Prevalence of Chronic Kidney disease in Patients with Metabolic Syndrome in Saudi Population
Khalid S. J. Aljabri1, Samia A. Bokhari1, Muneera A. Alshareef1, Patan M. Khan1, Hesham M. Abuelsaoud1, Mohammad M. Jalal1, Rania F. Safwat1, Rehab M. El Boraie1, Bandari K. Aljabri2
2.College of Medicine, Umm Al-Qura University, Makkah, Kingdom of Saudi Arabia.
Citation : Aljabri KSJ, Bokhari SA, Alshareef MA, Khan PM, Abuelsaoud HM, Jalal MM, Safwat RF, El Boraie RM, Aljabri BK. Prevalence of Chronic Kidney disease in Patients with Metabolic Syndrome in Saudi Population. Clin Res Diabetes Endocrinol 2018;1(2):1-7.
Chronic kidney disease (CKD) which is an increasingly important clinical and public health issue is associated with cardiovascular disease. Epidemiologic studies have also linked metabolic syndrome (MetS) with an increased risk of incident CKD. Therefore, the present study was designed retrospectively to find the prevalence and potential risk factors of CKD in patients with MetS in Saudi Arabia.
For the present study, 1959 participants with MetS whom are between the age 20 and 98 years were analyzed retrospectively. All patients were from the population of the Primary Health Centre at King Fahad Armed Forces Hospital, Jeddah, Saudi Arabia.
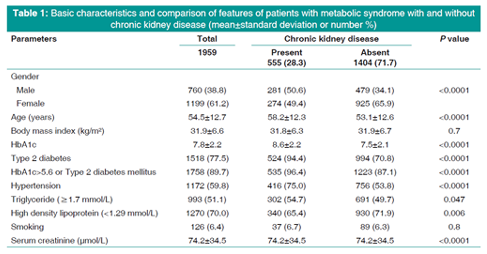
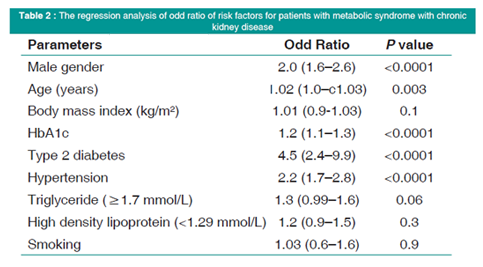
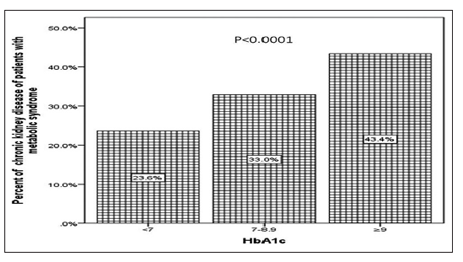
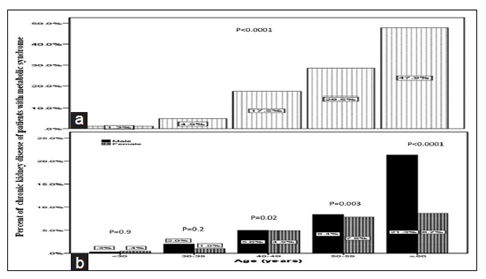
We analyzed 1959 participants with MetS. Mean age was 54.5 ± 12.7 (minimum 20 years and maximum 98 years). CKD was present in 555 (28.3%) cases. 281 (50.6%) cases were male and 479 (34.1%) cases were female with male to female ratio 1.5:1, P < 0.0001. Patients with CKD were significantly older than patients without CKD (58.2 ± 12.3 vs. 53.1 ± 12.6, respectively, P < 0.0001). Mean body mass index (BMI) was not significantly different in patients with than without CKD (31.8 ± 6.3 vs. 31.9 ± 6.7, respectively, P = 0.7). Mean HbA1c was significantly higher in patients with than without CKD (8.6 ± 2.2 vs. 7.5 ± 2.1, respectively, P < 0.0001). There was a graded linear relationship between HbA1c and the prevalence of CKD. Moreover, patients with CKD have a significantly higher prevalence of type 2 diabetes (T2DM), hypertension (HTN), and serum triglyceride (=1.7 mmol/L), and nonsignificantly slightly more frequent of smoking prevalence than patients without CKD. In addition, the number of MetS components and the risk for CKD showed a significant graded association. The multivariable logistic regression model examined the magnitude of associations between CKD presence in individuals with MetS and potential demographic and clinical factors. T2DM, hypertensive, or male patients with MetS were significantly 4-fold and 2-fold to possess CKD (odds ratio [OR] = 4.5; 95% confidence interval [CI] = 2.4, 9.9, P < 0.0001), (OR = 2.2; 95% CI = 1.7, 2.8, P < 0.0001), and (OR = 2.0; 95% CI = 1.6, 2.6, P < 0.0001), respectively. Age and HbA1c were associated with higher likely hood of CKD (OR = 1.02; 95% CI = 1.0, 1.03, P = 0.003) and (OR = 1.2; 95% CI = 1.1, 1.3, P < 0.0001), respectively. CKD prevalence is consistently statistically significant with increasing age (P < 0.0001) with male predominant across age groups; 40-49 years, 50-59 years, and =60 years. CKD prevalence is consistently statistically not significant with increasing BMI categories (P = 0.2) with significant male predominant across BMI groups.
