breastfeeding for 6 months were well known to participating WRA. A young, nulliparous woman stated she learned at school that, "...a mother's milk gives nutrients, protects from diseases and will help the baby have a good brain."
Women reported introducing solid foods to their infants from 5 months, continuing breastfeeding until their children were approximately 18 months old. Participants explained that infants were weaned before 6 months if mothers developed sore and/or crackled nipples, were HIV positive or otherwise unwell or become pregnant. WRA reported adding hot chilli or other deterrents to their nipples to wean infants quickly.
Other foods considered optimal for infants included porridge made with fine mealie meal (a version of the corn staple food, nshima) with an added protein source (e.g., mashed eggs, groundnuts, kapenta, or beans), fruit and drinks made from fermented munkoyo root (Rhynchosia insignis). Okra and food leftover after meals were considered harmful. Some breastfeeding women avoided providing meat to their children since, although meat is rarely eaten alone, "When you give too much meat to a child, she will start refusing nshima and only want meat!" Although WRA suggested that CHWs were figures of authority whose health advice was trusted by their communities, they expressed concern about their inability to follow CHWs' advice, due to financial and time restraints: "The health workers tell us we must have special times and special diets for babies, (but) that can only work if we have enough food to give."
A total of three CHWs employed at CRHS were regularly present at the clinic during the data collection period. In-depth interviews were held with two CHWs who provided nutrition advice to women. CHWs considered women's nutrition knowledge to be low. CHWs provided nutrition education to women attending ante- and post-natal clinics and through monthly village outreach programs, which included demonstrations of food prepared for infants (e.g., maize porridge). A traditional birth attendant reported receiving annual nutrition training, where she learned about "balanced diets" comprising "energy foods, bodybuilding foods and protective foods." CHWs were responsible for providing and educating women on the importance of micronutrient supplements in "adding more blood" and "giving appetite" during pregnancy. CHWs also weighed infants; however, there was an observed lack of time and resources to adequately assess infants' individual growth trajectories.
When considering complementary feeding, CHWs suggested that a specific feeding schedule was important, "...starting with a light porridge at 10:00. At 12:00, then they can give porridge or anything else like fruit, and then at 15:00, they give again porridge." CHWs highlighted the potential nutritional significance of wild foods to infants' diets but suggested that WRA did not recognize these foods as nutritious: "These women should come to realise that the traditional food that we have, if well-prepared and well-mixed, is nutritious enough to sustain their children, and they shouldn't think that they need to go and buy things from town."
A lack of useful resources to aid health education was also reported to compromise CHWs' ability to effectively deliver health messages. Women were not provided resources to aid their understanding at clinic visits or information to take home. Posters displayed at the clinic were old, damaged and predominately written in English. One CHW suggested that since "most of the women do not read," picture-based resources would be more effective.
Women agreed that information pamphlets, booklets, or magazines to take home would aid their own learning and engage their husbands in understanding the importance of nutrition for their partners and children. As a breastfeeding woman suggested, "You give us, we take, when we go home we can read slowly and learn more... The husband can be happier and more supportive for their children because they would be getting information from the same magazines as us."
A total of 33 WRA provided usable dietary histories including 7 adolescents, 10 pregnant women and 16 women currently breastfeeding.
For all groups, the usual dietary intake of women comprised three, predominately plant-based, meals per day. Meals typically included maize (as nshima, porridge or samp, made from large groats of maize) with small amounts of plant foods and less frequently, ASFs (fresh/dried fish or kapenta [small dried fish], chicken, or goat), consumed as accompaniments or relishes. Overall, women (n = 33) consumed between 7 and 16 (mean = 11, SD 2.2) different foods in the previous month, excluding sugar and cooking oil. A total of 38 foods and 4 beverages were reported across participants.
The average energy intake across groups was 2651 kcal/day, SD 765 kcal. While apparent energy intake means exceeded the RNI according to life stage for all groups of WRA, the reported diets of six women (18%) failed to meet their estimated energy requirements. The mean contribution of protein, fat, and carbohydrate to total energy intake were 10% (SD 1%), 13% (SD 2%), and 77% (SD 3%), respectively. Mean energy, protein, iron, zinc, calcium, and vitamin A intake, adequacy and contribution by food group, for nulliparous, pregnant, and breastfeeding women are shown in Tables 2-4, respectively.
