Apoptosis Post Microwave Ablation of the Liver: Does it Change with Power?
Ahmed Alzaraa1, Fergus McKeagney1, Charalampos Seretis1, Kassim Zayyan1, Kevin West2, Bruno Morgan3
2.Departments of Histopathology, University Hospitals of Leicester, United Kingdom, Europe.
3.Departments of Radiology, University Hospitals of Leicester, United Kingdom, Europe.
Citation : Alzaraa A, McKeagney F, Seretis C, Zayyan K, West K, Morgan B. Apoptosis Post Microwave Ablation of the Liver: Does it Change with Power?. Clin J Surg 2018;1(1):1-6.
Apoptosis is a type of the delayed or indirect cellular responses that happen after microwave ablation. It helps eradicate the few cancer cells that might survive the applied heat during cancer ablation. The extent of its expression is yet to be defined.
We investigated whether the ablation power made any difference to the expression of apoptosis in the ablated and normal areas.
Ablations with 50W, 70W, and 90W powers were created in three ex vivo perfused porcine livers. Biopsies were collected from the lesions and were assessed with Hematoxylin-Eosin and immunohistochemistry (Caspase 3 and M30) looking for apoptosis in each zone (central necrotic zone [CNZ], transitional zone [TZ], and normal surrounding zone [NZ]). Statistical analysis was performed using ANOVA and t-test.
None of the CNZ showed expression of Caspase-3. In the TZ, there was significant difference between 50W and 90W (P = 0.009), but not between 50W and 70W (P = 0.8), or between 70W and 90W (P = 0.4). In the NZ, a highly significant difference was noted between 50W and 90W (P = 0.003), a significant difference between 50W and 70W (P = 0.01), but not between 70W and 90W (P = 0.06). For M30, no expression of M30 was noted in all necrotic zones. A significant difference was noted between 50W and 90W (P = 0.02). There were no significant differences between 50W and 70W (P = 0.4) or between 70W and 90W (P = 0.07).
Increasing power enhances apoptosis in the ablated areas. This response can be an adjunct for eradicating cancer cells that might escape the heat in the ablated zones.
Ablation, apoptosis, liver, microwave
INTRODUCTION
With an enduring focus on minimally invasive techniques in surgery, ablative therapies have been of significant clinical interest in recent years for their potential utility in the treatment of early stage tumors in situ. Such ablation modalities have included ethanol ablation, cryoablation, laser ablation, focused ultrasound (FUS), radiofrequency ablation (RFA) and more lately, and microwave ablation (MWA) [1]. Delivery of localized thermoablative therapy in the clinical setting is performed under image guidance, with usually US or CT based methods used to guide the deposition of energy at a site of specific therapeutic benefit, usually a tumour [2]. The supraphysiological temperature rise of the surrounding tissues derived from this energy deposition causes changes at a molecular, cellular, and macro-histological level, resulting initially in coagulative necrosis of tissues in the immediate vicinity of the ablative energy. Further afield, away from the center of ablation and adjacent to cell necrosis occurs a zone of transition between necrosis and intact cells, where a delayed and indirect apoptotic response of a variable degree arises. This apoptotic response is of further therapeutic benefit in the treatment of neoplastic cells and the prevention of tumor recurrence [3].
With MWA being the latest ablation modality explored, work has been done to further characterize and compare the physical properties of this technique with other ablation modalities. MWA occurs at characteristic frequencies falling between 300 MHz and 300 GHz, laying between radio wave and infrared on the electromagnetic spectrum. The delivery of thermal energy in MWA is based on the alternation of polar electric charge on water (H2O) molecules in the local tissues causing agitation of, and thereby friction between, these H2O molecules generating heat. The frequency with which the charge on H2O molecules alternate depends on the frequency of microwave energy used, but is of the order of 2-5 X 109 times per second [4].
On review of the literature to date by the authors, current in vivo and ex vivo work on MWA has focused on characterizing its tumor ablation potential and ability to cause cell necrosis with regard to different MWA variables. These have included the wavelength of microwave energy used, with studies comparing wavelengths of 915 MHz and 2.45 GHz, energy application time and power used in watts, with studies comparing powers of between 45W-60W and 60W-180W [5]. In this study, we wanted to find out if apoptosis correlated with the applied MWA power. To the best of our knowledge, no similar experiments have been published in the literature.
