Non-operative Treatment Compared to Surgery in the Management of Uncomplicated Acute Appendicitis
Ashraf M. Abdelkader1, Taher H. Elwan1, Mokhtar A. Bahbah1, Emad M. Abdelrahman1, Nasser A. Zaher1, Ebtesam ND. Attia1
Citation : Abdelkader AM, Elwan TH, Bahbah MA, Abdelrahman EM, Zaher NA, Attia END. Non-operative Treatment Compared to Surgery in the Management of Uncomplicated Acute Appendicitis. Clin J Surg 2018;1(2):1-7.
Methods: The study includes 400 consecutive patients who were diagnosed as AA. The study involved patients with symptoms < 72 h and the first attack of AA. Patients divided into two equal groups using the "alternation" method. In the first group, patients were hospitalized and received medical treatment, while in the second group, appendectomy was done. After discharge, follow-up was done in all cases for 2 years. Data collected and statistically analyzed.
The NOT was effectively completed in 185 patients, while 15 patients (7.5%), did not respond to the NOT regimen as they had continued or deteriorating symptoms and underwent an appendectomy. During the follow-up period, 14 patients (7%) of the NOT group were readmitted and treated successfully, while 17 patients (8.5%) underwent an appendectomy. The success rate of the NOT was 84% with safety of 100%. Among patients of the surgery group, 160/200 showed a pathologically inflamed appendix with an efficacy of 80%.
In selected cases, AA can be managed by NOT taking into consideration patient assurance, proper observation, communication, and follow up.
Acute appendicitis, appendectomy, non-operative treatment, Surgery,asclepius open
INTRODUCTION
Acute appendicitis (AA) considered as one of the most common lower abdominal emergencies with an incidence of 89/100,000 annually,[1] and a lifetime prevalence of about 7-8%[2]. Presentation, clinical assessment, and pathological conditions of AA vary from one patient to another. About 20% of patients with AA are presenting with complications such as abscesses, gangrene, or peritonitis. However, the mainstream of cases is presented in an uncomplicated state[2]. Till now, appendectomy is the gold-standard choice for treating AA[3]. However, in several studies over the past decade, there has been an increasing interest toward the conservative management of this common condition[4-6]. These literature concentrated mainly on the safety, efficiency, therapeutic suitability, and economic competence of the medical treatment as compared to surgery in the management of AA[3,7].
Conservative management of AA was pronounced by Stengel in 1908 before the presence of antibiotics[8] and by Coldrey in 1956; however, it is not documented at this time due to lack of diagnostic modalities and antibiotic deficiency[9]. This line of management showed an upsurge manner over the past decade,[5] without a noticeable increase in the rate of appendix perforation[5]. This has led to a revised physiological as well as the pathologic condition of AA, which defines how perforated and non-perforated AA might represent two separate things[10]. Since many questions still not explained about the conservative management of AA, our target of the current study is to compare the outcomes of conservative therapy and surgical treatment for patients with uncomplicated acute appendicitis (UAA).
MATERIALS AND METHODS
The present prospective study was conducted in the General Surgery Department, at Banha University Hospital in Egypt and King Saud Hospital in Saudi Arabia from November 2015 to November 2018. The study includes 400 consecutive patients who are diagnosed as uncomplicated AA, after approval of the study protocol by the ethical committee. Patients were informed in detail about the possible risks and advantages of the two procedures (non-operative treatment [NOT] vs. appendectomy). A separate fully informed written consent was signed for surgical operation.
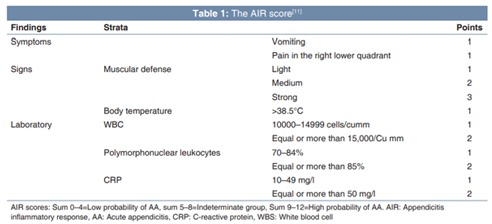
Before hospitalization, patients were evaluated through clinical, laboratory, and radiological exams. History of pain, nausea and/or vomiting, fever, constipation or diarrhea was undertaken. Clinical data included right iliac fossa tenderness, rebound tenderness, and special clinical signs were determined. Laboratory exams were done by means of complete blood count (CBC) and white blood cell (WBC) differential. Diagnostic imaging was done in the form of abdominal ultrasonography (US). In case the US is inconclusive, computed tomography (CT) scan was done. Calculation of the appendicitis inflammatory response (AIR) score, which is a system for the diagnosis of AA. The AIR score is made of 2-symptoms, 1-sign, and 4-laboratory results that were scored as shown in Table 1[11].