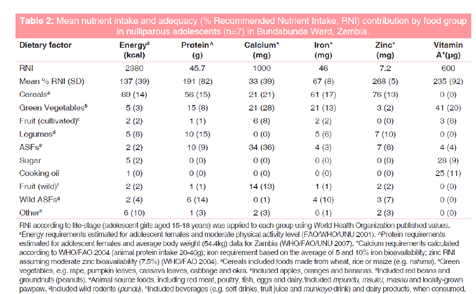
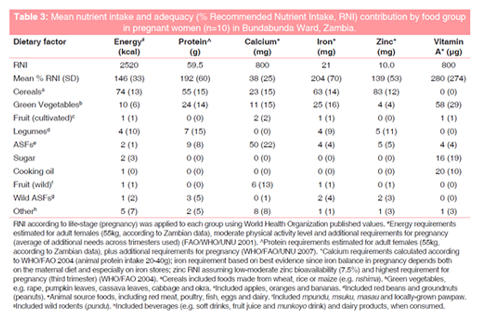
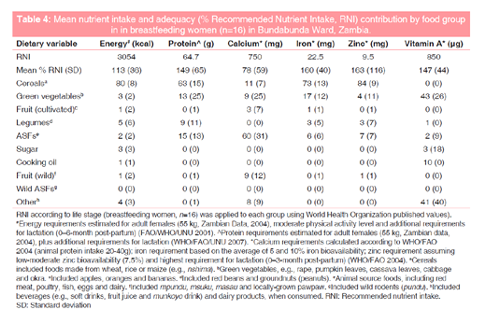
Cereals, largely comprised maize, were major contributors to energy and nutrient intake [Tables 2-4]. The mean daily intake of nshima was 2023 g (SD 820 g), contributing 68% energy (SD 13%), 53% protein (SD 16%), 56% iron (SD 20%), and 68% zinc (SD 28%) to women's diets. Samp and maize porridge contributed 5% (SD 2%) and 2% (SD 1%) of energy to consumers, respectively.
Groundnuts, sugar, and sugar-sweetened beverages (SSBs), contributed a mean 11% (SD 9%), 6%, (SD 3%) and 4% (SD 5%) to energy intake, respectively. Fortified sugar (10 µg/g) was also a major source of vitamin A, contributing a mean 28% (SD 23%) to total intake. Other important vitamin A sources included rape, vegetable oil, and kapenta, contributing 33% (SD 21%), 26% (SD 14%), and 6% (SD 8%) to total vitamin A intake, respectively.
90% of participants reported weekly intake of ASFs. Wild foods (predominately fruits) were consumed by 61% of participants each week and also included leaves, wild caterpillars, and rodents. ASF intake ranged from 0 to 171 g/ day (Mean 41 g and SD 46), with the highest consumers of ASFs regularly consuming wild rats ("pundu," Tatera leucogaster). When analyzed according to iron type, mean contribution of haem iron from ASFs was 5% (SD 6%), with the remaining 95% (SD 6%) comprising non-haem iron.
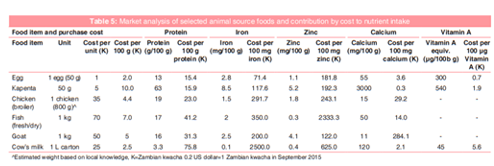
Table 5 highlights the cost per unit of protein, iron, zinc, calcium, and vitamin A for six ASFs. Chicken egg was the most cost-effective source for the majority of nutrients analyzed including protein, iron, and vitamin A. Kapenta was the most cost-effective for calcium and goat for zinc.
DISCUSSION
This study examined attitudes and behaviors regarding nutrition, dietary adequacy, and opportunities to feasibly optimize nutrient intake for WRA and infants in Bundabunda Ward, Zambia. Both WRA and CHWs consider nutrition to be important for women and infants, recognizing the unique significance of nutrition during pregnancy, breastfeeding, and weaning for their children's growth and development. Despite women's interest in positive nutrition behaviors, a combination of factors, including a lack of financial resources, inflexible complementary feeding advice and competing priorities, compromised the quality of women's diets, characterized by a reliance on maize, and other plant-based foods and low consumption of ASFs.
International literature indicates that maternal education about breastfeeding and complementary feeding is associated with improved height-for-age z-scores in children [22,43,44]. Women attributed their nutrition knowledge to CHWs, trusted sources of health information in Zambia [45] and in similar contexts [24,46].
