Long-term Observational Study on Albuminuria and the Passive Extension Angle of Metacarpophalangeal Joints in Patients with Type 2 Diabetes
Yuji Aoki
Citation : Aoki Y. Long-term Observational Study on Albuminuria and the Passive Extension Angle of Metacarpophalangeal Joints in Patients with Type 2 Diabetes. Clin Res Diabetes Endocrinol 2018;1(2):1-6.
Limited joint mobility (LJM) is often observed in diabetic patients and elderly people. Since our previous cross-sectional study indicated the association of LJM with diabetic nephropathy, a longitudinal study was performed.
A total of 71 patients with type 2 diabetes whose albuminuria, graded as normo- (< 30 mg/g creatinine, Grade 0), micro- (30-300, Grade 1), and macroalbuminuria (>300, Grade 3), and the passive extension angle of metacarpophalangeal (MP) joints to quantitatively assess LJM were measured again 10-12 years later in 2015 were studied.
The angle of MP joints was smaller in males than in females and correlated with age in males but not in females at baseline. At follow-up, hemoglobin A1c (HbA1c) level increased, albuminuria worsened, and the angle of MP joints decreased. Binary logistic regression analysis demonstrated that the decreasing of the angle (>10°) could be predicted by male gender, age, body mass index, and duration of diabetes at baseline in patients with relatively normal angles of MP joints and that the worsening of albuminuria (progression from Grade 0 or 1 to Grade 1 or 2) could be predicted by age and use of insulin at baseline and HbA1c level at follow-up.
Taken together with our previous report, it is inferred that the decreasing of the angle of MP joints is rather associated with arteriosclerosis than early diabetic nephropathy. It would be worth elucidating the relationship between LJM, diabetic nephropathy, and macrovascular disease, all of which are involved in advanced glycation end products.
Advanced glycation end products, diabetic nephropathy, limited joint mobility, type 2 diabetes
INTRODUCTION
Limited joint mobility (LJM) is often observed in diabetic patients and elderly people. The main pathologic mechanism of joint stiffness is considered to be the increase of collagen cross-linking, due to the non- enzymatic glycosylation of collagen with advanced glycation end product (AGE) formation [1]. AGEs produced by glycoxidation cause collagen-associated fluorescence, cross-linking, and stiffening, which are not necessarily the same products [2,3]. In addition, LJM is not well-defined because of the different subjects studied and the different methods used to assess it [1,4].
We previously demonstrated in a cross-sectional study using a quantitative method to assess LJM that stiffening of connective tissue measured by the passive extension angle of metacarpophalangeal (MP) joints was associated with diabetic nephropathy and oxidative stress in elderly diabetic patients [5]. Here, a longitudinal observational study was performed to investigate the changes in the angle of MP joints and early diabetic nephropathy in patients with type 2 diabetes.
SUBJECTS AND METHODS
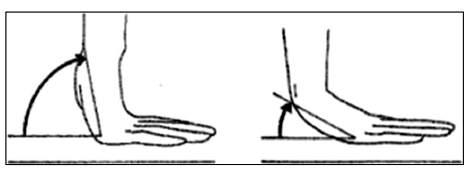
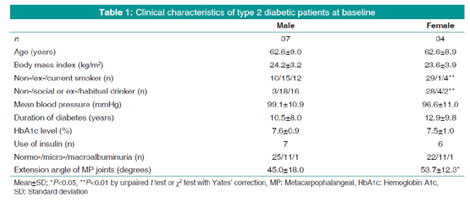
A total of 71 patients with type 2 diabetes whose albuminuria and the passive extension angle of MP joints were measured again 10-12 years later in 2015 were studied in accordance with the Declaration of Helsinki ethical guidelines. Their clinical characteristics and laboratory data at baseline are shown by gender in Table 1. Significant differences between male and female were seen in smoking and drinking status and the angle of MP joints. The measurement of the angle of MP joints to quantitatively assess LJM is as in the previous report [4]. In brief, the angle was measured while subjects lifted their hands off the table with the fingers fixed flat on the table [Figure 1]. The mean of the angles measured on the right and left hands in individual subjects was used for assessment. Spot urine albumin-to-creatinine ratio was determined and graded as normoalbuminuria (< 30 mg/g creatinine), microalbuminuria (30-300 mg/g creatinine), and macroalbuminuria (>300 mg/g creatinine). The baseline serum creatinine levels were < 1.20 mg/dl.