Inclusion criteria for the present study included: A - Clinical criteria: Right iliac fossa region localized tenderness, positive bowel sounds, no palpable abdominal masses, age =18 years and < 70 years, the patient's ability to sign consent and undergo the study procedure, and American Society of Anesthesiology (ASA) score of I-III. B - biochemical
criteria: Raised count of WBCs and high C-reactive protein (CRP). C - US criteria: Imaging-confirmed UAA such as a non-compressible appendix with an outer diameter >6mm that is tender on probing, secondary signs of inflammation such as infiltration of the surrounding fat, and increased vascularity within the wall of the appendix on Doppler US study. Exclusion criteria included: A - Clinical criteria: Signs of generalized peritonitis, symptoms long-lasting > 36 h, pregnant ladies, patients who were hospitalized before and treated conservatively for AA, suspicion of an underlying malignancy or inflammatory bowel disease, recognized allergy to the antibiotics used, patient sharing in another study, ASA score >III and psychiatric disease. B - Radiological criteria: Findings suggestive of complex appendicitis on imaging such as marked and/or turbid free fluid, signs of intraabdominal mass or abscess, signs of perforation, and a doubt of an appendiceal faecolith.
Patients divided into two groups (200 patients in each group) according to the type of AA management as NOT (medical) group and surgery group. In the present study, we have been using the "alternation" method as an allocation process that is not subject to anyone's personal decision. In this distribution method, we did the conservative management for the first patient who included in the study, then the surgical management for the second patient, then the conservative management of the third patient, and so on. Diagnosis of AA was completed through using the AIR score and abdominal US. Computed tomography (CT) was done in selected cases. In the group of patients who underwent surgery, AA was diagnosed pathologically when there is neutrophilic infiltration of the muscularis propria[12]. The collected data included: (1) Patients' demographics; gender, age, ASA score, clinical signs and symptoms, CBC, CRP, US, and AIR score at presentation and associated comorbidities and (2) the length of hospital stay and pathology results. The primary endpoint included the hospital stay days. Data collected at each participating hospital, then compared and analyzed.
The primary outcome of our study was the efficacy and the success rate of the NOT for UAA, that was defined as no appendectomy during hospital admission or within the follow-up period. The safety of the NOT protocol was defined as the absence of appendiceal perforation in the removed specimen in patients who underwent an appendectomy. Non-responders were defined as patients who did not respond to the NOT and underwent surgery during the initial hospital admission. Patients who underwent NOT but had a recurrent attack of AA during the follow-up period were considered as recurrent AA cases. On the other hand, the efficacy of surgical management was defined as AA that was confirmed by the PO pathological reports.
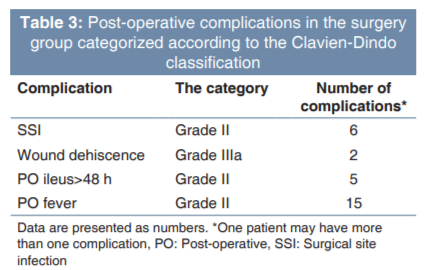
With regard to failure within the NOT group, all patients who needed surgery during the initial admission considered as (acute failure), while patients who were readmitted with a new episode of suspected AA and underwent an appendectomy within 1 year of follow-up considered as delayed failure. The failure rate in the surgery (appendectomy) group was evaluated using two outcome variables ("Failure 1" and "Failure 2"). Negative appendectomy was considered as "Failure 1," while peri - and post-operative (PO) complications (PO ileus >48 h, wound dehiscence, surgical site infection, or medical morbidities) were considered as "Failure 2" and categorized as mentioned in Clavien-Dindo classification[13].