MATERIALS AND METHODS
Three white pigs weighing between 45 and 60 kg were humanely sacrificed in accordance with the Home Office regulations. The autologous blood was collected in a pre- heparinized nonpyogenic container with 5000 Units of Heparin. With a minimal warm ischemic time, the livers were retrieved and were perfused with 2 L of cold Soltran solution (Baxter Healthcare, Thetford, United Kingdom) through the portal vein (PV) and the hepatic artery (HA) and were then transported on ice from the abattoir to the laboratory.
The circuit was primed with the autologous heparinized blood. Cannulation of the PV, HA, bile duct, and supra- and infra-hepatic inferior vena cava (IVC) was carried out during the priming. 1 L of 0.9% normal saline solution (Baxter Healthcare, Thetford, United Kingdom) was perfused through the PV and HA to flush out the Soltran solution and remove air from the liver and the cannulae before the livers were connected to the extracorporeal circuit.
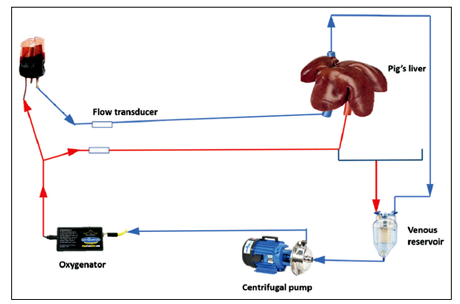
The extracorporeal circuit (Medtronic Inc., Minneapolis, Minnesota - United States) consisted of an automatic centrifugal pump which provided the HA flow and pressure, an oxygenator, a heat exchanger unit, and a blood reservoir to simulate the venous flow and pressure [Figure 1]. The venous blood was collected from the supra- and infra-hepatic IVC and returned to the centrifugal pump. Perfusion was carried out for 6 h. To optimize the physiological condition of the system, parenteral nutrition, vasodilation prostacyclins, sodium bicarbonate, sodium taurocholate, and insulin were added to the circulation.
In the three livers, 21 MWA lesions were created 1 h after liver perfusion to make sure all physiological parameters have settled. The lesions were created at powers 50W, 70W, and 90W (seven lesions for every power, total 21). Each lesion was created for 2 min. The microwaves were generated by a MicrosulisTissue Ablation Sulis TMV Generator (Microsulis Ltd., Denmead, Hampshire, UK) at a frequency 2.45 GHz and delivered through the Accu5i applicator (Microsulis Ltd., Denmead, Hampshire, UK) which has a shaft diameter of 9 mm and a biocompatible non-stick coating. The applicator was inserted to 2 cm beneath the surface of the liver in all applications to achieve a consistent shape throughout the study.
Wedge biopsies were collected from the ablated areas including the three zones and were embedded in liquid paraffin (seven biopsies for each power; 50W, 70W, and 90W, total = 21).
The specimens were cut onto Vectabond slides, dried at 37°C overnight and were then heated at 65°C for 10 min, deparaffinized through xylene, rehydrated through graded alcohols (99% industrial methylated spirits [IMS] and 95% IMS) and then rinsed in tap water for 5 min. The slides were then placed in a plastic slide rack, in a plastic dish which was then topped with 10 mM sodium citrate (pH 6.0). The dish was then microwaved at 80% power for 20 min and was then left to cool slowly in the buffer at room temperature.
Immunohistochemistry for apoptosis was conducted with the primary antibodies Cleaved Caspase-3 "Asp 175," New England Biolabs and M30 CytoDeath. Bioaxxess using the NovoLink Polymer Detection System and Leica Microsystems. RE7140-CE. The slides were washed with buffer (Blocking Solution - TBS/3%BSA/0.1% Triton-X-100) as a primary antibody diluent. Neutralization of the endogenous peroxidase was done by using Peroxidase Block for 5 min. The slides were then washed in TBS for 2 minX5 min, incubated with Protein Block for 5 min, washed in TBS for 2 minX5 min and were then incubated with optimally diluted primary antibody, then washed in TBS for 2 minX5 min, incubated with Post Primary Block for 30 min, washed again in TBS for 2 minX5 min and incubated with NovoLink Polymer for 30 min, washed in TBS for 2 minX5 min and developed peroxidase activity with DAB working solution for 5 min. The slides were then washed in tap water for 5 min and counterstaining with Mayer's Hematoxylin was done for 30 s. Finally, the slides were washed in tap water for 5 min and were then dehydrated and mounted in DPX. Apoptotic cells were identified when there was evidence of Caspase-3 and M30 positivity.
