Synchronous Endometrial Carcinoma and Adenosarcoma in Postmenopausal Patient: A Case Report
Chrisostomos. Sofoudis1, E. Tsanakalis1, M. Lenos2, G. Georgoulias1
2.Department of Surgical Pathology, Konstandopoulio General Hospital, Athens, Greece.
Citation :Sofoudis C, Tsanakalis E, Lenos M, Georgoulias G. Synchronous Endometrial Carcinoma and Adenosarcoma in Post-menopausal Patient: A Case Report. Clin J Surg 2018;1(1):1-3.
Adenosarcomas represent one of the rarest types of endometrial cancer (E.C). On the other hand, the incidence of E.C is increasing, especially in developed countries. E.C is the fourth most common type of cancer in women. The presence of two different histologic neoplasms inside the endometrial cavity on the same patient reflects an extremely rare occasion. Predispositional factors which influence the therapeutic strategy are the age of the patient, tumor size, lymphatic infiltration, staging, and grading of the lesion. Therapeutic mapping is strongly accompanied with quality of life, increased overall survival, and fertility preservation, especially in women of reproductive age. The aim of this study is focused on the presentation of a 64-year-old patient with synchronous E.C and adenosarcoma proper diagnosed and treated.
Adenosarcoma, endometrial cancer, lymph node dissection, obesity.
INTRODUCTION
Adenosarcomas are comprised by a malignant stromal sarcoma, as well as a benign epithelial component, making up approximately 8% of all uterine sarcomas [1]. They can be encountered in both pre- and post-menopausal women. Mean age of the patients has been reported between 50 and 55 years old [2].
Adenosarcomas are not only located on the body of the uterus but also on the cervix, the ovaries, and even the fallopian tubes. They most commonly appear as masses in the uterus, accompanied by uterine bleeding not linked to menstruation. Endometrial cancer's (E.C) incidence is on the rise and it is subdivided into two types. Type I is related to estrogen and includes adenocarcinomas. Type I is known for growing slowly and having a good prognosis since they infiltrate the myometrium only superficially. On the other hand, Type II is not related to estrogen and has a worse prognosis because of its aggressive behavior.
As it is easily understood, the risk factor highly linked to E.C is the amount of exposure to estrogen regardless if it internally produced or it is encountered in the outside world.
Combination of several factors such as obesity epidemic, along with aging population, and increased age of childbearing all contributed to that increase [3,4].
We present a rare case of a 64-year-old patient with coexistence of two different histologic type carcinomas inside the endometrial cavity.
CASE REPORT
A 64-year-old patient (gravida 1 and para 1) admitted to our department with episodes of postmenopausal bleeding. The patient had a cesarian section in the past and underwent also a dilation and curettage (D and C) due to removal of an endometrial polyp.
Pap smear tests and pelvic examination revealed no signs of malignancy. The patient had undergone appendectomy and tonsillectomy during her teenage years. Her atomic history revealed diabetes mellitus II, hypercholesterolemia, thyroiditis, and increased arterial blood pressure all under treatment with the appropriate medication.
After all the laboratory and imaging examinations and the continuing vaginal bleeding, the patient underwent a D and C procedure. The histologic report consisted of an adenosarcoma in the endometrial cavity probably originating from the isthmus, as well as an adenocarcinoma of the endometrium.
A computed tomography (CT) of the upper abdomen and a magnetic resonance imaging (MRI) of the lower abdomen were scheduled for the patient. The CT did not reveal any signs of malignancy.
On the other hand, the MRI presented a growth of the endometrium infiltrating more than 50% of the myometrium. Furthermore, neoplastic tissue was located in the inner cervix.
According to histologic review, the patient underwent a total abdominal hysterectomy, bilateral salpingo-oophorectomy, pelvic lymph nodes dissection from internal and external iliac region, as well as dissection of omentum. On macroscopic examination, a mass was found protruding from the body of the uterus. The patient had an uneventful recovery after the surgery.
The final histologic examination revealed the isthmus as the origin of the neoplasm, infiltrating not only the body of the uterus but also the inner cervix. 17 dissected lymph nodes and the omental region were all free of malignancy. Cytological review of the peritoneum washing did not reflect any malignant cells. Microscopically, the lesion appeared like adenosarcoma with a sarcomatous overgrowth [Figures 1 and 2].
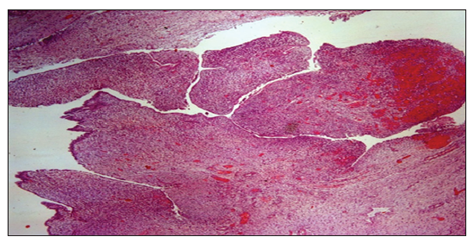
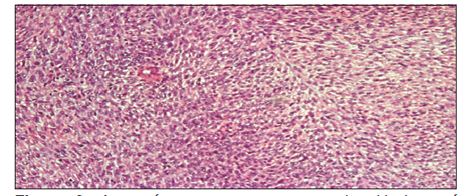
The neoplasm had a binary origin with epithelial and mesenchymal elements.
According to federation international of gynecology and obstetrics, the neoplasm was classified as pT1c N0 Mx.
The EC elements were classified as pT1 N0 Mx. There was any sign of these elements in the final histological review. They had been entirely removed during the D and C procedure.