However, advice from CHWs that infants required "special porridge" was challenging in practice, as it required preparing separate meals. Guidance regarding how to modify family meals such that they are suitable for infants could include providing a child nshima from the family pot by mixing a small portion (the size of an egg, i.e. 2-3 tablespoons) with carefully mashed relish prepared for the household would be more practical. In addition, while education on different foods and their roles is provided, the importance of food diversity, including the role of ASFs in providing protein and micronutrients, could be further emphasized by CHWs. A recent study highlighted that participatory community-based nutrition education improved child dietary diversity in food insecure areas in Malawi [46].
CHWs indicated more nutrition training and resources were needed, including visual teaching materials. The Zambian National Food and Nutrition Commission previously highlighted that investment in posters (especially showing local foods in food groups and demonstrating hygienic practices), picture information cards and booklets is required [45]. Storytelling approaches and flip charts have previously been used in Zambia for nutrition education for people with HIV/AIDS,[47] and have been shown to be effective health promotion tools in similar contexts [48,49].
Women indicated the need for greater support from their partners in accessing the financial and social capital necessary to access foods important for their family's health. Breastfeeding advocacy should extend to those who influence women's decisions to breastfeed, that is, her partner and extended family, as well as community leaders who may have considerable influence in village settings [50]. "Take-home" resources such as pamphlets may further assist to provide credible information and advice to supplement clinic-based education delivered to WRA and to mitigate the commonly low attendance of fathers at antenatal clinics.
It is increasingly understood that adolescence represents a frequently overlooked window of opportunity for nutrition interventions in the prevention of stunting [13,51]. Since stunted young women often have stunted offspring,[7] establishing healthy nutrient stores with diverse diets in young women before pregnancy, as emphasized by the "first 1000 days" approach, may attenuate the risk of stunted children [13,52]. In this study, adolescents indicated that health education in schools was a major source of their nutrition knowledge. Previous research by our group[26] also indicated that adolescent girls are also the most likely to consume potentially nutritious wild foods, including ASFs, compared with pregnant and breastfeeding women [53].
Dietary analysis showed almost one-fifth of WRA did not regularly consume diets adequate in energy. On average, maize supplied more than two-thirds of total energy, highlighting the low diversity of these women's diets.
The contribution of energy from protein (10%) in this sample is commensurate with previously published results for Zambia,[54]. and represents the lower limit of the WHO's recommendation (10-15% of energy intake) [55]. Further, the overall quality of protein was poor, with nshima contributing up to 80% of protein intake in some participants. Due to the substantial contribution of maize to total protein intake and a probable inadequacy of some amino acids, namely lysine and tryptophan,[56] the capacity for women's diets to satisfy their metabolic demand for amino acids and nitrogen is likely to be compromised [40].
Similarly, while the mean iron and zinc intakes of WRA were considered adequate according to FAO/WHO recommendations (except for iron in female adolescents),[39] the bioavailability of these micronutrients is likely to be low due to a reliance on maize and infrequent and small portions of ASFs and plant-based alternatives (e.g., beans and groundnuts). The inhibitory effect of phytate in maize and tannins in black tea often consumed with breakfast in this group may also contribute since they strongly inhibit iron absorption [39,57-59]. However, the effect of phytate is debated,[60] and refined nshima (lower in phytate) was mostly consumed. Further, while demonstrated to be effective in similar contexts,[61] WRA suggested that minimizing the phytate content of maize (e.g., by soaking) is not acceptable or feasible in the dry and hot season, where access to water is limited. Nevertheless, the development of practical guidelines for enhancing iron absorption, including planning intake of ASFs or vitamin C containing vegetables or fruits with meals, and consuming tea at least half an hour before or after food,[62] could be integrated into health messaging.
This study highlights the low consumption of ASFs in WRA, consistent with literature highlighting the uneven global distribution of ASFs, determined largely by wealth status [63]. ASFs have considerable potential to improve nutrient intake through highly digestible, complete protein and bioavailable micronutrients including iron, zinc, vitamin B12, vitamin A, and calcium [64]. However, a notable decline in the availability of ASFs and pulses in Zambia alongside an increase in the supply of cassava and vegetable oils in the past 50 years [9] has diminished the capacity of Zambians to access ASFs due to rising prices of these foods.
