Confabulation: Etiology, Typology, and Intervention
Jerrod Brown1,2,3, Deb Huntley2, Steve Morgan3
2.Pathways Counseling Center, Inc., St. Paul, MN, USA,
3.American Institute for the Advancement of Forensic Studies, St. Paul, MN, USA
Citation : Brown J, Huntley D, Morgan S. Confabulation: Etiology, Typology, and Intervention. Clin Res Neurol 2018;1(1):1-4.
Confabulation is an inaccurate memory that results from a distortion or fabrication of thoughts about oneself or the surrounding environment. Confabulations can range from small changes to a memory of an actual event to the grand generation of a new memory of an event that never took place. In the context of confabulation, these inaccurate memories are created and maintained in the absence of any intent to deceive others. The potential for confabulation is particularly dangerous in the criminal justice system where many legal processes rely on self-reported information (e.g., police interviews, interrogations, and eyewitness testimony). Here, confabulation can have a profound impact throughout the criminal justice system and results in miscarriages of justice (e.g., false confessions and wrongful convictions). As such, it is imperative that clinical and forensic mental health professionals develop and hone screening, assessment, and treatment skills that are appropriate for clients with the potential of confabulation. Unfortunately, opportunities for advanced education and training on the topic of confabulation are few and far between. To provide a primer on confabulation in clinical and forensic settings, this article defines confabulation, discusses the etiology and risk factors for confabulation, and reviews viable screening, assessment, and treatment approaches for confabulation through a thorough review of the existing empirical research on the topic.
Confabulation, forensic mental health professional, intervention, screening, training ,Neurology,asclepiusopen
CONFABULATION: A BRIEF OVERVIEW
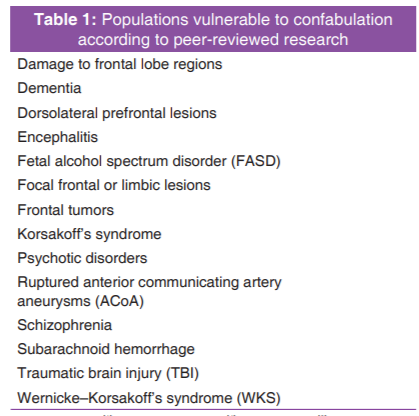
Scholars have argued that self-deception can be described as a continuum, ranging from not giving full attention or credibility to beliefs that are contrary to one's value system to delusions. On that continuum is forms of false memory such as confabulations[22]. Confabulation refers to the unintentional false reporting of a memory and is experienced by both individuals diagnosed with psychiatric and neurological disorders [Table 1][36] as well as those without making the phenomenon important for both clinical and forensic mental health professionals to understand.
Ranging from slight deviations to non-factual claims,[7] confabulations are delivered sincerely[23] and are unique from other forms of false reporting such as malingering, which involves purposeful deviation to achieve a secondary gain[41]. Confabulators fully believe their made-up statements. As stated by Hirstein,[22] "confabulators don't know that they don't know what they claim" (p. 209). Confabulated memories are most often episodic or autobiographical in nature. Confabulation is not an uncommon phenomenon, especially in certain populations. For example, in a study by Kessels et al.,[28] they examined confabulation behavior in 19 Korsakoff patients and found all 19 of them to have demonstrated evidence of confabulation. Despite its common occurrence, confabulation remains a misunderstood phenomenon surrounded by many misconceptions. Hence, the aim of the present article is to delineate the etiology, types, and interventions that have been proposed to assist clinical and forensic mental health professionals in dealing with this unique behavior.
ETIOLOGY OF CONFABULATION
The etiology of confabulation is currently uncertain, but there does not appear to be a single cause agent. Hippocampal functioning may be compromised in persons who confabulate, resulting in deficits in both the correct encoding and subsequent decoding of memories. When several memories contain similar features, they can become confused when being retrieved, [26]with elements of each being reported. When the incorrect memory is easier to access (e.g., overlearned) or has more emotional significance, it may be retrieved in place of the correct memory. For example, research has found that pleasant or favorable memories are easier to retrieve than unpleasant or unfavorable ones,[17,18] as there is an unconscious motive to promote positive traits[19]. The frontal lobe of the cerebral cortex - the area of the brain implicated in combining memories with executive functions (e.g., judgment, inhibition, and attention) - may also play a role, as persons who confabulate are unable to monitor their memories for accuracy before communicating them[40]. Disinhibition of false memories may also be caused by an individual's inability to self-monitor their behavior and mental state, increasing their suggestibility and likelihood of "person pleasing" without realizing it.