The multidisciplinary council proposed CT thorax scan and upper abdomen followed by episodes of chemotherapy and radiotherapy.
These imaging findings did not reveal signs of metastatic lesion. The patient is followed up with laboratory and imaging examinations.
DISCUSSION
Early diagnosis of the uterine adenosarcoma is pivotal to the survival of the patient. The majority of cases are presented with a transvaginal ultrasound followed by normal imaging findings [5].
Definite diagnosis is only placed after microscopic analysis of the surgically removed uterus. Therapeutic mapping and treatment of choice are adjusted with a diagnostic hysteroscopy, along with a biopsy/resection of the lesion.
Lymph node dissection regarding the staging of EC cases is still a topic for discussion.
Sentinel lymph node or complete pelvic or para-aortic lymph node dissection had not been proven to lead to increase of overall survival and disease-free survival of the lesion [6,7].
As we mentioned before, age of the patient, tumor size, lymphatic infiltration, staging, and grading of the lesion affect the therapeutic strategy. In cases of premenopausal patients, less radical strategy and fertility preservation influence the final diagnosis.
It is a matter for discussion whether the use of post-operative radiotherapy offers increased survival rates [8,9].
According to current literature, 5% of cases of E.C consist premenopausal women of reproductive age [10-12].
Fertility-sparing treatment entails the use of oral progestins in high doses and/or the use of an intrauterine device releasing levonorgestrel.
Latest meta-analysis suggests that women using medroxyprogesterone acetate had regression up to 76.2% [13]. These cases are strongly accompanied with positive estrogen and progesterone receptors.
CONCLUSION
Coexistence of two different histologic neoplasms inside the endometrial cavity represents a rare entity. Proper diagnosis and treatment is related to increased free survival and overall survival of the lesion.
Multidisciplinary cooperation is mandatory to establish a definite clinical result.
REFERENCES
- Hollema M, De Vries W, Van Der Zee A. Adenosarcoma of the uterus following tamoxifen treatment for breast cancer pages. Int J Gynecol Cancer 1998;8:168-71.
- Gallardo A, Prat J. Mullerian adenosarcoma: A clinicopathologic and immunohistochemical study of 55 cases challenging the existence of adenofibroma. Am J Surg Pathol 2009;33:278-88.
- Wartko P, Sherman ME, Yang HP, Felix AS, Brinton LA, Trabert B, et al. Recent changes in endometrial cancer trends among menopausal-age U.S. Women. Cancer Epidemiol 2013;37:374-7.
- Crosbie EJ, Zwahlen M, Kitchener HC, Egger M, Renehan AG. Body mass index, hormone replacement therapy, and endometrial cancer risk: A meta-analysis. Cancer Epidemiol Biomarkers Prev 2010;19:3119-30.
- Leung F, Terzibachian JJ, Aouar Z, Govyadovskiy A, Lassabe C. Uterine sarcomas: Clinical and histopathological aspects. Report on 15 cases. Gynecol Obstet Fertil 2008;36:628-35.
- ASTEC study group, Kitchener H, Swart AM, Qian Q, Amos C, Parmar MK, et al. Efficacy of systematic pelvic lymphadenectomy in endometrial cancer (MRC ASTEC trial): A randomised study. Lancet 2009;373:125-36.
- Benedetti Panici P, Basile S, Maneschi F, Alberto Lissoni A, Signorelli M, Scambia G, et al. Systematic pelvic lymphadenectomy vs. No lymphadenectomy in early-stage endometrial carcinoma: Randomized clinical trial. J Natl Cancer Inst 2008;100:1707-16.
- Creutzberg CL, van Putten WL, Koper PC, Lybeert ML, Jobsen JJ, Warlam-Rodenhuis CC, et al. Surgery and postoperative radiotherapy versus surgery alone for patients with stage-1 endometrial carcinoma: Multicentre randomised trial. PORTEC study group. Post-operative radiation therapy in endometrial carcinoma. Lancet 2000;355:1404-11.
- Keys HM, Roberts JA, Brunetto VL, Zaino RJ, Spirtos NM, Bloss JD, et al. A phase III trial of surgery with or without adjunctive external pelvic radiation therapy in intermediate risk endometrial adenocarcinoma: A Gynecologic oncology group study. Gynecol Oncol 2004;92:744-51.
- Morice P, Leary A, Creutzberg C, Abu-Rustum N, Darai E. Endometrial cancer. Lancet 2016;387:1094-108.
- Lee NK, Cheung MK, Shin JY, Husain A, Teng NN, Berek JS, et al. Prognostic factors for uterine cancer in reproductive-aged women. Obstet Gynecol 2007;109:655-62.
- Rodolakis A, Biliatis I, Morice P, Reed N, Mangler M, Kesic V, et al. European society of gynecological oncology task force for fertility preservation: Clinical recommendations for fertilitysparing management in young endometrial cancer patients. Int J Gynecol Cancer 2015;25:1258-65.
- Gallos ID, Yap J, Rajkhowa M, Luesley DM, Coomarasamy A, Gupta JK, et al. Regression, relapse, and live birth rates with fertility-sparing therapy for endometrial cancer and atypical complex endometrial hyperplasia: A systematic review and metaanalysis. Am J Obstet Gynecol 2012;207:266.e1-12.