For pregnant and breastfeeding women, ASFs supply rich sources of bioavailable micronutrients [14,64]. For breastfed children, the nutrients for which at least 75% must come from complementary foods - iron (97-98%), zinc (80-86%), and vitamin B6 (80-90%) - are difficult to consume in adequate amounts without ASFs, fortified foods, or micronutrient supplements, particularly for non- or minimally breastfed children [65,66] There is an inverse association between meat intake and stunting[67] and evidence supports promotion of ASFs in enhancing child growth [66]. The WHO recommends meat, poultry, fish, and/or egg intake daily or as often as possible for infants 6-23 months of age [65]. A recent study used dietary modeling with FAO Food Balance Sheet data to identify several potential deficiencies in the Zambian diet, including protein, lysine, calcium, zinc, available iron, and vitamins A, B2, B12, and D. They demonstrated supplementation with small amounts of milk and meat would reduce the probability of inadequacy of these nutrients compared to supplementation with additional plant-based foods [9].
In particular, the present study highlights the inadequate calcium intake of WRA, with mean intakes of calcium below half of requirements in all groups. Dairy products were rarely consumed and intake of other calcium-rich foods was low, for example, fish with bones (e.g., kapenta). Our "cost-to-nutritional-benefit" analysis showed that the daily addition of 12 g (approximately one tablespoon) of kapenta to a pregnant woman's diet contributes one-third of her calcium requirements. Using the mean calcium intake of pregnant women in this sample, this addition represents an improvement from 28% adequacy to 61%. However, the volatility of kapenta prices in Zambia may influence its ongoing cost-effectiveness [68]. Alternative calcium sources, such as ground chicken bones or eggshells present opportunities, though their use requires further research [69].
The contribution of wild foods to women's diets Wild foods have the potential to contribute significantly to the nutrition of WRA in Bundabunda Ward and similar contexts. While consumed by almost two-thirds of WRA and reported by these women to be healthful, their reported consumption did not appear to increase in periods of food scarcity or when readily available, including the dry and hot season [27]. CHWs considered women's lack of knowledge regarding the nutritional benefit of wild foods prohibitive to their frequent consumption. Promotion of wild food intake, including fruits and ASFs such as rodents (pundu), caterpillars, and insects, which may be preserved, could increase consumption of wild foods and therefore nutrient intake.
This study demonstrates that fortification and supplementation under current conditions help to meet some nutritional requirements in vulnerable groups. Vitamin A-enriched sugar, for example, contributed, on average, to over a quarter of WRA's vitamin A intake in this sample and is estimated to have reduced the prevalence of inadequate intake in Zambia from 87% to 79% [70]. However, consumption of other vitamin A-containing foods in this population was low, including ASFs and sufficient quantities of fruits and vegetables high in beta-carotene.
Antenatal supplementation of iron and folic acid is provided by all health facilities in Zambia, though the Zambian Health survey shows less than 60% of women took these for more than 90 days [18]. Ongoing advocacy for supplementation of iron and folic acid during pregnancy is crucial given the difficulty in achieving adequate intake with the local diet alone, but further efforts are required to increase availability, accessibility, and utilization of foods containing iron and folic acid, especially ASFs [14,39].
This study applies to Bundabunda Ward, Zambia, during the hot and dry season, using a small, largely convenience sample. While not generalizable, it presents a relatively simple model for identifying nutrition issues, developing recommendations, and designing interventions according to the needs and opportunities of similar communities.
The limitations of data in the of FCTs for Zambia and across Africa are significant, affecting nutrition research and policy [71,72]. In this study, folate, vitamin B12, and iodine were not assessed since they are not yet analyzed in Zambian FCTs, however, they are important micronutrients in pregnancy and are likely to be inadequate in this population second largely to low intake of ASFs and low dietary diversity [9,73]. Alternative datasets were required to "fill the gaps" in nutrition data and ascertain nutrient values for prepared foods, rather than uncooked foodstuffs, for example, maize flour versus nshima. Other foods not included in FCTs, including wild foods and ASFs such as offal, were not extensively consumed by this sample but may have important nutritional impacts on women's and infant's diets. Using currently available food composition data for Zambia, these foods lack substantive nutrition information to develop robust, evidence-based recommendations about their consumption.