The apoptotic index was expressed as the ratio of the number of hepatic cells with Caspase-3 and M30 positivity out of the total number of nucleated cells in each field (magnification, X40) calculated after counting 5 random microscopic fields for each time point with a 19mm Whipple grid graticule lens (Pyser-SGI LTD). In each field, 100 squares were evaluated for the presence of apoptotic cells. Activated Caspase-3 hepatocytes positive for DNA fragmentation and cytoplasmic activity for M30 were counted on the whole sections. The mean counts were expressed as a percentage of the total number of non-apoptotic cells counted in each field.
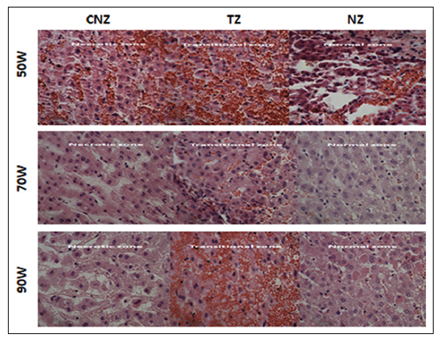
Signs of central coagulative necrosis with unrecognizable cell boundaries and collapsed collagen fibers were seen in the central necrotic zone (CNZ), surrounded by a transitional zone (TZ) with signs of vacuolation of hepatocytes, sinusoidal dilatation, and hemorrhagic extravasation of red blood cells from the sinusoids into the liver parenchyma [Figure 2].
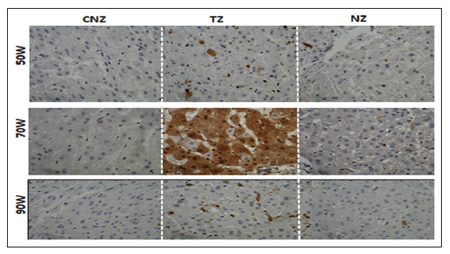
None of the samples showed any expression of Caspase-3 in the CNZ with all powers. There was strong evidence of its expression in all TZ, especially with power 70W, with less expression in the NZ [Figure 3].
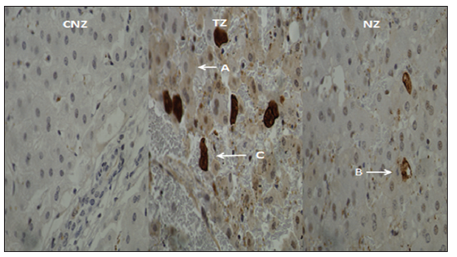
Different staining of M30 expression was noted in the TZ and NZs ranging from weak (a), intermediate (b) to strong (c) reactions. There was more expression in the TZ [Figure 4].
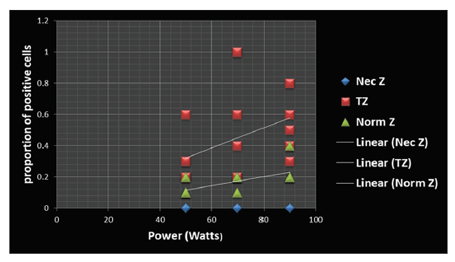
No expression of Caspase-3 was noted in all necrotic zones. In the TZ, the mean and SD values for 50W, 70W, and 90W were 0.28 "SD 0.14," 0.51 "SD 0.36," and 0.54 "SD 0.19," respectively. There was significant difference between Powers 50W and 90W (P = 0.009), but no significant differences between 50W and 70W (P = 0.8) or between 70W and 90W (P = 0.4) [Figure 5]. In the NZ, the mean and SD values were 0.11 "SD 0.03," 0.17 "SD 0.04," and 0.22 "SD 0.07," respectively. A highly significant difference was noted between 50W and 90W (P = 0.003), a significant difference between 50W and 70W (P = 0.01), but not between 70W and 90W (P = 0.06).
