Early Detection of Necrotizing Fasciitis Secondary to Group A Streptococcus: A Case Report
Joshua K. Phillips, Melanie Nukala, Vandana Grover, Peter Devito
Citation :Phillips JK, Nukala M, Grover V, Devito P. Early Detection of Necrotizing Fasciitis Secondary to Group A Streptococcus: A Case Report. Clin J Surg 2018;1(1):1-3.
Compartment syndrome is a known complication of necrotizing fasciitis (NF). We provide an interesting case report of a patient with a unique presentation of Type II NF and his subsequent management. A 31-year-old male with a recent history of bed bug bites presented to the ED with worsening swelling, pain, and pruritus along the entire left lower extremity. Furthermore, the patient's status was rapidly declining as he developed septic shock with acute kidney injury. Fasciotomy was performed for emergent decompression and infection source control; it proved to be both diagnostic and therapeutic. Intraoperative cultures were positive for Group A streptococcus. This case illustrates the importance of early surgical intervention to reduce morbidity and mortality in patients with high clinical suspicion of NF and the value of a complete history. Although compartment syndrome is uncommon in the absence of trauma, insect bites are a noted cause. Early recognition of compartment syndrome and NF is critical for appropriate surgical intervention and prevention of irreversible damage. The laboratory risk indicator for NF score may be useful for predicting the probability of a necrotizing soft tissue infection and aide in stratifying patients into risk categories. The patient in discussion possibly contracted this infection from bacteria introduced through breaks in the skin as a result of scratching the bed bug bites. Early detection of a possible necrotizing soft tissue infection and treatment of compartment syndrome proved to be lifesaving for this patient.
Case report, compartment syndrome, Group A streptococcus, necrotizing fasciitis.
INTRODUCTION
A small number of cases of acute compartment syndrome are due to non-traumatic causes such as insect bites. We provide an interesting case report of a patient with a very unusual presentation of necrotizing fasciitis (NF) and compartment syndrome and his subsequent management.
CASE REPORT
A 31-year-old male with a history of hypertension and gout presented to the emergency department of a community hospital for a 3-day history of worsening left lower extremity pain and. He reported significant swelling extending from the groin to foot making it difficult to mobilize. The patient initially attributed his symptoms to a gout flare and later presented to the hospital when he found no relief with colchicine. He then reported recent bed bug bites causing pruritus on the left foot before noticing the swelling. In addition, he experienced a single episode of vomiting followed by persistent diarrhea, cold sweats, dizziness, lightheadedness, and generalized weakness, for the past day. Since the onset of symptoms, he had experienced decreased urine output that was dark yellow in color. He denied paresthesias or trauma to the left lower extremity.
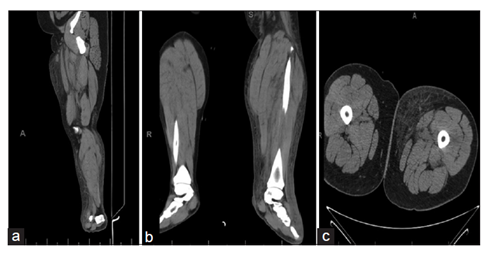
On examination, he was afebrile, hypotensive, tachypneic, and tachycardic to 140 beats/min. Examination of the left lower leg showed extensive swelling and tenderness around the left ankle extending up to the medial thigh, blistering in the posterior medial aspect of the left ankle, and previous bites on the toes along with palpable distal pulses. Presenting features raised suspicion for septic shock, acute compartment syndrome, NF, and/or deep venous thrombosis (DVT) as possible diagnoses. The left lower extremity ultrasound was negative for DVT and X-ray was consistent with soft tissue swelling. Computed tomography (CT) of the left tibia, fibula, and femur revealed extensive inflammatory change and edema involving both superficial and deep tissues [Figure 1a-c]. Laboratory evaluation was consistent with acute kidney injury and respiratory and metabolic acidosis; lactic acid 6.3, myoglobin 1810, BUN 59, creatinine 8.06, Na 131, and CO2 18. The complete blood count was within normal limits. Treatment was initiated in the ED, with aggressive fluid hydration with 5 L normal saline and vancomycin. The plan was made to transfer the patient to nearest tertiary care center; however, due to delay in transfer and shortage of beds at tertiary care center intensive care unit (ICU), decision was made to transfer after emergent decompressive fasciotomy at presenting hospital. Despite initial bolus of 5 L normal saline, the patient remained hypotensive (blood pressure 79/40) and required vasopressors and was started on intravenous clindamycin.