Patients kept fasting during the first 12h and intravenous (IV) fluid given. Patients received one of the following IV antibiotics: (A) Ceftriaxone IV (1 g) once daily plus metronidazole IV infusion (IVI) (500 mg) 3 times daily or (B) ciprofloxacin IVI (200 mg) twice per day plus metronidazole IVI (500 mg) 3 times daily for 48h. Pain medication adjusted according to the pain scores and hospital protocols. Vital parameters are assessed every 6h, including pain scores. A physician reevaluates the patient twice per day. After 48h, if the patient meets the predefined discharge criteria, he/she is discharged home. If not, the NOT continued with a maximum duration of 72h.
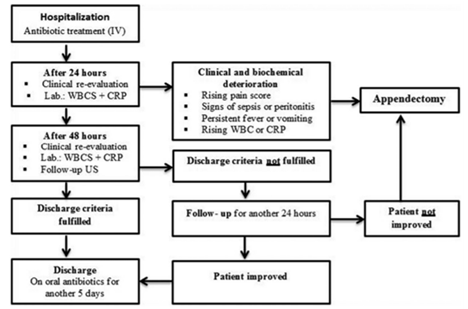
The discharge criteria for the NOT group are:
(1) Temperature < 38.0°C, (2) pain scores < 4, (3) reduced WBC count, (4) diminished CRP, (5) tolerate oral intake,
(6) Able to mobilize, and (7) 2nd US showed no signs of complex appendicitis. Patients were discharged with oral metronidazole (500 mg) 3 times per day plus amoxicillin/ clavulanic acid (1 g) 3 times a day. The total duration of antibiotic treatment is 7 days. Patients aged >40 years and allocated to the NOT group; a colonoscopy was indicated within the follow-up period.
More specifically, patients were allocated to the surgical group in the following situations: (1) If they preferred and underwent immediate surgical treatment from the start or
(2) if they underwent appendectomy within the first 72 h of NOT; this was based on sequential clinical evaluations of the on-call surgeon. However, patients who did not undergo surgery within 72 h belonged to the NOT group. Appendectomies were done either through conventional open approach or laparoscopic approach, depending on the patient's preference and the on-call surgeon's decision.
The data presented as mean ± standard deviation, numbers, ranges, and ratios. The results analyzed by means of Wilcoxon's ranked test. Statistical analysis implemented using the SPSS version 21 (IBM Corp., Armonk, NY, USA) for Windows statistical package. P-value was considered statistically significant if < 0.05.
RESULTS
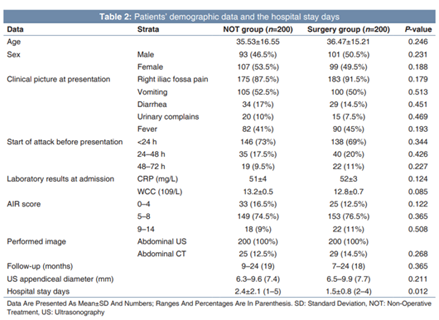
The study contained 400 consecutive patients who came to our emergency room suffering from acute abdominal pain and diagnosed as AA. Patients were divided into two equal groups; (1) the NOT group, underwent a NOT and (2) the surgery group, underwent appendectomy for AA. No difference regarding age, sex, and ASA score among patients of both groups. Medical history, clinical findings, AIR score, and pre-operative diameter of the appendix also were not statistically different in both groups (Table 2).
Cohort data of the study are described in Figure 2. The NOT protocol was effectively completed in 185 patients who were discharged home without operation. However, 15 patients (7.5%) did not respond to the NOT regimen, and they had a continuous or deteriorating abdominal pain or tenderness and underwent appendectomy within 3 days of admission. Histology examination revealed two gangrenous un-perforated appendices; 10 with inflamed appendices, 2 with mild acute subsiding appendicitis with lymphoid hyperplasia, and 1 with appendicolith without inflammatory changes [Figure 2]. Overall, 31 patients (15.5% of the NOT group) were readmitted for recurrent AA during the follow-up period. 14 patients (7%) were admitted 1-12 months after discharge and were treated successfully with NOT for the 2nd time after consent. However, the remaining 17 patients (8.5%) underwent an appendectomy. Histology of the 17 patients who were operated revealed no inflammation in 4 cases and AA in 13/17 patients, including 1/17 with gangrenous changes without perforation [Figure 2]. The overall success rate in the NOT group was 168/200 (84%) with a failure rate of 32/200 (16%) and safety of 100% as there were no any appendiceal perforations between cases who failed NOT and underwent surgery [Figure 2].
