A Deadly Mistake in Treatment of Parkinson's Disease
Knox Van Dyke
Citation :Van Dyke K. A Deadly Mistake in Treatment of Parkinson's Disease. Clin Res Immunol.2018;1(1):1-3.
Abstract
The treatment of Parkinson's disease (PD) has evolved from drugs that are mostly symptomatic to substances which if used correctly can actually slow down the progression of the disease. The first major discovery for PD was made when Professor Arvid Carlssen suggested the use of L-DOPA for treatment - which increases the amount of the key transmitter dopamine in the dopaminergic nerves in the substantia nigra where brain dopamine is synthesized, stored, and released, as well as recycled. A variety of scientists have now developed the idea that the Nurr-1 transcription factor and receptor are the controller of the various activity of brain dopamine whose depletion causes PD. However, Kim et al. discovered chloroquine which is the first effective agonist which binds to Nurr-1. Chloroquine, an antimalarial drug, actually stimulates the formation of dopamine - while it, apparently, protects against toxic activity from activated microglia producing harmful peroxides. Using this knowledge, Kim et al. demonstrated that chloroquine or similar antimalarial drugs are effective against animal models of PD. However, a combination therapy (carbidopa [CD]/levodopa) presently heavily used today to treat PD rather than decreasing death rate as was observed with L-DOPA alone actually increases the PD death rate 4 fold. The use of CD depends crucially on the drug not entering the brain. However, PD causes the blood-brain barrier to become leaky as does increasing age and it is herein proposed that if and when CD enters the brain, it prevents the L-DOPA from forming dopamine because CD is an amino acid decarboxylase inhibitor which would prevent L-DOPA from forming dopamine - a necessary neurotransmitter for movements and life itself. We propose that this is likely why this drug combination is shortening the lives of people with PD. There are approximately 1 million people in the USA with PD most of who are taking the wrong drug combination for their disease. There are many millions more around the world with PD who should change their treatment accordingly.
Carbidopa, chloroquine, EPA, fish oil-DHA, L-DOPA, Parkinson's disease, L Tyrosine
INTRODUCTION
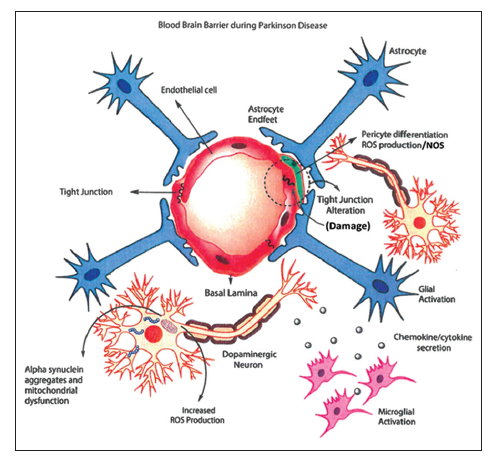
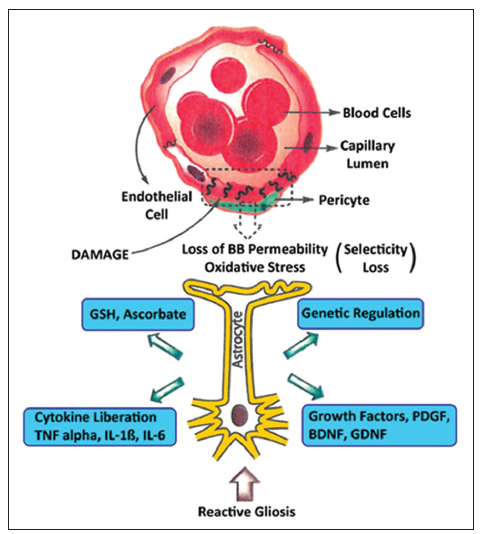
The blood-brain barrier (BBB) is the important interface between the central nervous system (CNS) which regulates molecular movement in and out of the brain creating CNS homeostasis. Its composition is mainly endothelial cells, pericytes, and astrocytes thus creating a neurovascular unit surrounded by adjacent neurons. Astrocytes are crucial for both information and maintenance of the BBB by secreting factors leading to the adequate and strong association of the cells of the BBB and strong junction formation. Various disease states, for example, Alzheimer's, Parkinson's, multiple sclerosis and different forms of dementia, brain trauma, and chronic cerebral ischemia there is a disruption of the BBB creating a loss of proper permeability of the carrier and concomitant physical changes in endothelial cells and astrocytes. Reactive gliosis is a common astrocytic feature during BBB damage which affects barrier function and neuronal survival.