It can be concluded from this study that the prevalence of CKD among MetS Saudis is relatively high. Older age, male gender, T2DM, HTN, and high HbA1c can be regarded as related factors. There is a graded relationship between the number of the MetS components and risk of CKD. These findings warrant future prospective and interventional studies to test the impact of preventing and treating the MetS on the risk of CKD.
Chronic kidney disease, metabolic syndrome, prevalence
INTRODUCTION
Worldwide, 10-15% of the population suffers from chronic kidney disease (CKD) [1,2]. CKD which is an increasingly important clinical and public health issue is associated with cardiovascular disease (CVD), and all-cause mortality [3,4]. The prevalence of CKD in Saudi population is around 5.1-5.7% [5,6]. Therefore, prevention and management of CKD by identifying and treating its risk factors are of critical urgency. Metabolic syndrome (MetS), which is characterized by high fasting glucose levels, high blood pressure, being overweight, abdominal obesity, hypertriglyceridemia, and low high- density lipoprotein cholesterol (HDL-C) levels, is prevalent worldwide, and its incidence is growing at an alarming rate annually [7]. Epidemiologic studies have also linked MetS with an increased risk of incident CKD [8,9]. The increase in the incidence of CKD has been paralleled with a rising prevalence of MetS in recent years. Obesity plays a particularly central role in the pathomechanisms of MetS and raises the risk for CKD by about 4-fold. The two chief risk factors for end- stage renal disease, hypertension (HTN), and Type 2 diabetes (T2DM) are both linked to MetS and obesity [10,11]. Previous studies have documented that MetS and CKD share similar risk factors, and both of them are also independent risk factors for CVD [12,13]. The MetS is also an important predictor of early renal dysfunction and the odds ratio (OR) of CKD and microalbuminuria increase with the number of MetS components [12,14]. Prospective data have demonstrated the impact of MetS on the evolution of CKD and highlighted the importance of targeting MetS for prevention of renal disease and premature death [15]. Therefore, the present study was designed retrospectively to find the prevalence and potential risk factors of CKD in patients with MetS in Saudi Arabia.