Another cause of confabulation that has been noted is problems with temporal memory, as evidenced by misplacing a memory into the wrong time frame[37]. The memory of the event is accurate, but the subject places it in a different chronology. Motivational factors, such as the need to recall information when pressured, are another view of what may lead to confabulations. Subjects may remember incorrect information when pressured, as in interrogations,[27] when repeatedly questioned,[39] when incorrect information is suggested[27], or when the subject is stressed or depressed[16]. Fotopoulou[16] writes that confabulations help preserve a sense of identity. This need to define one's self is vulnerable to motivational influences.
PROVOKED CONFABULATION AND SPONTANEOUS CONFABULATIONS
The two of the most common types of confabulation found in the literature include provoked confabulation and spontaneous confabulations. Often occurring when an individual feels driven to say something, such as the context of a memory task during a psychological assessment, provoked confabulations are normal responses attributable to a deficient memory or resulting from iatrogenic questioning or prompts[27]. Spontaneous confabulations, on the other hand, are unprompted and occur outside the circumstance of questioning or assessment. More rare than provoked confabulations, persons who spontaneously confabulate often eventually stop this behavior[37,38]. Although it has been argued that both provoked and spontaneous confabulations can be considered different expressions of the same cognitive deficit, other scholars maintain that the two types are unique in their neurological underpinnings[14,34]. Regardless of the type, it is a common misconception that confabulations are simply spoken or written down. On the contrary, behavioral confabulation may occur. For example, an individual who has mistakenly reported that he still works at a gas station despite having been retired for 15 years may have an emotional reaction to his sincerely reported false memory, resulting in him getting dressed for work and reporting for duty at the gas station the next day.
INTERVENTION AND SCREENING
Some forms of confabulation resolve with time, but intervention may be necessary in refractory cases to assist the individual in gaining insight as well as learning strategies to reduce the frequency of his or her confabulating. These interventions may be focused on improving functional behaviors or on cognitive issues such as executive function, source monitoring, or memory retrieval[16]. It is also helpful to meet with the family to help them understand the nature of confabulation and provides support. Families can be directed to gently challenge the false memories or provide additional, factual information that modifies or replaces the erroneous memories. Regardless of the form of treatment delivered, practitioners should perform (or have performed by a qualified professional) a thorough psychiatric and neurological examination and corroborate the information gathered both through file review and additional interviewing of collateral sources (both familial and non-familial)[2,24]. Routine intake screening for confabulation is important, as such behavior can negatively impact diagnostic assessment results and treatment outcomes[25]. Use of an evidence-based procedure is crucial, as individuals who confabulate will not self-report such behavior because they usually lack insight into having a memory deficit or underestimate its impact on their functioning[31]. Empirical instruments have been employed by some to measure the likelihood of confabulation. For example, Barba et al.[13] employed what is called a "Don't Know" test. This test asks the respondent to answer questions of varying difficulty with some questions being so hard that it is highly unlikely that the average person would know the answer. On these questions, the non-confabulator would respond "I don't know", whereas the confabulator would be far less likely to respond "I don't know" and instead make up an answer. The fewer the "I don't know" responses (relative to normal controls), the higher the likelihood of confabulation.
If confabulation or a history of confabulation is detected, an ongoing fact-checking procedure will likely be necessary to verify and subsequently document confabulations during the course of treatment - tracking the frequency and severity of the confabulations is advisable to monitor progress[6,9] This ongoing procedure should include a process by which discrepancies in the individual's self-reports are identified and addressed. During treatment, practitioners are advised to remind themselves that such behavior is unintentional - remembering this will help establish a helpful working rapport[10]. In addition, such reminders will prevent unnecessary countertransference brought about by the confabulation[11].
CONCLUSION
In summary, confabulation is a disturbance of memory that results in the unintentional distortions, fabrications, or misinterpretations of memories. Professionals should remember that individuals who confabulate do not necessarily have psychiatric or neurological disorders, but rather may have confabulated in the context of a number of environmental and social circumstances. As part of their routine continuing education recertification process, mental health professionals should consider taking trainings on the evidence-based identification and treatment of confabulation. Such trainings will aid them in developing useful and effective skillsets when working with individuals at risk for confabulation. Mental health professionals interested in increasing their awareness, knowledge, and understanding of confabulation and its impact on clinical and forensic mental health settings should consider engaging in the following:
1) Review new additions to the scientific research literature on a continuous basis.
2) Utilize in-person and online educational resources on confabulation as part of continuing education training on an annual basis.
3) Collaborate with mental health professionals who can provide both accurate screening for confabulation and expert testimony to educate the court about the impact of this phenomenon.
By equipping themselves with the knowledge presented in this article and with a commitment to following the above recommendations, mental health professionals will be in a better position to more effectively serve clients who confabulate and produce significantly more positive outcomes.
REFERENCES
- Berlyne N. Confabulation. Br J Psychiatry 1972;120:31-9.
- Brown J. Fetal alcohol spectrum disorder and confabulation: A clinical, forensic, andjudicial dilemma. J Spec Popul 2017;1:1-11.