Analysing nutrient intake using FCTs, while feasible, also does not take into account interactions between foods consumed together. This is important for nutrients including iron and zinc, which are particularly susceptible to the inhibitory and enhancing effects of other meal elements and are likely affected by the low ASF content of Zambian diets. As such, our intake estimates may be somewhat different to the amount of utilizable nutrient in women in this sample.
Dietary intake assessment is challenging; however, efforts in reducing error using spoons regularly used by women in the community and triangulating research methods (mealtime observations, FGDs, and diet histories) were made to enhance the validity of captured data. While subject to error and misreporting, especially in estimation of portion sizes,[74] the diet history method may overestimate intake [35] but does provide detail when considering usual intake, and allows the substantial variability in nutrient intake across days and subjects to be highlighted. In particular, intake of ASFs, though low, would not be adequately represented if 24-h recalls were used. The contribution of iron and folic acid supplementation to the nutrient intake of pregnant women was also not included due to variable and uncertain rates of uptake.
RNIs used to evaluate nutritional adequacy change across the life course, including the stages of pregnancy [40-42]. This study did not categorize women according to pregnancy stage since many women were unable to provide an estimated delivery date.
As such, nuances in nutrient requirements across the gestation period, especially iron, are not addressed. WRA in this sample may also have increased requirements when disease incidence is high; however, since these additional needs cannot be reliably estimated, they were not included in our analysis.
CONCLUSION
This study presents a small-scale model for identifying nutrition issues, and developing recommendations and interventions that consider local needs and opportunities. While the importance of optimal nutrition across the life course is deeply valued by WRA in Bundabunda Ward, strategies including those strengthening the teaching capacity of CHWs; increasing the availability, accessibility, and utilization of ASFs; and further development of context- and season-specific food-based guidelines are necessary to address the ongoing high prevalence of micronutrient deficiencies and stunting in Bundabunda Ward and in similar contexts. Aligning these efforts with ongoing efforts on community and national levels, including the Zambian National Food and Nutrition Strategic Plan, which focuses on the "first 1000 days" as a crucial period for nutrition intervention is essential. In addition, increased attention to the diets of adolescent females for whom optimizing nutrient stores can have a profound impact on future generations is essential to ensure sustained improvements in the nutrition of WRA and their future children.
ACKNOWLEDGMENTS
The authors would also like to acknowledge the supportive staff involved in the research both in Zambia and Sydney, who generously shared their time and expertise: Mu Li (The University of Sydney), Hilda Lumbwe (Ministry of Agriculture and Livestock, Zambia), and Agnes Aongola (Ministry of Health, Zambia). Special thanks to the study participants and community leaders in Bundabunda Ward, Zambia, who shared their knowledge and experiences for the purpose of this research.
This study was part of a project (FSC/2014/101) funded by the Australian Centre for International Agricultural Research and the Government of Zambia.
REFERENCES
- Hautvast JL, Tolboom JJ, Kafwembe EM, Musonda RM, Mwanakasale V, van Staveren WA, et al. Severe linear growth retardation in rural Zambian children: The influence of biological variables. Am J Clin Nutr 2000;71:550-9.
- UNICEF, WHO, World Bank. Levels and Trends in Child Malnutrition: UNICEF-WHO-The World Bank Joint Child Malnutrition Estimates. New York, USA: UNICEF; Geneva, Switzerland: WHO; Washington DC, USA: The World Bank; 2012.
- Palmer AC. Nutritionally mediated programming of the developing immune system. Adv Nutr 2011;2:377-95.
- Chango A, Pogribny IP. Considering maternal dietary modulators for epigenetic regulation and programming of the fetal epigenome. Nutrients 2015;7:2748-70.
- Branca F, Ferrari M. Impact of micronutrient deficiencies on growth: The stunting syndrome. Ann Nutr Metab 2002;46 Suppl 1:8-17.
- Dewey KG, Begum K. Long-term consequences of stunting in early life. Matern Child Nutr 2011;7 Suppl 3:5-18.
- Prendergast AJ, Humphrey JH. The stunting syndrome in developing countries. Paediatr Int Child Health 2014;34:250-65.
- Christian P, Lee SE, Donahue Angel M, Adair LS, Arifeen SE, Ashorn P, et al. Risk of childhood undernutrition related to small-for-gestational age and preterm birth in low- and middle-income countries. Int J Epidemiol 2013;42:1340-55.