METHODS
For the present study, 1959 participants with MetS whom are between the age 20 and 98 years were analyzed retrospectively. All patients were from the population of the Primary Health Centre at King Fahad Armed Forces Hospital, Jeddah, Saudi Arabia. All data were collected on the basis of a review of electronic medical data and through a personal interview. All patients in the present study fulfilled the revised National Kidney Foundation criteria for the diagnosis of CKD [16]. The diagnosis and definition of CKD were made according to the presence of markers of kidney damage in urine or blood, or an eGFR < 60 mL/min/1.73 m2. All cases with other causes of CKD were excluded such as connective tissue diseases or chronic infection. Weight (kg) and height (cm) were measured and recorded. Body mass index (BMI) values classified into groups as lean (BMI < 18.5), normal weight (BMI = 18.5-24.9 kg/m2), overweight (BMI = 25.0-29.9 kg/m2), and obese (BMI =30 kg/m2) [17]. Laboratory assessments included HbA1c, lipids, creatinine, and urinary microalbumin. HbA1c was expressed as a percentage. High-performance liquid chromatography was used. Glycosylated hemoglobin was separated into three groups as < 7.0, 7.0-8.9, and =9.0. Fasting serum lipids were measured on a sample of blood after fasting for 14 h. We used the Enzymatic method for determining the cholesterol and triglycerides levels. Metabolic risk factors were defined using the 2006 IDF criteria that define elevated triglyceride as =150 mg/dL (=1.7 mmol/L) and reduced HDL-C as < 50 mg/dL (< 1.29 mmol/L) for female [18]. HTN was defined when the systolic blood pressure was =130 mm Hg and/or diastolic blood pressure was =85 mm Hg in addition to receiving any medication for HTN [19]. Abnormal glucose metabolism was considered when HbA1c (=5.7) or when patients were known to have T2DM [20]. A combination of two or more of these risk factors was used to define MetS. The total number of cohort was separated on the basis of age values into five groups: < 30 years, 30-39 years, 40-49 years, 50-59 years, and =60 years.
Unpaired t-test analysis and Chi-square test (categorical data comparison) were used between variables to estimate the significance of differences between groups for the demographic and clinical laboratory. The independent relationship between the stratified risk factors and the OR of having CKD was analyzed using logistic regression. All statistical analyses were performed using SPSS Version 23.0. The difference between groups was considered significant when P < 0.05.
RESULTS
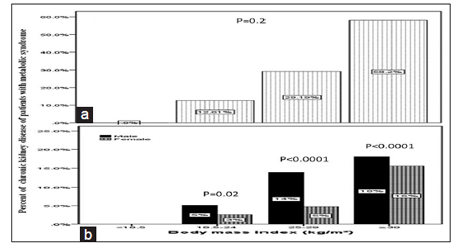
We analyzed 1959 participants with MetS. Mean age was 54.5 ± 12.7 (minimum 20 years and maximum 98 years), Table 1. CKD was present in 555 (28.3%) cases. 281 (50.6%) cases were male and 479 (34.1%) cases were female with male to female ratio 1.5:1, P < 0.0001. Patients with CKD were significantly older than patients without CKD (58.2 ± 12.3 vs. 53.1 ± 12.6, respectively, P < 0.0001). Mean BMI was not significantly different in patients with than without CKD (31.8 ± 6.3 vs. 31.9 ± 6.7 respectively, P = 0.7). Mean HbA1c was significantly higher in patients with than without CKD (8.6 ± 2.2 vs. 7.5 ± 2.1, respectively, P < 0.0001). There was a graded linear relationship between HbA1c and the prevalence of CKD, Figure 1. Moreover, patients with CKD have a significantly higher prevalence of T2DM, HTN, and triglyceride (=1.7 mmol/L) and nonsignificantly slightly more frequent of smoking prevalence than patients without CKD. In addition, the number of MetS components and the risk for CKD showed a significant graded association, Figure 2. The multivariable logistic regression model examined the magnitude of associations between CKD presence in individuals with MetS and potential demographic and clinical factors, Table 2. T2DM, hypertensive, or male patients with MetS were significantly 4-fold and 2-fold to possess CKD (OR = 4.5; 95% confidence interval (CI) = 2.4, 9.9, P < 0.0001), (OR = 2.2; 95% CI = 1.7, 2.8, P < 0.0001), and (OR = 2.0; 95% CI = 1.6, 2.6, P < 0.0001), respectively. Age and HbA1c were associated with higher likely hood of CKD (OR = 1.02; 95% CI = 1.0, 1.03, P = 0.003) and (OR = 1.2; 95% CI = 1.1, 1.3, P < 0.0001), respectively. CKD prevalence is consistently statistically significant with increasing age (P < 0.0001) with male predominant across age groups; 40-49 years, 50-59 years, and =60 years, Figure 3a and b. CKD prevalence is consistently statistically not significant with increasing BMI categories (P = 0.2) with significant male predominant across BMI groups, Figure 4a and b.