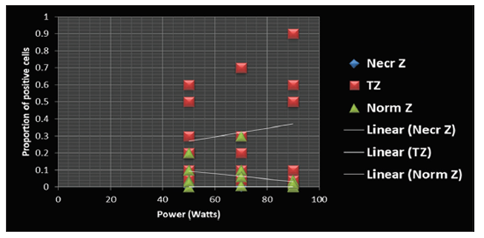
No evidence of M30 was noted in all necrotic zones. In the TZ, the mean and SD values for 50W, 70W, and 90W were 0.27 "SD 0.2," 0.29 "SD 0.29," and 0.38 "SD 0.33," respectively. The only significant difference was noted between powers 50W and 90W (P = 0.02). There were no significant differences between powers 50W and 70W (P = 0.4) or between 70W and 90W (P = 0.07). In the NZ, the mean and SD values were 0.08 "SD 0.06," 0.08 "SD 0.1," and 0.02 "SD 0.01," respectively [Figure 6].
DISCUSSION
Multiple focal ablative methods have been developed and investigated for alternative treatments that complement conventional oncologic therapies for primary and metastatic hepatic malignancies. These newer ablative techniques include MWA, high-intensity FUS, laser-induced interstitial thermotherapy, RFA, and cryoablation [6]. With all forms of thermal ablation therapies there are three distinct zones in heat-ablated lesions: The CNZ, which is in the immediately vicinity of the application rod and which undergoes ablation- induced coagulative necrosis; a TZ of sublethal hyperthermic injury, which mostly occurs from thermal conduction of the central area that is either undergoing apoptosis or recovering from reversible injury; and the surrounding NZ tissue that is unaffected by ablation [7]. As well as having three distinct lesion zones in MWA, there are also three factors that determine the extent of cellular damage caused by the heat- based ablative therapy: The amount of the applied energy, the rate of energy delivery and the target tissue's intrinsic thermal sensitivity [8]. Previous studies suggest that due to increased cellular density, fewer interstitial vascular and lymphatic channels to dissipate heat and the hypoxic/acidic tumor microenvironment, tumor tissue is more sensitive than normal tissue [9-13]. The focus of our study was to investigate whether the rate of MWA induced apoptosis in the CNZ, TZ, and NZ increased when three different ablative powers were applied. In our three controlled experiments, we applied 50W, 70W, and 90W MWA energies directly into the porcine hepatic lesions from which we took seven biopsies each and observed cell apoptosis using M30 and Caspase-3 as immunohistochemistry markers 6 h post ablation.
Previous MWA studies investigating the rate of apoptosis in liver cells have been published.A study by Ohno et al. measured the rate of apoptosis by Caspase-3 activity with flow cytometry in the transition zone immediately, 2, 6, 12, 24,72, and 168 h following MWA. Their study reported peak activity at 2-6 h with no evidence of CNZ apoptosis [14]. Another study by Bhardwaj et al. also confirmed the lack of apoptotic activity in the CNZ tissue post-MWA and their study demonstrated peak Caspase-3 expression in the transition zone at 4 h. Bhardwaj et al. hypothesized that the lack of apoptotic activity in the transition zone at time 0 was most likely due to the fact that very little energy had dissipated outside the immediate applicator and central zone and that in addition to other factors such as edema and local hemorrhage, and transition zone cells undergoing apoptosis post-ablation may also account for the increase in macroscopic ablation size observed at 4 and 24 h [4].
In our study, we too were able to confirm these findings as there was no evidence of apoptosis in the CNZ at all applied powers using Caspase-3 and M30 as apoptotic markers 6 h post-MWA. However, unlike previous studies, our study was able to demonstrate that there was a noticeable change in the rate of apoptosis within the TZ and NZ when the applied MWA power was increased. When we compared apoptosis at the TZ and NZ using Caspase-3 as a marker, we observed that there was a marked increase in apoptosis induction between 50W and 90W. We were also able to observe a higher peak rate of apoptosis in the TZ at 70W compared to 90W and increased apoptosis induction in the NZ at 90W compared to 50W and 70W. When we compared our biopsy samples with the different MWA ablative powers using the M30 maker, we also observed a marked increase in apoptosis induction at 90W compared to 50W in the TZ. There were less significant increases of apoptosis at 50W-70W and 70W-90W with the peak induction of apoptosis observed at 90W in the TZ.