The data are expressed as the mean ± standard deviation. Statistical analysis was performed using paired t-test, unpaired t-test, χ² test with Yates' correction, Pearson's correlation, multiple regression, or binary logistic regression, where appropriate, with a significant level at P < 0.05. In case of multiple or binary logistic regression analysis, gender was coded as 0 for female and 1 for male; smoking status was graded as 0 for non-smoker, 1 for ex-smoker, and 2 for current smoker; drinking status was graded as 0 for non-drinker, 1 for social or ex-drinker, and 2 for habitual drinker; the use of insulin was coded as 0 for "no" and 1 for "yes;" and albuminuria was graded as 0 for normoalbuminuria, 1 for microalbuminuria, and 2 for macroalbuminuria. Analyses were performed using BellCurve for Excel (Social Survey Research Information Co., Ltd.).
RESULTS
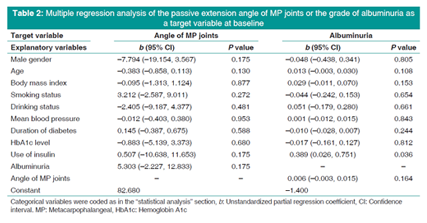
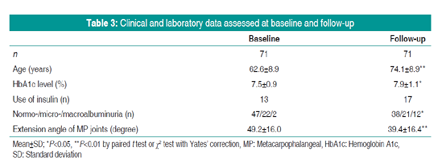
As in Table 1, the passive extension angle of MP joints at baseline was significantly (P < 0.05) smaller in males than in females. The angle of MP joints were significantly correlated with age in males (r = -0.350, P = 0.034) but not in females (r = 0.022, P = 0.903). Table 2 shows multiple regression analysis of the angle of MP joints or the grade of albuminuria as a target variable at baseline. The partial regression coefficient for use of insulin ("yes") was only significant (P < 0.05) when the grade of albuminuria was set as a target variable. The best fitting multiple regression equation by the stepwise method with P = 0.2 was the angle of MP joints = -8.496 X male gender (P = 0.021) -0.389 X age (P = 0.062) + 5.125 X grade of albuminuria (P = 0.134) + 76.065 (adjusted R2 = 0.103, P = 0.016) and the grade of albuminuria = 0.011 X age (P = 0.116) + 0.034 X body mass index (P = 0.056) + 0.312 X use of insulin (P = 0.054) + 0.006 X angle of MP joints (P = 0.159) -1.503 (adjusted R2 = 0.088, P = 0.038). Data assessed at follow-up in comparison with those at baseline are shown in Table 3. There were significant differences between them in hemoglobin A1c (HbA1c) level, albuminuria, and angle of MP joints; HbA1c level increased, albuminuria worsened, and the angle of MP joints decreased at follow-up.
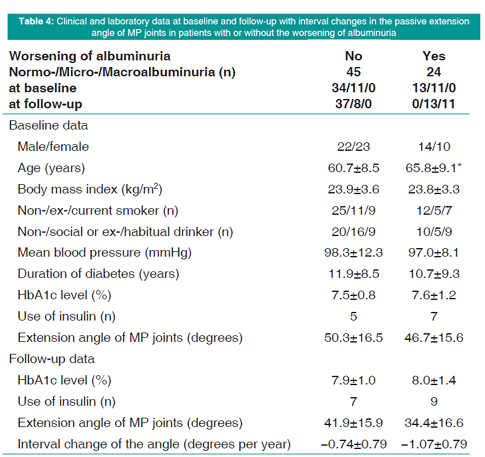
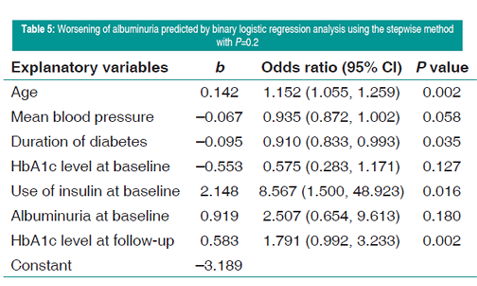
Excluding two patients with macroalbuminuria at baseline, the remaining patients were divided into two groups by "yes" or "no" for the worsening of the grade (0 or 1-1 or 2) of albuminuria at follow-up. Table 4 shows clinical and laboratory data at baseline and follow-up, including interval changes (per year) in the extension angle of MP joints in two groups. Patients with the worsening of albuminuria were significantly (P < 0.05) older than patients without and tended to have smaller angles of MP joints and higher frequencies of insulin use at baseline and follow-up. When the worsening of albuminuria (1 for "yes" and 0 for "no") was predicted by binary logistic regression analysis using the stepwise method with P = 0.2, partial regression coefficients were significant (P < 0.05) for age, duration of diabetes, use of insulin at baseline, and HbA1c level at follow-up [Table 5]. The explanatory variables of the extension angle of MP joints at baseline and follow-up and its interval change were excluded.