DISCUSSION
In our study, the overall prevalence of CKD in patients with MetS was 28.3%. MetS, previously called "syndrome X," is a term in popular use for the past quarter century, having first been described in 1988 by Reaven to denote a combination of selected, widely prevalent CVD related risk factors [7]. Many studies associate MetS with CKD [8,21-32]. MetS and CKD share a complex, bidirectional relationship. Data from the multiethnic study of atherosclerosis reported that the combination of CKD and MetS is a strong predictor of incident cardiovascular events (myocardial infarction, cardiac arrest, angina, stroke, and cardiovascular-related death) with an adjusted hazard ratio 5.56 (95% CI 3.72-8.12).
The prevalence of CKD increased sharply in participants after 60 years of age. Renal functions deteriorate in the aged population for various reasons. In addition, the duration of MetS might be longer in the older participants (≥60 years),and this might explain the higher prevalence of CKD in the older participants. Moreover, these participants might have had renal diseases, such as nephrosclerosis or ischemic kidney disease.
In Saudi Arabia, T2DM is the most common cause of CKD [33]. We showed a graded linear relationship between HbA1c and the prevalence of CKD, Figure 1. The results support the notion that hyperinsulinemia has a significant role in renal dysfunction, and therefore, it is important to recognize the risk of end-organ complications [34,35]. De Fronzo et al. were the first to demonstrate this by assessing tissue sensitivity to insulin with the euglycemic insulin clamp technique in patients with renal insufficiency [36]. Insulin resistance and subsequent hyperinsulinemia in addition to mild hyperglycemia may be accountable for the association between impaired fasting glucose level and CKD [37,38].
Another component of MetS is HTN. HTN alone is a known cause of CKD and proteinuria and is the second leading cause of ESRD [39]. It is associated with an approximately 2- to 3-fold increased risk of microalbuminuria which could be related to increased intraglomerular pressure and resultant injury to the epithelial lining leading to leakage of albumin [40,41]. In a study by Rashidi et al., for HTN eliminated the statistical association between MetS and renal disease. This study suggests that HTN is the key player in the MetS renal disease association [42].
In our study, the mean BMI was not significantly different in patients with CKD in MetS patients.
BMI was not an independent factor for the occurrence of CKD in our patients in discordance with other studies [43-45]. Most previous studies found higher BMI in patients with CKD in MetS patients [21-32,46]. This could be explained by glomerular hyperfiltration, which results in glomerular sclerosis [47]. Pro-inflammatory cytokines secreted by adipose tissue (interleukin-6 and tumor necrosis factor-alpha) and angiotensin II33 can also play an important role in the genesis of glomerulosclerosis [48,49].
Dyslipidemia is also an important risk factor for proteinuria and decline of renal function [50]. In a prospective study of 12,728 subjects, high triglyceride and low HDL-C levels predicted an increased risk of renal dysfunction [51]. These results remained unchanged, even after additional adjustment for incident T2DM and HTN [9]. Dyslipidemia is associated with glomerular capillary endothelial and mesangial cell as well as podocyte injury, which further leads to mesangial sclerosis [52,53]. The accumulation of lipoproteins in the glomerular mesangium can stimulate matrix production and glomerulosclerosis [54]. Although hypertriglyceridemia and low HDL-C levels have been previously associated with an increased risk for CKD, these factors are often overlooked in clinical practice [9,50,51]. Our results suggest that these could be potential targets for reducing the risk of CKD. Early detection of MetS or high triglyceride levels might be beneficial if accompanied by early intervention such as statins to lower triglyceride levels and suppress the pathways for renal injury.
Our findings revealed that each component of MetS was an independent predictor of CKD. We analyzed individual components to explore their differential effect in the presence of MetS, and thus, the risk estimates were interpreted in the context of MetS, Tables 1 and 2. In addition, the number of MetS components and the risk for CKD showed a graded association, Figure 2. Therefore, therapeutic strategies that targeted individual MetS components seem highly reasonable for preventing CKD.
Our study has several limitations. This study was a retrospective and not longitudinal, preventing determination of whether any risk factors were the cause or result of CKD. Furthermore, a single serum creatinine value was used to estimate kidney function which might lead to the misclassification of CKD. This random measurement error, due to day-to-day variation in serum creatinine levels in individuals, is likely to bias the association toward zero.
