Acute Graft-versus-host Disease Following Autologous Stem Cell Transplant for Multiple Myeloma
Sanjeev Kumar Sharma1, Divya Doval1, Dharma Choudhary1, Vipin Khandelwal1, Meet Kumar1, Anil Handoo1, Pawan Kirtani2, Veena Malhotra2
2. Department of Histopathology, BLK Super Speciality Hospital, New Delhi, India
Citation: Sharma SK, Doval D, Choudhary D, Khandelwal V, Kumar M, Handoo A, Kirtani P, Malhotra V. Acute Graft-versus-host Disease Following Autologous Stem Cell Transplant for Multiple Myeloma. Clin Res Hematol 2018;1(1):1-3.
Graft-versus-host disease (GVHD) has rarely been reported after autologous stem cell transplant (ASCT). GVHD risk is more after ASCT for multiple myeloma compared to lymphoma. Clinical manifestations and treatment of acute GVHD post ACST are similar to those after allogenic SCT. We report here our experience of acute GVHD following ASCT for multiple myeloma.
Autologous graft-versus-host disease, autologous stem cell transplant, multiple myeloma
INTRODUCTION
Graft-versus-host disease (GVHD) is common after allogeneic hematopoietic stem cell transplant (SCT) but has rarely been reported after autologous stem cell transplant (ASCT). Acute GVHD after ASCT can involve the gastrointestinal tract and rarely the skin and liver and presents with diarrhea, skin rash, and jaundice, respectively, similar to that in allogeneic SCT. Early recognition and prompt treatment can reduce disease progression, morbidity, and mortality. We report here four patients of multiple myeloma who developed acute gut GVHD following ASCT. All patients showed complete recovery after treatment except one patient who later develops chronic GVHD, requiring prolonged immunosuppression.
CASE REPORT
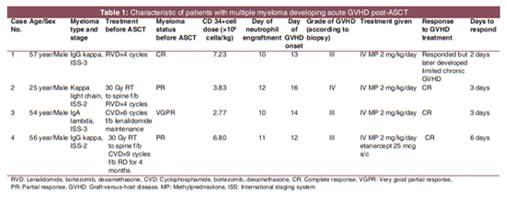
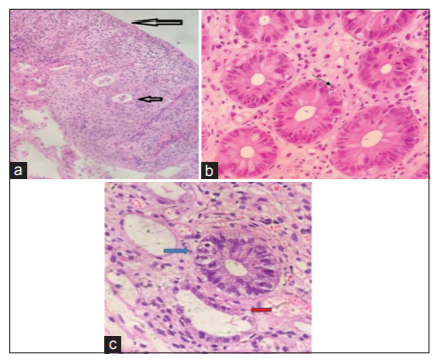
A total of 207 patients underwent ASCT at Bone Marrow Transplant center of BLK Super Speciality Hospital from January 2010 to December 2017, of which 135 had multiple myeloma, and others had lymphoma (Hodgkin and non-Hodgkin) and acute promyelocytic leukemia. Autologous acute GVHD developed in 4 patients all of whom had multiple myeloma. We retrospectively analyzed the data of these patients developing autologous GVHD. The study was approved by Hospital Ethical committee. The patient characteristics and outcome have been described in Table 1. Of these four patients, two had received RVD (lenalidomide, bortezomib, and dexamethasone) and two had received CVD (cyclophosphamide, bortezomib, and dexamethasone) before ASCT. All patients received melphalan 200 mg/m2 as conditioning regimen. The median stem cell dose was 5.31 X 106 cells/kg (range, 2.77-7.33 X 106 cells/kg). The median days of neutrophil and platelet engraftment were 10.5 (range, 10-12) and 17 (range, 15-23) days, respectively. All patients developed green-colored, large volume, watery loose stools after engraftment (median 13.5 days of ASCT) clinically suggestive of acute gut GVHD. Patients were evaluated for infective causes of diarrhea including stool examination for Clostridium difficile and blood cytomegalovirus-polymerase chain reaction, and all were negative. Sigmoidoscopy was done in all patients and histopathology of the specimens showed evidence of gut GVHD with apoptosis in crypts, cryptitis, and crypt loss in focal areas [Figure 1a-c].