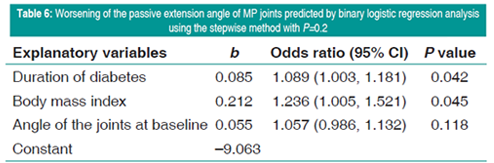
When patients were divided by the median value of the angle of MP joints at baseline (45° for male and 50° for female), patients with smaller angles of MP joints than the median value tended to have a higher frequency of the worsening of albuminuria (12/24 [50.0%]) than the other patients (12/45 [26.7%]) (P = 0.053, χ² test). Among patients with the angle of MP joints at baseline =45° for males and 50° for females, the worsening of the angle of MP joints, which was regarded as the decrease of the angle >10° at follow-up (1 for "yes" and 0 for "no"), was predicted by binary logistic regression analysis using the stepwise method with P = 0.2. Partial regression coefficients were significant (P < 0.05) for the duration of diabetes and body mass index at baseline [Table 6]. The explanatory variables of albuminuria at baseline and follow-up and the worsening of albuminuria were excluded.
DISCUSSION
In general, joint ranges of motion are affected by age and gender, depending on the segments of joints [6,7]. The present study in patients with type 2 diabetes, similar to the results of another study population in our previous report,[5] demonstrated that the passive extension angles of MP joints were smaller in males than in females and correlated negatively with age in males but not in females. The influence of age on the passive range of motion of peripheral joints seems to be little in females [8]. A multiple regression analysis was performed using 10 explanatory variables including age and gender to predict the angle of MP joints or the grade of albuminuria at baseline. When using all 10 explanatory variables, the partial regression coefficient for the use of insulin was only significant in case of the grade of albuminuria as a target variable. When using the stepwise method, the partial regression coefficient for male gender was only significant in case of the angle of MP joints as a target variable. At 10-12-year follow-up, it was apparently observed that the passive extension angles of MP joints decreased and the grades of albuminuria progressed. Patients whose grades of albuminuria worsened were significantly older and tended to have smaller angles of MP joints compared with patients without the worsening of albuminuria. Binary logistic regression analysis using the stepwise method demonstrated that the worsening of albuminuria could be predicted by age, duration of diabetes (negatively), and use of insulin at baseline and HbA1c level at follow-up. Similarly, it was demonstrated that the decreasing (>10°) of the angle of MP joints could be predicted by duration of diabetes and body mass index at baseline. In this case, patients whose angles of MP joints were equal to or larger than the median value of 45° for males and 50° for females were analyzed. There is a report [9] describing that the passive extension angle of MP joints >60° or < 45° was regarded as normal or definitely abnormal.
Thus, the present long-term observation study suggested that the passive extension angle of MP joints to quantitatively assess LJM was affected by male gender, aging, high body mass index, and long duration of diabetes but did not well predict the progression of early diabetic nephropathy. The progression of early diabetic nephropathy was suggested to be associated with aging, use of insulin, and poor glycemic control but not long duration of diabetes. Taken together with the results of our previous report [5] (possible common factors contributing the decreased angle and arteriosclerosis), it is inferred that the decreasing of the angle of MP joints is rather associated with arteriosclerosis than early diabetic nephropathy. Other follow-up studies using common methods to identify LJM in type 1 diabetes have demonstrated inconsistent results on the relationship between LJM and diabetic nephropathy [10-13]. In contrast to our study, a cross-sectional study in younger patients with type 1 (age, 31.7 ± 10.5 years) indicated that microalbuminuria, but not LJM, was associated with risk factors of cardiovascular disease [14]. In patients with type 2 diabetes, it was reported that age, duration of diabetes, and occupation, but not microvascular complications, correlated with LJM [15]. It would be worth elucidating further the relationship between LJM, diabetic nephropathy, and macrovascular disease, all of which are involved in AGEs [1,16-18].