These findings have important clinical and public health implications because MetS and CKD are becoming common in the Saudi general population. The current study provides new and important information regarding the relationship between MetS and risk of CKD in a representative sample of the Saudi general adult population and suggests that prevention and treatment of the MetS should be an important priority for reducing the prevalence of CKD and its associated disease burden in Saudi Arabia.
It can be concluded from this study that the prevalence of CKD among MetS Saudis is relatively high. Older age, male gender, T2DM, HTN, and high HbA1c can be regarded as related factors. There is a graded relationship between the number of the MetS components and risk of CKD. These findings warrant future prospective and interventional studies to test the impact of preventing and treating the MetS on the risk of CKD.
ACKNOWLEDGMENTS
We are grateful to the staffs from the Primary Care Department and Diabetic Centre at King Fahad Armed Forces Hospital for their valuable contributions in data collection. The authors have no conflicts of interest to disclose.
REFERENCES
- Eckardt KU, Coresh J, Devuyst O, Johnson RJ, Kottgen A, Levey AS, et al. Evolving importance of kidney disease: From subspecialty to global health burden. Lancet 2013;382:158-69.
- GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: A systematic analysis for the global burden of disease study 2013. Lancet 2015;385:117-71.
- Levey AS, Atkins R, Coresh J, Cohen EP, Collins AJ, Eckardt KU, et al. Chronic kidney disease as a global public health problem: Approaches and initiatives-a position statement from kidney disease improving global outcomes. Kidney Int 2007;72:247-59.
- Glynn LG, Reddan D, Newell J, Hinde J, Buckley B, Murphy AW, et al. Chronic kidney disease and mortality and morbidity among patients with established cardiovascular disease: A West of Ireland community-based cohort study. Nephrol Dial Transplant 2007;22:2586-94.
- AlsuwaidaAO, Farag YM,Al SayyariAA, Mousa D,Alhejaili F, Al-Harbi A, et al. Epidemiology of chronic kidney disease in the kingdom of Saudi Arabia (SEEK-Saudi investigators)-a pilot study. Saudi J Kidney Dis Transpl 2010;21:1066-72.
- Aljabri KS, Bokhari SA, Alshareef MA, Khan PM, Elsaoud HM, Jalal MM, et al. Prevalence of chronic kidney disease and its risk factors in Saudi adults. J Med Pract Rev 2018;2:241-4.
- Reaven GM. Banting lecture 1988. Role of insulin resistance in human disease. Diabetes 1988;37:1595-607.
- Lucove J, Vupputuri S, Heiss G, North K, Russell M. Metabolic syndrome and the development of CKD in American Indians: The strong heart study. Am J Kidney Dis 2008;51:21-8.
- Ryu S, Chang Y, Woo HY, Lee KB, Kim SG, Kim DI, et al. Time-dependent association between metabolic syndrome and risk of CKD in Korean men without hypertension or diabetes. Am J Kidney Dis 2009;53:59-69.
- Lakka HM, Laaksonen DE, Lakka TA, Niskanen LK, Kumpusalo E, Tuomilehto J, et al. The metabolic syndrome and total and cardiovascular disease mortality in middle-aged men. JAMA 2002;288:2709-16.
- Hall JE, Crook ED, Jones DW, Wofford MR, Dubbert PM. Mechanisms of obesity-associated cardiovascular and renal disease. Am J Med Sci 2002;324:127-37.
- Chen J, Muntner P, Hamm LL, Jones DW, Batuman V, Fonseca V, et al. The metabolic syndrome and chronic kidney disease in U.S. adults. Ann Intern Med 2004;140:167-74.
- Chien KL, Hsu HC, Sung FC, Su TC, Chen MF, Lee YT, et al. Metabolic syndrome as a risk factor for coronary heart disease and stroke: An 11-year prospective cohort in Taiwan community. Atherosclerosis 2007;194:214-21.
- Navaneethan SD, Schold JD, Srinivas TR. Metabolic syndrome and mild to moderate chronic kidney disease among minorities. Semin Nephrol 2010;30:51-8.
- Agrawal V, Shah A, Rice C, Franklin BA, McCullough PA. Impact of treating the metabolic syndrome on chronic kidney disease. Nat Rev Nephrol 2009;5:520-8.