Damage to BBB function is a fundamental characteristic of various diseases and physical damage to the brain. Since the BBB functions to allow certain nutrients and ions to enter the brain, it also functions to keep out cells and materials that could be detrimental to the brain. It is generally known that for every 100 drugs used by humans only 2 of the 100 actually are allowed to penetrate into the brain, so there is a clear selectivity for different substances entering the brain. Figures 1 and 2 demonstrate the damage to the BBB from either diseases or trauma to the brain.
One aspect of the BBB which is not always appreciated is that this barrier functions a little differently in some people than others. For example, the newer H1 antihistamines are not supposed to penetrate the BBB, and therefore they cannot make you sleepy. However, it is well known that some people that are normal otherwise do get sleepy from these drugs, indicating that these H1 antihistamines do get into their brains. Another aspect of the BBB that is not always appreciated is that as people get older that the BBB becomes leaky. Naturally, many older people begin to have chronic diseases after the age of 50 and either the change in years or the disease or the combination of the two causes increase in BBB leaking. Parkinson's disease (PD) is a chronic and progressive neuroinflammatory disorder caused by the death of the dopaminergic neurons in the substantia nigra. This a movement disorder which includes asymmetrical bradykinesia (slow movement), rigidity, resting tremor, and postural instability. The initiation and progression of the disease are likely caused by oxidative/nitrosative stress and mitochondrial dysfunction, apoptosis and necrosis with increases in autophagy.
Our original discovery was that continual and sustained use of a mixture of various antioxidants could actually slow the progression of neurodegenerative diseases such as PD Van Dyke and Sacks,[1,2] and Schwarzschild [3] indicates that early treatments with sustained release Vitamin C, Vitamin E (tocotrienols), sustained release inosine or inosine will actually slow progression of the early disease.
In 1960, Professor Carlssen [4] introduced dihydroxy phenylalanine (L-DOPA) into clinical treatment of PD. From 1960 to 1975, the death rate from PD actually decreased. However, L-DOPA was partially converted to dopamine outside the brain (in the periphery) causing side effects - nausea and low blood pressure. Merck Sharpe and Dohme introduced carbidopa (CD) to be taken in combination with L-DOPA - and in Europe, benserazide is added to L-DOPA instead of CD to alleviate side effects of L-DOPA. However, 40% of these patients using the combination of the two drugs used in Europe or the USA also caused motor fluctuation and dyskinesia. In addition, and more importantly - from 1975 to present day 2018 - the death rate of Parkinson's patients taking the combinational drugs increased 4 fold. This is an unacceptable situation, created by drug manufacturers and the government not watching PD death rate figures of patients using these drugs. One wonders why retrospective studies have not been done on these drug combinations. It is likely that drug acceptance has escaped scrutiny because acceptance happened so long ago.