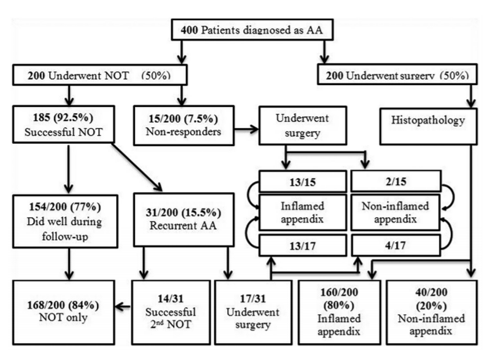
On the other hand, among the surgery group, 160/200 of operated patients showed a pathologically inflamed appendix with an efficacy of 80%. In the appendectomy group, "Failure 1" was 40/200 (20%) (Non-inflamed appendix depending on the PO pathological reports) and "Failure 2" encountered in 17/200 patients with a number of complications varied between Grade II and Grade IIIa according to the Clavien-Dindo classification (Table 3).
DISCUSSION
The diagnosis of AA remains vague, and surgeons benefit from radiological investigations to supplement the clinical picture before surgical intervention[14]. However, there are variable drawbacks of imaging, principally the exposure to radiation during CT scan in young people. On the other hand, there are probable several major complications associated with surgical operations in patients who are diagnosed as AA[15]. Hence, it is important to determine whether surgical intervention remains the management of first choice for treating persons who are diagnosed as having AA. A number of recent studies have suggested that AA can be managed with medical treatment. However, many recent studies concluded that the antibiotic use as a definitive treatment for AA is actually not simple and depends on numerous factors (e.g. Complicated versus UAA, adults vs. children, and if it is a final treatment or interval up to surgery)[16,17].
Our results reveal that there is an alternative management approach to UAA patients other than surgery. The patients with UAA can be advised that there is a safe option of NOT, and it is effective in most cases. Furthermore, they must be informed that the hospital stay will be longer for a mandatory close clinical observation and that is NOT might fail within 1-3 days in about 7-8% of cases, and an around 15-16% might need a second course of NOT. In general, about 18-20% will need surgical management for removal of the appendix during the follow-up period, without any extra morbidities or appendiceal perforation. Our experience in this study shows that, despite a potentially longer hospitalization, most patients preferred NOT through the initial hospital admission compared to the immediate operation for UAA.
The present study assessed the safety and feasibility of the NOT for uncomplicated AA, using predefined criteria. In our cohort of 400 patients with a diagnosed AA, 200 underwent NOT. Among these, 168 (84%) were managed without surgery and successfully completed the initial NOT with a median follow-up of 19 (9-24) months. In our study, there were no appendiceal perforations occurred in the group of patients who failed the NOT. This is consistent with the results of a recent meta-analysis[17] that included many studies about the safety and efficacy of NOT in cases of UAA, showed that NOT for UAA is effective, with success rate of 79% at final follow-up. This meta-analysis reported a 14% recurrence in AA throughout the follow-up period with no severe adverse events. This agrees with the results of our study in which 31/200 (15.5%) of the NOT group patients had a recurrent attack of AA during a median follow-up period of 19 (9-24) months. Among these group patients with recurrent AA, 11/200 (5.5%) had a successful 2nd NOT trial. On the other hand, among the surgery group of our study, 160/200 of operated patients showed a pathologically inflamed appendix with an efficacy of 80%. We think that our policy of giving IV antibiotics for 3 days and excluding cases of AA with appendicolith from the NOT group might be an important contributing factor in our high success rates. However, a short course of antibiotics might lead to unsuccessful treatment. The aforementioned meta-analysis conclusion was that the absence of major variances in outcomes between NOT and appendectomy, and there was a balance between the results of both treatment modalities. However, the authors mentioned that no recommendation can be given until there are large-scale randomized studies comparing the NOT with appendectomy in the UAA.