- Inker LA, Astor BC, Fox CH, Isakova T, Lash JP, Peralta CA, et al. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am J Kidney Dis 2014;63:713-35.
- Chen YM, Ho SC, Lam SS, Chan SS. Validity of body mass index and waist circumference in the classification of obesity as compared to percent body fat in Chinese middle-aged women. Int J Obes (Lond) 2006;30:918-25.
- Bee YT Jr., Haresh KK, Rajibans S. Prevalence of metabolic syndrome among Malaysians using the international diabetes federation, national cholesterol education program and modified world health organization definitions. Malays J Nutr 2008;14:65-77.
- Whelton PK, Carey RM, Aronow WS, Casey DE Jr., Collins KJ, Dennison Himmelfarb C, et al 2017 ACC/AHA/AAPA/ABC/ ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, Evaluation, and management of High blood pressurein Adults: Executive Summary: A Report of the American college of cardiology/American heart association task force on clinical practice guidelines. J Am Coll Cardiol 2018;71:2199-269.
- American Diabetes Association 2. Classification and diagnosis of diabetes: Standards of medical care in diabetes-2018. Diabetes Care 2018;41:S13-S27.
- Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: Diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med 1998;15:539-53.
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult treatment panel III) final report. Circulation 2002;106:3143-421.
- Grundy SM, Brewer HB Jr., Cleeman JI, Smith SC Jr., Lenfant C, American Heart Association. et al. Definition of metabolic syndrome: Report of the national heart, lung, and blood institute/American heart association conference on scientific issues related to definition. Circulation 2004;109:433-8.
- Alberti KG, Zimmet P, Shaw J. The metabolic syndrome-a new worldwide definition. Lancet 2005;366:1059-62.
- Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, et al. Harmonizing the metabolic syndrome: A joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; American heart association; world heart federation; international atherosclerosis society; and international association for the study of obesity. Circulation 2009;120:1640-5.
- Gami AS, Witt BJ, Howard DE, Erwin PJ, Gami LA, Somers VK, et al. Metabolic syndrome and risk of incident cardiovascular events and death: A systematic review and meta-analysis of longitudinal studies. J Am Coll Cardiol 2007;49:403-14.
- Wilson PW, D'Agostino RB, Parise H, Sullivan L, Meigs JB. Metabolic syndrome as a precursor of cardiovascular disease and Type 2 diabetes mellitus. Circulation 2005;112:3066-72.
- Ford ES. Risks for all-cause mortality, cardiovascular disease, and diabetes associated with the metabolic syndrome: A summary of the evidence. Diabetes Care 2005;28:1769-78.
- Resnick HE, Jones K, Ruotolo G, Jain AK, Henderson J, Lu W, et al. Insulin resistance, the metabolic syndrome, and risk of incident cardiovascular disease in non diabetic American Indians: The strong heart study. Diabetes Care 2003;26:861-7.
- Hamaguchi M, Kojima T, Takeda N, Nakagawa T, Taniguchi H, Fujii K, et al. The metabolic syndrome as a predictor of nonalcoholic fatty liver disease. Ann Intern Med 2005;143:722-8.
- Lin WY, Liu CS, Li TC, Lin T, Chen W, Chen CC, et al. In addition to insulin resistance and obesity, hyperuricemia is strongly associated with metabolic syndrome using different definitions in Chinese populations: A population-based study (Taichung community health study). Ann Rheum Dis 2008;67:432-3.
- Kitiyakara C, Yamwong S, Cheepudomwit S, Domrongkitchaiporn S, Unkurapinun N, Pakpeankitvatana V, et al. The metabolic syndrome and chronic kidney disease in a Southeast Asian cohort. Kidney Int 2007;71:693-700.
- Al Wakeel JS, Mitwalli AH, Al Mohaya S, Abu-Aisha H, Tarif N, Malik GH, et al. Morbidity and mortality in ESRD patients on dialysis. Saudi J Kidney Dis Transpl 2002;13:473-7.
- Kubo M, Kiyohara Y, Kato I, Iwamoto H, Nakayama K, Hirakata H, et al. Effect of hyperinsulinemia on renal function in a general Japanese population: The Hisayama study. Kidney Int 1999;55:2450-6.