- Zhang Z, Goldsmith PD, Winter-Nelson A. The importance of animal source foods for nutrient sufficiency in the developing world: The Zambia scenario. Food Nutr Bull 2016; pii: 0379572116647823.
- Gluckman PD, Hanson MA, Pinal C. The developmental origins of adult disease. Matern Child Nutr 2005;1:130-41.
- Abu-Saad K, Fraser D. Maternal nutrition and birth outcomes. Epidemiol Rev 2010;32:5-25.
- Ramakrishnan U, Martorell R, Schroeder DG, Flores R. Role of intergenerational effects on linear growth. J Nutr 1999;129:544S-549S.
- Prentice AM, Ward KA, Goldberg GR, Jarjou LM, Moore SE, Fulford AJ, et al. Critical windows for nutritional interventions against stunting. Am J Clin Nutr 2013;97:911-8.
- Darnton-Hill I, Mkparu UC. Micronutrients in pregnancy in low-and middle-income countries. Nutrients 2015;7:1744-68.
- Darnton-Hill I, Nishida C, James WP. A life course approach to diet, nutrition and the prevention of chronic diseases. Public Health Nutr 2004;7:101-21.
- Bwalya BB, Lemba M, Mapoma C, Mutombo N. Factors associated with stunting among children aged 6-23 months in Zambia: Evidence from the 2007 Zambia demographic and health survey. Int J Adv Nutr Health Sci 2015;3:116-31.
- Central Statistical Office Zambia, Ministry of Health Zambia, University of Zambia Teaching Hospital, Tropical Diseases Research Centre Zambia, University of Zambia. Zambia Demographic and Health Survey 2013-2014. Maryland, USA: Calverton; 2015. p. 1-518.
- Stevens GA, Finucane MM, De-Regil LM, Paciorek CJ, Flaxman SR, Branca F, et al. Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995-2011: A systematic analysis of population-representative data. Lancet Glob Health 2013;1:e16-25.
- Kafwembe EM. Iron and vitamin A status of breastfeeding mothers in Zambia. East Afr Med J 2001;78:454-7.
- Harris J, Haddad L, Grutz SS. Turning Rapid Growth into Meaningful Growth: Sustaining the Commitment to Nutrition in Zambia. Brighton, UK : Institute of Development Studies Special Collection; 2014.
- Bhutta ZA, Das JK, Rizvi A, Gaffey MF, Walker N, Horton S, et al. Evidence-based interventions for improvement of maternal and child nutrition: What can be done and at what cost? Lancet 2013;382:452-77.
- Zerfu TA, Ayele HT. Micronutrients and pregnancy; effect of supplementation on pregnancy and pregnancy outcomes: A systematic review. Nutr J 2013;12:20.
- Haines A, Sanders D, Lehmann U, Rowe AK, Lawn JE, Jan S, et al. Achieving child survival goals: Potential contribution of community health workers. Lancet 2007;369:2121-31.
- Traore M, Thompson B, Thomas G. Sustainable Nutrition Security: Restoring the Bridge between Agriculture and Health. Rome, Italy : FAO; 2012.
- Alders R, Aongola A, Bagnol B, de Bruyn J, Kimboka S, Koch R, et al. Using a One Health Approach to Promote Food and Nutrition Security in Tanzania and Zambia. 2nd ed. Davos, Switzerland: GRF One Health Summit; 2013. p. 17-20.
- Huber U. Wild foods in Bundabunda ward Zambia: An assessment of diversity and potential contribution to food and nutrition security. In: Master of Science in One Health (Infectious Diseases). UK: University of London; 2015.
- Powell B, Thilsted SH, Ickowitz A, Termote C, Sunderland T, Herforth A. Improving diets with wild and cultivated biodiversity from across the landscape. Food Security 2015;7:535-54.
- Ministry of Health, Zambia. The 2012 List of Health Facilities in Zambia. Lusaka, Zambia : Ministry of Health, Zambia; 2013. p. 1-252.
- Central Statistical Office Zambia. Zambia 2010 Census of Population and Housing. National Analytical Report. Lusaka: Republic of Zambia, Central Statistical Office; 2012. p. 1-117.