The patient was taken to the OR, where a four-compartment fasciotomy and incision and drainage of the foot were performed, for urgent decompression. During the operation, a medial incision was made along the arch of the foot, across the bullae. On opening, significant fluid was expressed from the area and a culture was obtained. Two 4 cm counter incisions were made on the dorsum of the foot, expressing additional fluid but no pus. A longitudinal incision was then made along the medial aspect of the foot extending along the length of the tibia. Dissection was taken down to the fascia. As the fascia was opened, the muscle belly bulged and was noted to be dark and gray. As edema was removed, the muscle belly became pink and reactive. The soleus muscle was then taken down to expose the posterior and medial compartments. Along the lateral aspect of the foot, an incision was made 2 cm distal and posterior to the fibular head. The dissection was taken down to the level of the fascia, and the muscle bellies appeared to be bulging and gray. As the fascia was opened, the muscles began to turn pink and edema was removed. The patient remained hypotensive despite administration of additional vasopressors. Each incision was packed with Kerlix packing and sterile dressing wrapped around his leg. The patient was taken to the ICU until transfer to a tertiary care facility. Cultures returned positive for Group A streptococcus.
DISCUSSION
Among necrotizing soft tissue infections, there are two types of NF [1]. Type 1 NF most commonly has a polymicrobial etiology often associated with aerobic and anaerobic microbes [1,2] Type 2 NF usually has a monomicrobial etiology with Group A streptococcus as the most common cause [1-3] Necrotizing soft tissue infections typically have a non-specific presentation and vary based on the extent of disease [4,5]. Initial presenting features may include erythema not sharply demarcated, edema, tenderness, skin lesions, blister formation, ulceration, necrosis, crepitus, pain out of proportion, and subcutaneous tissue induration [1,6]. Overlying tissue may appear unaffected despite underlying fascial infection [6] Surgical intervention is the only definitive modality to differentiate between NF, myositis, and pyomyositis [2] Although it may be difficult to diagnose NF without direct visualization of the infected soft tissue, it is imperative to begin management immediately to limit morbidity and mortality [4-9].
One indispensable tool to help predict the probability of a necrotizing soft tissue infection is the laboratory risk indicator for NF score [1,4,10]. This score takes into account six specific parameters; C-reactive protein, white blood cell count, hemoglobin, sodium, creatinine, and glucose, at the time of admission [1,4,10]. Patients are stratified in risk categories of low, medium, and high [3,8]. A score of 5 or less at the time of admission predicts a < 50% chance of developing NF [3,8]. Medium risk is predicted when the patient's score is between 6 and 7 and indicates a 50%-75% chance of developing NF [3,8]. Finally, patients are designated as high risk with a score of 8 or greater, interpreted as a > 75% chance of developing NF [1,4,8-10]. Other findings supporting the diagnosis of NF include radiographic imaging such as CT or magnetic resonance imaging showing soft tissue swelling, positive wound cultures, leukocytosis with marked left shift, coagulopathy, elevated creatinine kinase, lactate, and creatinine [4,8]. Early surgical intervention is crucial to reduce mortality in a patient with high clinical suspicion of necrotizing soft tissue infection [3-8].
CONCLUSION
The patient in discussion possibly contracted this infection from bacteria introduced through breaks in the skin as a result of scratching the bed bug bites he reported on presentation.
Due to the urgent course of the patient's hospital stay, no pictures were taken of his left leg on presentation. Improvement of the color of the muscle bellies, from gray to pink after the fasciotomy, supported the diagnosis of compartment syndrome as sequela of NF. Early detection of a possible necrotizing soft tissue infection and treatment of compartment syndrome proved to be lifesaving for this patient.
REFERENCES
- Shaikh N. Necrotizing fasciitis: A decade of surgical intensive care experience. Indian J Crit Care Med 2006;10:225-9.
- 2. Stevens DL, Baddour LM. Necrotizing soft tissue infections. In: Post T, editor. UpToDate. Waltham, MA.: UpToDate; 2017. Available from: http://www.uptodate.com. [Last accessed on 2017 Apr 24].
- 3. Ali SS, Lateef F. Laboratory risk indicators for acute necrotizing fasciitis in the emergency setting. J Acute Disease 2015;5:114-6.
- 4. Gregorio M, Villa A. The relevance of a fast and early diagnosis of necrotizing fasciitis in the emergency department: A case report. Italian J Med 2016;10:223-5.
- 5. Stead TS, Hedna VS. Necrotizing fasciitis presenting as an itchy thigh. Case Reports Emerg Med 2016;2016:6376301.
- 6. Mustafa M, Firdaus H, Elllzam EM, Sharifa AM, Fairrul K, Muniandy RK, et al. Necrotizing fasciitis: Current concepts, pathogens and management. IOSR J Dent Med Sci 2017;16:146-51.
- 7. Leitch HA, Palepu A, Fernandes CM. Necrotizing fasciitis secondary to group A streptococcus. Morbidity and mortality still high. Can Fam Physician 2000;46:1460-6.
- 8. Misiakos EP, Bagias G, Papadopoulos I, Danias N, Patapis P, Machairas N, et al. Early diagnosis and surgical treatment for necrotizing fasciitis: A Multicenter study. Front Surg 2017;4:5.
- 9. Johnson P, Ocksrider J, Silva SR. Update and review of acute compartment syndrome and necrotizing fasciitis. Intern Med Rev 2017;3:1-9.
- 10. Van Stigt SF, de Vries J, Bijker JB, Mollen RM, Hekma EJ, Lemson SM, et al. Review of 58 patients with necrotizing fasciitis in the Netherlands. World J Emerg Surg 2016;11:21.