On the dispute of the above-mentioned results and opinions, Kessler et al.[18] in their recent systematic review that evaluated the NOT and appendectomy for management of UAA in children in a five cohort and randomized studies[19] found that in general, there were a few post-appendectomy complications, with comparable numbers in NOT and appendectomy (2% in both procedures). However, when they had analyzed the efficacy of NOT versus appendectomy, they found that appendectomy had an 82.5% success rate and NOT had a success rate of 74% (less efficacious). In addition, the appendectomy was associated with lower readmission rates compared to NOT. Their conclusion was that the surgical treatment should still be considered the management of first choice for UAA in children. In spite of a higher success rate in the NOT group our study, we do not support giving up surgery for AA, as appendectomy can eliminate appendicitis forever. We argue that if we applied to a strict inclusion and exclusion criteria in selected patients with UAA, NOT can be efficacious and safe and patients prefer it very much. We think that our protocol of regular follow-up that extended in some cases up to 24 months with a mean duration of 19 months in the NOT group through fixed visits to the outpatient clinic, an available line for patients' communication in case of abdominal symptom recurrence, was essential to our study's success.
The pathology reports of the removed appendices of patients who failed NOT reveal the safety of the non-operative medical management of UAA. Between 17 removed appendices after recurrent AA, 1/17 was gangrenous, 12/17 were inflamed, and 4/17 had no inflammation. There was no case of the perforated appendix in our study group with safety of 100%. This result agrees with several recent studies which confirmed that a delay of surgery in UAA is safe and not associated with an increase in the rate of appendiceal perforation, as well as this does not rise the hazard for PO morbidities[12]. In our study, we included only patients with abdominal pain for < 3 days before presentation depending on the hypothesis that has been established by other studies and mentioned that long time of complaints leads to greater danger for complicated AA[20]. It's important to mention that our study, as well as in others, the NOT is not preferred when appendicolith is found[19,21]. The more likely explanation is that the appendicolith causes an irreversible obstruction in the lumen of the appendix, contrary to the lymphoid hyperplasia that causes a reversible obstruction[22].
Allievi et al.[12] in their study agree with us and concluded that the conservative treatment of AA seemed to be safe and effective, and they explained this by mentioning that, if we consider negative appendectomy as a failure, the NOT was associated with a lesser percentage of failures (16.5%), as compared to the appendectomy (28.4%). This goes with our results, in which the failure rate of NOT was 7.5%, while in the surgery group, the "failure 1" (negative appendectomy) was 20% and the "failure 2" (PO complications) was 28 events (14%). Furthermore, they agree with us and mentioned that the surgery group was showing a shorter length of hospital stay during the hospital admission. Although it is less cost-effective than surgery for patients with UAA,[23] NOT has several advantages. First of all, it avoids the trauma of surgery and exposure to general anesthesia. Furthermore, preserving the appendix may be beneficial in that it is a fine reservoir for bacteria that normally found in the bowel flora, and required to recolonize the gut after bacterial infections, for example, diarrheal disease[24,25].
CONCLUSIONS
At the end of our study, we can confirm that, with a strict diagnostic strategy and firm inclusion and exclusion criteria, NOT considered as feasible and safe procedure in the management of UAA with a success rate of 84%. Physicians should take into consideration that NOT does not compete with appendectomy or make surgery obsolete. It is a safe alternative procedure in selected and appropriate cases. Further studies should be undertaken in this field to define the best management strategy for AA.
References
- Ceresoli M, Zucchi A, Allievi N, Harbi A, Pisano M, Montori G, et al. Acute appendicitis: Epidemiology, treatment and outcomes- analysis of 16544 consecutive cases. World J Gastrointest Surg 2016;8:693-9.
- Livingston EH, Woodward WA, Sarosi GA, Haley RW. Disconnect between incidence of nonperforated and perforated appendicitis: Implications for pathophysiology and management. Ann Surg 2007;245:886-92.
- Wilms IM, de Hoog DE, de Visser DC, Janzing HM. Appendectomy versus antibiotic treatment for acute appendicitis. Cochrane Database Syst Rev 2011;11:CD008359.
- Salminen P, Paajanen H, Rautio T, Nordstrom P, Aarnio M, Rantanen T, et al. Antibiotic therapy vs appendectomy for treatment of uncomplicated acute appendicitis: The APPAC randomized clinical trial. JAMA 2015;313:2340-8.
- Varadhan K, Neal K, Lobo D. Safety and efficacy of antibiotics compared with appendicectomy for treatment of uncomplicated acute appendicitis: Meta-analysis of randomized controlled trials. BMJ 2012;344:e2156.