A common limitation shared by all ablative heat-based modalities is the dissipation of thermal energy from the ablation zone to the peripheral zone or TZ known as the heat sink effect [15]. This effect primarily affects treatment efficacy within the TZ due to increased tumor tissues vasculature. Blood flowing within an adjacent blood vessel of highly vascular tumor tissue may prevent the peripheral zones reaching cytotoxic temperatures. This effect has been observed in the clinical setting, with higher rates of recurrence in tumors adjacent to large blood vessels [16]. In this study, we have been able to demonstrate that by increasing the MWA power, it is potentially possible to overcome the heat sink effect by induce a larger amount of apoptosis in the TZ and NZ of liver tissue. However, it must be noted that the size of the ablation zone with MWA can be harder to predict than other ablative modalities such as RFA and by increasing the power of MWA to escape the heat sink effect could potentially lead to overtreatment and damage to the adjacent off-target [16]. Further study needs to be carried out to access the possible advantageous or disadvantageous nature of these outcomes.
To calculate the extent of MWAinduced apoptosis in our study, we used the apoptotic index. Numerous sources of literature have pointed out that there are technical and methodological factors that can influence the determination of the apoptotic index and our study is no acceptation to this [17]. There is also no consensus on the criteria of how to define and calculate the apoptotic index. Some authors use it to denote the number of apoptotic cells per 1000 tumor cells, and other studies have defined it as a percentage of apoptotic cells and bodies per all tumor cells [18,19]. We calculated the apoptosis index as the ratio of all immunohistochemically Caspase-3 and M30 stained apoptotic cells out of the total number of nucleated cells in 500 high power microscopic fields.
It is now a general consensus that evasion of apoptosis is a hallmark of true established cancers [20]. However, some studies have discovered that inhibition of cell death is actually protective against HCC development in the liver. A study by Nakamoto et al. demonstrated in a preclinical model that anti- apoptotic treatment was preventative in the development of HCC in an animal model with HBV-mediated liver cancer [21]. Another study by Pierce et al. demonstrated that transgenic expression of Bcl-2 also prevented HCC in a mouse model of HCC [22]. However, other studies that examined increased induction of hepatocyte apoptosis with its associated compensatory cellular proliferation and inflammation found that this process was actually carcinogenic in the liver. For example, Vick et al [23]. demonstrated that in knockout Mcl-1 mice models there was hepatocyte genetic deletion of the potent antiapoptotic Bcl-2 protein leading to spontaneous hepatocyte apoptosis, cell turnover, inflammation, and hepatocarcinogenesis.
As our results have illustrated, with increasing MWA power, there is an increase in apoptosis before a threshold is hit. The next key question to ask is; is there a balance between applying an optimum MWA power that induces a high rate of apoptosis and can be used as an adjunct with other therapies to treat malignancy, or does the increase of apoptosis enhance the rate of malignancy and protect the malignant cells to develop and cause treatment resistance? There have been numerous studies that have investigated the role of apoptosis in HCC and other hepatic malignancies with inconclusive and conflicting results [21-23]. We would recommend further studies to establish if an increase of apoptosis through ablation therapies is beneficial or detrimental to the treatment of HCC and metastatic malignancies.
As the created lesions in our model were benign, it is not an ideal replication for human hepatic cancers. All tissue samples were taken 6 h post-MWA, and no follow-up biopsies were taken later. Therefore, there was no review to observe the evolution of apoptosis in the TZ and NZ with the increasing ablative powers. Another limitation was that the duration of ablation was kept the same for all power settings. To obtain the same ablation diameter, the low power settings should have been kept for longer to reflect real-life scenario.
CONCLUSION
For the 1st time, we were able to demonstrate the effect of different MWA powers on the rate of apoptosis induction in CNZ, TZ, and NZ of ablative tissue. Increasing MWA power enhances apoptosis in the peripheral ablated areas. This response has the potential to be an adjunct for eradicating cancer cells that might escape the heat in the peripheral ablated zones. Further study is needed to investigate if increasing the ablative power and induction of apoptosis has a long-term positive or negative effect on the outcome of treatment for hepatic malignancies.
REFERENCES
- Gravante G, Ong SL, Metcalfe MS, Strickland A, Dennison AR, Lloyd DM, et al. Hepatic microwave ablation: A review of the histological changes following thermal damage. Liver Int 2008;28:911-21.
- Hyodoh H, Furuse M, Kawamoto C, Isoda N, Ido K, Saito K, et al. Microwave coagulation therapy: Ex vivo comparison of MR imaging and histopathology. J Magn Reson Imaging 2000;11:168-73.
- Alzaraa A, Gravante G, Chung WY, Al-Leswas D, Morgan B, Dennison A, et al. Contrast-enhanced ultrasound in the preoperative, intraoperative and postoperative assessment of liver lesions. Hepatol Res 2013;43:809-19.