- Diabetes Prevention Program Research Group. Reduction in the incidence of Type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 2002;346:393-403.
- DeFronzo RA, Alvestrand A, Smith D, Hendler R, Hendler E, Wahren J, et al. Insulin resistance in uremia. J Clin Invest 1981;67:563-8.
- Eckel RH, Alberti KG, Grundy SM, Zimmet PZ. The metabolic syndrome. Lancet 2010;375:181-3.
- Tabak AG, Jokela M, Akbaraly TN, Brunner EJ, Kivimaki M, Witte DR, et al. Trajectories of glycaemia, insulin sensitivity, and insulin secretion before diagnosis of Type 2 diabetes: An analysis from the whitehall II study. Lancet 2009;373:2215-21.
- Klag MJ, Whelton PK, Randall BL, Neaton JD, Brancati FL, Ford CE, et al. Blood pressure and end-stage renal disease in men. N Engl J Med 1996;334:13-8.
- Jiang X, Srinivasan SR, Radhakrishnamurthy B, Dalferes ER Jr., Bao W, Berenson GS, et al. Microalbuminuria in young adults related to blood pressure in a biracial (black-white) population. The Bogalusa heart study. Am J Hypertens 1994;7:794-800.
- Srinivasan SR, Myers L, Berenson GS. Risk variables of insulin resistance syndrome in African-American and Caucasian young adults with microalbuminuria: The Bogalusa heart study. Am J Hypertens 2000;13:1274-9.
- Rashidi A, Ghanbarian A, Azizi F. Are patients who have metabolic syndrome without diabetes at risk for developing chronic kidney disease? Evidence based on data from a large cohort screening population. Clin J Am Soc Nephrol 2007;2:976-83.
- Watanabe H, Obata H, Watanabe T, Sasaki S, Nagai K, Aizawa Y, et al. Metabolic syndrome and risk of development of chronic kidney disease: The Niigata preventive medicine study. Diabetes Metab Res Rev 2010;26:26-32.
- Palaniappan L, Carnethon M, Fortmann SP. Association between microalbuminuria and the metabolic syndrome: NHANES III. Am J Hypertens 2003;16:952-8.
- Alexander MP, Patel TV, Farag YM, Florez A, Rennke HG, Singh AK, et al. Kidney pathological changes in metabolic syndrome: A cross-sectional study. Am J Kidney Dis 2009;53:751-9.
- Kramer H, Luke A, Bidani A, Cao G, Cooper R, McGee D, et al. Obesity and prevalent and incident CKD: The hypertension detection and follow-up program. Am J Kidney Dis 2005;46:587-94.
- Buscemi S, Verga S, Batsis JA, Cottone S, Mattina A, Re A, et al. Intra-renal hemodynamics and carotid intima-media thickness in the metabolic syndrome. Diabetes Res Clin Pract 2009;86:177-85.
- Bhowmik D, Tiwari SC. Metabolic syndrome and chronic kidney disease. Indian J Nephrol 2008;18:1-4.
- Locatelli F, Pozzoni P, Del Vecchio L. Renal manifestations in the metabolic syndrome. J Am Soc Nephrol 2006;17:S81-5.
- Tozawa M, Iseki K, Iseki C, Oshiro S, Ikemiya Y, Takishita S, et al. Triglyceride, but not total cholesterol or low-density lipoprotein cholesterol levels, predict development of proteinuria. Kidney Int 2002;62:1743-9.
- Muntner P, Coresh J, Smith JC, Eckfeldt J, Klag MJ. Plasma lipids and risk of developing renal dysfunction: The atherosclerosis risk in communities study. Kidney Int 2000;58:293-301.
- Cases A, Coll E. Dyslipidemia and the progression of renal disease in chronic renal failure patients. Kidney Int Suppl 2005;99:S87-93.
- Joles JA, Kunter U, Janssen U, Kriz W, Rabelink TJ, Koomans HA, et al. Early mechanisms of renal injury in hypercholesterolemic or hypertriglyceridemic rats. J Am Soc Nephrol 2000;11:669-83.
- Gluba A, Rysz J, Banach M. Statins in patients with chronic kidney disease: Why, who and when? Expert Opin Pharmacother 2010;11:2665-74.