- Sallinen V, Akl EA, You JJ, Agarwal A, Shoucair S, Vandvik PO, et al. Meta-analysis of antibiotics versus appendicectomy for non-perforated acute appendicitis. Br J Surg 2016;103:656-67.
- Sartelli M, Viale P, Catena F, Ansaloni L, Moore E, Malangoni M, et al.2013 WSES guidelines for management of intra-abdominal infections. World J Emerg Surg 2013;8:3.
- Stengel A. Appendicitis. In: Osler W, McCrae T, editors. Modern Medicine. Vol. 5. Diseases of the alimentary tract. Philadelphia, PA: Lea & Febiger; 1908. World J Surg 2017;41:2697-705, 2704.
- Coldrey E. Treatment of acute appendicitis. Br Med J 1956;2:1458-61.
- Bhangu A, Soreide K, Di Saverio S, Assarsson J, Drake F. Acute appendicitis: Modern understanding of pathogenesis, diagnosis, and management. Lancet 2015;386:1278-87.
- Andersson M, Andersson RE. The appendicitis inflammatory response score: A tool for the diagnosis of acute appendicitis that outperforms the alvarado score. World J Surg 2008;32:1843-9.
- Allievi N, Harbi A, Ceresoli M, Montori G, Poiasina E, Coccolini F, et al. Acute appendicitis: Still a surgical disease? Results from a propensity
- Dindo D, Demartines N, Clavien PA. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 2004;240:205-13.
- Stahlfeld K, Hower J, Homitsky S, Madden J. Is acute appendicitis a surgical emergency? Am Surg 2007;73:626-9.
- O'Connell PR. The vermiform appendix. In: Williams NS, Bulstrode CJ, O'Connell PR, editors. Bailey and Love's Short Practice of Surgery. 25th ed. London: Hodder Arnold; 2008. p. 1204-18.
- Steiner Z, Buklan G, Stackievicz R, Gutermacher M, Litmanovitz I, Golani G, et al. Conservative treatment in uncomplicated acute appendicitis: Reassessment of practice safety. Eur J Pediatr 2017;176:521-7.
- Georgiou R, Eaton S, Stanton MP, Pierro A, Hall NJ. Efficacy and safety of nonoperative treatment for acute appendicitis: A meta-analysis. Pediatrics 2017;139:e20163003.
- Kessler U, Mosbahi S, Walker B, Hau EM, Cotton M, Peiry B, et al. Conservative treatment versus surgery for uncomplicated appendicitis in children: A systematic review and meta-analysis. Arch Dis Child 2017;102:1118-24.
- Gorter RR, The SM, Gorter-Stam MA, Eker HH, Bakx R, van der Lee JH, et al. Systematic review of nonoperative versus operative treatment of uncomplicated appendicitis. J Pediatr Surg 2017;52:1219-27.
- Oliak D, Yamini D, Udani V, Lewis R, Vargas H, Arnell T, et al. Can perforated appendicitis be diagnosed preoperatively based on admission factors? J Gastrointest Surg 2000;4:470-4.
- Broker ME, van Lieshout EM, van der Elst M, Stassen LP, Schepers T. Discriminating between simple and perforated appendicitis. J Surg Res 2012;176:79-83.
- Otake S, Suzuki N, Takahashi A, Toki F, Nishi A, Yamamoto H, et al. Histological analysis of appendices removed during interval appendectomy after conservative management of pediatric patients with acute appendicitis with an inflammatory mass or abscess. Surg Today 2014;44:1400-5.
- Wu JX, Sacks GD, Dawes AJ, DeUgarte D, Lee SL. The cost-effectiveness of nonoperative management versus laparoscopic appendectomy for the treatment of acute, uncomplicated appendicitis in children. J Pediatr Surg 2017;52:1135-40.
- Randal Bollinger R, Barbas AS, Bush EL, Lin SS, Parker W. Biofilms in the large bowel suggest an apparent function of the human vermiform appendix. J Theor Biol 2007;249:826-31.
- De Coppi P, Pozzobon M, Piccoli M, Gazzola MV, Boldrin L, Slanzi E, et al. Isolation of mesenchymal stem cells from human vermiform appendix. J Surg Res 2006;135:85-91.