- Bhardwaj N, Dormer J, Ahmad F, Strickland AD, Gravante G, West K, et al. Microwave ablation of the liver: A description of lesion evolution over time and an investigation of the heat sink effect. Pathology 2011;43:725-31.
- Wei Z, Ye X, Yang X, Zheng A, Huang G, Li W, et al. Microwave ablation in combination with chemotherapy for the treatment of advanced non-small cell lung cancer. Cardiovasc Intervent Radiol 2015;38:135-42.
- Lee EW, Chen C, Prieto VE, Dry SM, Loh CT, Kee ST, et al. Advanced hepatic ablation technique for creating complete cell death: Irreversible electroporation. Radiology 2010;255:426-33.
- Chu KF, Dupuy DE. Thermal ablation of tumours: Biological mechanisms and advances in therapy. Nat Rev Cancer 2014;14:199-208.
- Paulet E, Aube C, Pessaux P, Lebigot J, Lhermitte E, Oberti F, et al. Factors limiting complete tumor ablation by radiofrequency ablation. Cardiovasc Intervent Radiol 2008;31:107-15.
- Kwan KG, Matsumoto ED. Radiofrequency ablation and cryoablation of renal tumours. Curr Oncol 2007;14:34-8.
- Haen SP, Pereira PL, Salih HR, Rammensee HG, Gouttefangeas C. More than just tumor destruction: Immunomodulation by thermal ablation of cancer. Clin Dev Immunol 2011;2011:160250.
- Davalos RV, Mir IL, Rubinsky B. Tissue ablation with irreversible electroporation. Ann Biomed Eng 2005;33:223-31.
- Sanchez-Ortiz RF, Tannir N, Ahrar K, Wood CG. Spontaneous regression of pulmonary metastases from renal cell carcinoma after radio frequency ablation of primary tumor: An in situ tumor vaccine? J Urol 2003;170:178-9.
- Mehta A, Oklu R, Sheth RA. Thermal ablative therapies and immune checkpoint modulation: Can locoregional approaches effect a systemic response? Gastroenterol Res Pract 2016;2016:9251375.
- Ohno T, Kawano K, Sasaki A, Aramaki M, Yoshida T, Kitano S, et al. Expansion of an ablated site and induction of apoptosis after microwave coagulation therapy in rat liver. J Hepatobiliary Pancreat Surg 2001;8:360-6.
- Lu DS, Raman SS, Vodopich DJ, Wang M, Sayre J, Lassman C, et al. Effect of vessel size on creation of hepatic radiofrequency lesions in pigs: Assessment of the "heat sink: effect. AJR Am J Roentgenol 2002;178:47-51.
- Lu DS, Raman SS, Limanond P, Aziz D, Economou J, Busuttil R, et al. Influence of large peritumoral vessels on outcome of radiofrequency ablation of liver tumors. J Vasc Interv Radiol 2003;14:1267-74.
- Potten CS. What is an apoptotic index measuring? A commentary. Br J Cancer 1996;74:1743-8.
- Soini Y, Paakko P, Lehto VP. Histopathological evaluation of apoptosis in cancer. Am J Pathol 1998;153:1041-53.
- Shinohara T, Ohshima K, Murayama H, Kikuchi M, Yamashita Y, Shirakusa T, et al. Apoptosis and proliferation in gastric carcinoma: The association with histological type. Histopathology 1996;29:123-9.
- Hanahan D, Weinberg RA. Hallmarks of cancer: The next generation. Cell 2011;144:646-74.
- Nakamoto Y, Kaneko S, Fan H, Momoi T, Tsutsui H, Nakanishi K, et al. Prevention of hepatocellular carcinoma development associated with chronic hepatitis by anti-fas ligand antibody therapy. J Exp Med 2002;196:1105-11.
- Pierce RH, Vail ME, Ralph L, Campbell JS, Fausto N. Bcl-2 expression inhibits liver carcinogenesis and delays the development of proliferating foci. Am J Pathol 2002;160:1555-60.
- Vick B, Weber A, Urbanik T, Maass T, Teufel A, Krammer PH, et al. Knockout of myeloid cell leukemia-1 induces liver damage and increases apoptosis susceptibility of murine hepatocytes. Hepatology 2009;49:627-36.