- Bagnol B. Research Trip Report: Population Census and Participatory Rural Appraisal (PRA) in Bundabunda Ward, Rufunsa District in Zambia. Strengthening Food and Nutrition Security Through Family Poultry and Crop Integration in Tanzania and Zambia ACIAR FSC Project No FSC 2012/023; 2015.
- Famine Early Warning Systems Network (FEWS). Zambia Food Security Outlook. USA: USAID; 2015.
- Marshall MN. Sampling for qualitative research. Fam Pract 1996;13:522-5.
- Patton MQ. Enhancing the quality and credibility of qualitative analysis. Health Serv Res 1999;34:1189-208.
- Burke BS. The dietary history as a tool in research. J Am Diet Assoc 1947;23:1041-6.
- Fagundez LJ, Torres AR, Sanchez ME, de Torres Aured ML, Rodrigo C, Rocamora JA, et al. Diet history: Method and applications. Nutr Hosp 2015;31 Suppl 3:57-61.
- Lukmanji Z, Hertzmark E. Tanzania Food Composition Tables. Tanzania and Boston, USA: Muhimbili University of Health and Allied Sciences, Tanzania Food and Nutrition Centre and Harvard School of Pubic Health; 2008. P. 1-272.
- Ministry of Health, Zambia. Zambia Food Composition Tables. 4th ed. Zambia: Lusaka; 2007. p. 1-96.
- Korkalo L, Hauta-alus H, Mutanen M. Food Composition Tables for Mozambique. Finland: University of Helsinki; 2011. p. 1-55.
- WHO/FAO. Vitamin and Mineral Requirements in Human Nutrition. 2nd ed. Rome, Italy: WHO Technical Report Series; 2004. p. 1-341.
- WHO/FAO/UNU. Protein and Amino Acid Requirements in Human Nutrition. Geneva, Switzerland : WHO Technical Report Series; 2007.
- Human Energy Requirements: Report of a joint FAO/WHO/ UNU expert consultation. Food Nutr Bull 2005;26:166.
- Imdad A, Yakoob MY, Bhutta ZA. Impact of maternal education about complementary feeding and provision of complementary foods on child growth in developing countries. BMC Public Health 2011;11 Suppl 3:S25.
- Lassi ZS, Das JK, Zahid G, Imdad A, Bhutta ZA. Impact of education and provision of complementary feeding on growth and morbidity in children less than 2 years of age in developing countries: A systematic review. BMC Public Health 2013;13 Suppl 3:S13.
- National Food and Nutrition Commission (NFNC) and Infant and Young Child Nutrition Project (IYCN). Qualitative Assessment of Maternal Nutrition Practices in Zambia; 2010. p. 1-33.
- Kuchenbecker J, Reinbott A, Mtimuni B, Krawinkel MB, Jordan I. Nutrition education improves dietary diversity of children 6-23 months at community-level: Results from a cluster randomized controlled trial in malawi. PLoS One 2017;12:e0175216.
- National Food and Nutrition Commission Zambia and FANTA. Eating and Living Well with HIV and AIDS. USA : Good Nutrition Makes a Difference; 2011.
- Malhotra R, Lal P, Prakash SK, Daga MK, Kishore J. Evaluation of a health education intervention on knowledge and attitudes of food handlers working in a medical college in Delhi, India. Asia Pac J Public Health 2008;20:277-86.
- Takanashi K, Quyen DT, Le Hoa NT, Khan NC, Yasuoka J, Jimba M, et al. Long-term impact of community-based information, education and communication activities on food hygiene and food safety behaviors in Vietnam: A longitudinal study. PLoS One 2013;8:e70654.
- Langa L. Breast is always best, even for HIV-positive mothers. Bull World Health Organ 2010;88:9-10.
- Mora JO, Nestel PS. Improving prenatal nutrition in developing countries: Strategies, prospects, and challenges. Am J Clin Nutr 2000;71:1353S-63S.
- Black RE, Victora CG, Walker SP, Bhutta ZA, Christian P, de Onis M, et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013;382:427-51.
- Rodents AL. Food Security and Infectious Disease in Tanzania. BSc(Vet) (thesis). The University of Sydney; 2014.
- FAO. Nutrition Country Profile: The Republic of Zambia. Lusaka, Zambia: Nutrition and Consumer Protection Division, Food and Agriculture Organization of the United Nations; 2009.