The patients were treated with intravenous methylprednisolone 2 mg/kg as the first-line treatment. One patient also required second-line treatment with etanercept. All patients recovered with the treatment after a median of 3.5 days (range, 2-6 days). The steroids were tapered over 2 weeks. After a median follow-up of 7 months (range 2-10 months), all patients are in remission for GVHD, except one patient who later develop chronic GVHD (limited and oral), requiring prolonged treatment with steroids.
DISCUSSION
Autologous GVHD is a rare condition which has been reported in patients undergoing autologous SCT for multiple myeloma [1]. Of 135 patients who underwent ASCT for multiple myeloma at our center over 8 years period, four patients (3%) developed acute gut GVHD. All these patients presented early after ASCT with copious watery diarrhea clinically suggestive of gut GVHD. Biopsy and histological examination in all cases revealed features consistent with gut GVHD and patients showed dramatic response to systemic steroids. Batra et al. reported autologous GVHD in eight patients undergoing ASCT for multiple myeloma, six of whom did not respond to steroids well and required extracorporeal photopheresis [1]. Drobyski et al . reported the outcome of 386 patients undergoing ASCT, of whom 26 underwent a second ASCT [2]. Five patients, all of whom had multiple myeloma, developed acute GVHD with severe skin rash and diarrhea. Three of the five patients developed GVHD after their second transplant.
The common causes of diarrhea post-ASCT include melphalan-induced mucositis, bacterial and viral infections, and drugs. Rarely, mucositis can be severe and life-threatening [3]. Autologous GVHD, though rare, should be considered in the differential diagnosis of severe unexplained diarrhea after ASCT.
In allogeneic SCT, the GVHD is due to an immunologic attack on the recipient's skin, gastrointestinal tract, and liver by donor lymphocytes due to the mismatch of histocompatibility antigens [4]. However, patients undergoing ASCT do not have this mismatch, and therefore, pathophysiology of GVHD after ASCT is mainly due to diminished self-tolerance secondary to an altered immune system [1,2]. Newer drugs used for multiple myeloma treatment such as immunomodulators and proteasome inhibitors, both of which our patients had received, have been postulated to alter regulatory T-cell function that could potentially lead to GVHD in these patients [5]. The prevalence has been found to be consistently higher among patients with multiple myeloma compared to lymphoma [1,2]. The diagnosis and management of autologous GVHD are similar to that of acute GVHD after allogeneic SCT. These cases highlight the need for high index of suspicion of autologous GVHD, particularly in multiple myeloma patients, and need urgent treatment.
ACKNOWLEDGMENT
We are thankful to Ms. Bharti Sharma for compiling the data.
References
- Batra A, Cottler-Fox M, Harville T, Rhodes-Clark BS, Makhoul I, Nakagawa M, et al. Autologous graft versus host disease: An emerging complication in patients with multiple myeloma. Bone Marrow Res 2014;2014:891427.
- Drobyski WR, Hari P, Keever-Taylor C, Komorowski R, Grossman W. Severe autologous GVHD after hematopoietic progenitor cell transplantation for multiple myeloma. Bone Marrow Transplant 2009;43:169-77.
- Sharma SK, Handoo A, Choudhary D, Dhamija G, Gupta N. Severe gastrointestinal mucositis following high dose melphalan therapy for multiple myeloma. World J Gastroenterol 2013;19:784-5.
- Couriel D, Caldera H, Champlin R, Komanduri K. Acute graft-versus-host disease: Pathophysiology, clinical manifestations, and management. Cancer 2004;101:1936-46.
- Galustian C, Meyer B, Labarthe MC, Dredge K, Klaschka D, Henry J, et al. The anti-cancer agents lenalidomide and pomalidomide inhibit the proliferation and function of T regulatory cells. Cancer Immunol Immunother 2009;58:1033-45.