CONCLUSIONS
Taken together with our previous report, it is inferred that the decreasing of the angle of MP joints is rather associated with arteriosclerosis than early diabetic nephropathy. It would be worth elucidating the relation between LJM, diabetic nephropathy, and macrovascular disease, all of which are involved in AGEs.
REFERENCES
- Abate M, Schiavone C, Pelotti P, Salini V. Limited joint mobility in diabetes and ageing: Recent advances in pathogenesis and therapy. Int J Immunopathol Pharmacol 2010;23:997-1003.
- Fessel G, Li Y, Diederich V, Guizar-Sicairos M, Schneider P, Sell DR, et al. Advanced glycation end-products reduce collagen molecular sliding to affect collagen fibril damage mechanisms but not stiffness. PLoS One 2014;9:e110948.
- Sternberg M, M'bemba J, Urios P, Borsos AM, Selam JL, Peyroux J, et al. Skin collagen pentosidine and fluorescence in diabetes were predictors of retinopathy progression and creatininemia increase already 6years after punch-biopsy. Clin Biochem 2016;49:225-31.
- Macedo LG, Magee DJ. Differences in range of motion between dominant and nondominant sides of upper and lower extremities. J Manipulative Physiol Ther 2008;31:577-82.
- Aoki Y, Yazaki K, Shirotori K, Yanagisawa Y, Oguchi H, Kiyosawa K, et al. Stiffening of connective tissue in elderly diabetic patients: Relevance to diabetic nephropathy and oxidative stress. Diabetologia 1993;36:79-83.
- Doriot N, Wang X. Effects of age and gender on maximum voluntary range of motion of the upper body joints. Ergonomics 2006;49:269-81.
- Hwang J, Jung MC. Age and sex differences in ranges of motion and motion patterns. Int J Occup Saf Ergon 2015;21:173-86.
- Macedo LG, Magee DJ. Effects of age on passive range of motion of selected peripheral joints in healthy adult females. Physiother Theory Pract 2009;25:145-64.
- Campbell RR, Hawking SJ, Maddison PJ, Reckless JPD. Limited joint mobility in diabetess mellitus. Ann Rheum Dis 1985;44:93-7.
- McCance DR, Crowe G, Quinn MJ, Smye M, Kennedy L. Incidence of microvascular complications in Type 1 diabetic subjects with limited joint mobility: A 10-year prospective study. Diabetic Med 1993;10:807-10.
- Arkkila PET, Kantola IM, Viikari JSA, Ronnemaa T, Vahatalo MA. Limited jount mobility is associated the presence but does not predict the development of microvascular complications in Type 1 diabetes. Diabetic Med 1996;13:828-33.
- Amin R, Bahu TK, Widmer B, Dalton RN, Dunger DB. Longitudinal relation between limited joint mobility, height, insulin-like growth factor 1 levels, and risk of developing microalbuminuria: The oxford regional prospective study. Arch Dis Child 2005;90:1039-44.
- Labad J, Rozadilla A, Garcia-Sancho P, Nolla JM, Montanya E. Limited joint mobility progression in Type 1 diabetes: A 15-year follow-up study. Int J Endocrinol 2018;2018:1897058.
- Montana E, Rozadilla A, Nolla JM, Gomez N, Escofet DR, Soler J. Microalbuminuria is associated with limited joint mobility in Type 1 diabetes mellitus. Ann Rheum Dis 1995;54:582-86.
- Rajendran SR, Bhansali A, Walia R, Dutta P, Bansal V, Shanmugasundar G. Prevalence and pattern of hand soft-tissue changes in Type 2 diabetic mellitus. Diabetes Metab 2011;37:312-7.
- Yu Y, Thorpe SR, Jenkins AJ et al. Advanced glycation end-products and methionine sulphoxide in skin collagen of patients with Type 1 diabetes. Diabetologia 2006;49:2488-98.
- Goldin A, Beckman JA, Schmidt AM, Creager MA. Advanced glycation end products sparking the development of diabetic vascular injury. Circulation 2006; 114:597-605.
- Ahmad S, Siddiqui Z, Rehman S, Khan MY, Khan H, Khanum S, et al. A glycation angle to look into the diabetic vasculopathy: Cause and cure. Curr Vasc Pharmacol 2017;15:352-64.