- Nishida C, Uauy R, Kumanyika S, Shetty P. The joint WHO/ FAO expert consultation on diet, nutrition and the prevention of chronic diseases: Process, product and policy implications. Public Health Nutr 2004;7:245-50.
- FAO. Maize in Human Nutrition.: Food and Agriculture Organisation of the United Nations; 1992.
- Gillooly M, Bothwell TH, Torrance JD, MacPhail AP, Derman DP, Bezwoda WR, et al. The effects of organic acids, phytates and polyphenols on the absorption of iron from vegetables. Br J Nutr 1983;49:331-42.
- Schlemmer U, Frolich W, Prieto RM, Grases F. Phytate in foods and significance for humans: Food sources, intake, processing, bioavailability, protective role and analysis. Mol Nutr Food Res 2009;53 Suppl 2:S330-75.
- Gilani GS, Wu Xiao C, Cockell KA. Impact of antinutritional factors in food proteins on the digestibility of protein and the bioavailability of amino acids and on protein quality. Br J Nutr 2012;108 Suppl 2:S315-32.
- Miller LV, Hambidge KM, Krebs NF. Zinc Absorption Is Not Related to Dietary Phytate Intake in Infants and Young Children Based on Modeling Combined Data from Multiple Studies. Journal of Nutrition2 015 Aug;145(8):1763-9.
- Hotz C, Gibson RS, Temple L. A home-based method to reduce phytate content and increase zinc bioavailability in maize-based complementary diets. Int J Food Sci Nutr 2001;52:133-42.
- Zijp IM, Korver O, Tijburg LB. Effect of tea and other dietary factors on iron absorption. Crit Rev Food Sci Nutr 2000;40:371-98.
- Speedy AW. Global production and consumption of animal source foods. J Nutr 2003;133:4048S-4053S.
- Murphy SP, Allen LH. Nutritional importance of animal source foods. J Nutr 2003;133:3932S-3935S.
- Vossenaar M, Doak CM, Solomons NW. Challenges in the elaboration of a field interview instrument to capture information for the evaluation of adherence to the WHO/ PAHO guiding principles for complementary feeding of the breastfed child. Food Nutr Bull 2014;35:338-50.
- Dewey KG, Adu-Afarwuah S. Systematic review of the efficacy and effectiveness of complementary feeding interventions in developing countries. Matern Child Nutr 2008;4 Suppl 1:24-85.
- Krebs NF, Mazariegos M, Tshefu A, Bose C, Sami N, Chomba E, et al. Meat consumption is associated with less stunting among toddlers in four diverse low-income settings. Food Nutr Bull 2011;32:185-91.
- Chibuye M. The Impact of Rising Food Prices on Child Nutrition in Zambia. IDS Special Collection. Brighton, UK: Institute of Development Studies; 2014. p. 22-33.
- . Schaafsma A, Pakan I, Hofstede GJ, Muskiet FA, Van Der Veer E, De Vries PJ, et al. Mineral, amino acid, and hormonal composition of chicken eggshell powder and the evaluation of its use in human nutrition. Poult Sci 2000;79:1833-8.
- Fiedler JL, Lividini K, Zulu R, Kabaghe G, Tehinse J, Bermudez OI, et al. Identifying Zambia's industrial fortification options: Toward overcoming the food and nutrition information gap-induced impasse. Food Nutr Bull 2013;34:480-500.
- Afrofoods. Afrofoods' Arusha Declaration., Arusha, Tanzania: FANUS conference; 2015.
- de Bruyn J, Ferguson E, Allman-Farinelli M, Darnton-Hill I, Maulaga W, Msuya J, et al. Food composition tables in resource-poor settings: Exploring current limitations and opportunities, with a focus on animal-source foods in sub-Saharan Africa. Br J Nutr 2016;116:1709-19.
- Torheim LE, Ferguson EL, Penrose K, Arimond M. Women in resource-poor settings is at risk of inadequate intakes of multiple micronutrients. J Nutr 2010;140:2051S-8S.
- Poslusna K, Ruprich J, de Vries JH, Jakubikova M, van't Veer P. Misreporting of energy and micronutrient intake estimated by food records and 24 hour recalls, control and adjustment methods in practice. Br J Nutr 2009;101 Suppl 2:S73-85.
- Macdiarmid J, Blundell J. Assessing dietary intake: Who, what and why of under-reporting. Nutr Res Rev 1998;11:231-53.