Hinz and Cole [5] mentioned that CD and benserazide both react with Vitamin B6 through Schiff base formation. Once this covalent complex is formed, the Vitamin B6 cannot react to create important amino acid transamination reactions. Normally, there are 9 essential amino acids, but 20 amino acids are needed. The 20 amino acids have to be produced using biochemical changes to the 9 essential amino acids, and if Vitamin B6 is bound to one of the two drugs, this essential transamination cannot occur. This creates a nutritional disaster. However, can it be the main cause of the increased death rate? It certainly could be a contributing factor. However, since many of the PD patients are over the age of 65, it is quite likely that a leaky BBB may play a large role because it is known that age and PD can become an important factor in BBB leakiness [6]. If either CD or benserazide entered the brain through a leaky barrier - it could inhibit the amino acid decarboxylase which forms dopamine from L-DOPA. Without sufficient dopamine, life cannot exist. Further, the tachyphylaxis effect of L-DOPA or (its dwindling effect) could be explained because less dopamine would be formed over time and this produces a deficient amount of dopamine. In other words, if there is less production of dopamine, it could be related to a less actual hormone produced over time caused by an amino acid decarboxylase inhibitor.
We suggest a different method to increase the production of dopamine and protect the damage to dopaminergic neurons. First, take orally, L-tyrosine at least 500 mg every 8 h. L-tyrosine is the natural supplement that produces dopamine. It is readily taken into the brain using specific transporters and enters the Nurr-1 complex in the dopaminergic neurons. The enzymes of the Nurr-1 complex convert the tyrosine to dihydroxyphenylalanine (DHA) using tyrosine hydroxylase. The DHA is then decarboxylated using amino acid decarboxylase to form L-dopamine [7]. The dopamine is stored, released and even taken back by reuptake mechanism to be reused. We propose a more complete list of substances which will help to prevent and control PD.
Ingredients to prevent or slow progression of PD:
- Inosine - 4 g/day in divided doses inosine or sustained release inosine.
- Tocotrienol - special form of Vitamin E capsules -1 capsule every 12 h. Available from Endurance Products - Oregon.
- Fish oil with omega 3 fatty acids - DHA/EPA (500- 1000 mg/day); make sure they are coated tablets.
- Sustained release 5 hydroxytryptophan - 500 mg every 12 h.
- L-tyrosine - at least 500 mg capsules every 8 h.
- Astrazanthin capsules 12 mg/day.
- Krill oil - 1 capsule/day.
- Tylenol - arthritis formula-sustained release 2-650 mg tablets/8 h.
- N- acetylcysteine sustained release - 600 tablet take 1/day
- Sustained release niacinamide - 500 mg tablets - take 2-3/day get from endurance products, Oregon.
- Levo-DOPA/carbidopa dose determined by the physician and best avoided because of toxicity. If Levo-DOPA alone would be available, this would be a more judicious choice.
- Chloroquine 200-300 mg every 3rd day. The dose and timing should be confirmed by a physician.
- Vitamin C - 2 g every 12 h or sustained release Vitamin C - 2 g every 12 h.
REFERENCES
- Van Dyke K, Sacks M. Use of a Combination Comprising of a Precursor of Uric Acid and Antioxidant for the Treatment of Neurodegenerative Diseases Euopean Patent - EP No. 110507B1.
- Van Dyke K, Sacks M. Compositions for Raising Uric Acid Level and Methods for Using the Same USA Patents No. 20120241006, 20040176306.
- Schwarzschild MA. Study of Urate Elevation in Parkinson's Disease-Phase 3 (SURE-PD3)-NCT No. 92642393.
- Carlssen A. Perspectives on the discovery of central monoaminergic neurotransmission. Ann Rev Neurosci 1987;1:179-86.
- Hinz M, Cole T. The Parkinson's disease death rate: Carbidopa and vitamin B6. Clin Pharmacol Adv Appl 2014. DOI:10.20147/cpaa.570707.
- Cabezas R, Avila M, Gonzalez J, El-Bacha RS, Baez E, Garcia-Segura LM, et al. Astrocytic modulation of blood brain barrier: Perspectives on Parkinson's disease. Front Cell Neurosci 2014;8:211.
- Kim CH, Han BS, Moon J, Kim DJ, Shin J, Rajan S, et al. Nuclear receptor Nurr1 agonists enhance its dual functions and improve behavioral deficits in an animal model of Parkinson's disease. Proc Natl Acad Sci U S A 2015; 112:8756-61.