- Brown J, Charette C, Huntley D, Wartnik AP, Wiley CR, Cich J, et al. Confabulation: A beginner's guide for legal professionals. For Sci Criminol 2017;2:1-5.
- Brown J, Charette C, Morgan S. Wernicke-korsakoff syndrome and memoryimpairments: Considerations for criminal justice and forensic professionals. J Spec Popul 2016;1:1-8.
- Brown J, Fordice H, Weaver J, Hesse M. Wernicke-korsakoff syndrome and confabulation: A review for criminal justice professionals. Behav Health 2015;3:1-8.
- Brown J, Haun J, Zapf PA, Brown NN. Fetal alcohol spectrum disorders (FASD) and competency to stand trial (CST): Suggestions for a 'best practices' approach to forensic evaluation. Int J Law Psychiatry 2017;52:19-27.
- Brown J, Hesse M, Rosenbloom M, Harris B, Weaver J, Wartnik A, et al. Confabulation in correctional settings: An exploratory review. J Law Enforc 2015;4:1-8.
- Brown J, Huntley D, Asp E, Fabrizio K, Wiley CR, Harris B, et al. Traumatic brain injury and confabulation: An introduction for criminal justice and legal professionals. J Spec Popul 2016;1:1-13.
- Brown J, Huntley D, Asp EW, Wiley CR, Cich J, Morgan S. Confabulation: Implications for criminal justice, forensic mental health, and legal professionals. J Neurol Neurosci 2017;8:1-8.
- Brown J, Huntley D, Morgan S, Dodson KD, Cich J. Confabulation: A guide for mental health professionals. Int J Neurol Neurother 2017;4:1-9.
- Chlebowski S, Chung C, Alao A, Pies R. Confabulation: A bridge betweenNeurology and psychiatry?
- Conway MA, Tacchi PC. Motivated confabulation. Neurocase 1996;2:325-39.
- Barba GD, Cipoletti L, Denes G. Different patterns of confabulation. Cortex 1990;29:567-81.
- Barba GD, Nedjam Z, Dubois B. Confabulation, executive functions, and source memory in Alzheimer's disease. Cogn Neuropsychol 1999;16:385-98.
- Fletcher PC, Shallice T, Frith CD, Frackowiak RS, Dolan RJ. The functional roles of prefrontal cortex in episodic memory. II. Retrieval. Brain 1998;121:1249-56.
- Fotopoulou A. False selves in neuropsychological rehabilitation: The challenge of confabulation. Neuropsychol Rehab 2008;18:541-65.
- Fotopoulou A, Conway MA, Griffiths P, Birchall D, Tyrer S. Self-enhancing confabulation: Revising the motivational hypothesis. Neurocase 2007;13:6-15.
- Fotopoulou A, Conway MA, Tyrer S, Birchall D, Griffiths P, Solms M. Is the content of confabulation positive? An experimental study. Cortex 2008;44:764-72.
- Gilboa A, Verfaellie M. Telling it like it isn't: The cognitive neuroscience of confabulation. J Int Neuropsychol Soc 2010;16:961-6.
- Glowinski R, Payman V, Frencham K. Confabulation: A spontaneous and fantastic review. Aust N Z J Psychiatry 2008;42:932-40.
- Hashimoto R, Tanaka Y, Nakano I. Amnesic confabulatory syndrome after focal basal forebrain damage. Neurology 2000;54:978-80.
- Hirstein W. Brain Fiction. Cambridge: M.I.T. Press; 2005.
- Hirstein W, editor. Confabulation: Views from Neuroscience, Psychiatry, Psychology, and Philosophy. USA: Oxford University Press; 2009.
- Huntley D, Brown J. Understanding confabulation: An introduction for criminal justice and mental health professionals. Forensic Scholars Today,2016 1(4), 1-4.
- Huntley D, Brown J, Wiley CR. Confabulation and mental health: A beginner's guide. Behav Health 2016;4:1-9.
- Johnson MK, Raye CL. False memories and confabulation. Trends Cogn Sci 1998;2:137-45.
- Kassin SM, Kiechel KL. The social psychology of false confessions: Compliance, internalization, and confabulation. Am Psychol Soc 1996;7:125-8.
- Kessels RP, Kortrijk HE, Wester AJ, Nys G. Confabulation behavior and false memory in Korsakoff's syndrome: Role of source memory and executive functioning. Psychiatry Clin Neurosci 2008;62:220-5.
- Kopelman MD. Two types of confabulation. J Neurol Neurosurg Psychiatry 1987;50:1482-7.
- Lorente-Rovira E, Santos-Gomez JL, Moro M, Villagran JM, McKenna PJ. Confabulation in schizophrenia: A neuropsychological study. J Int Neuropsychol Soc 2010;16:1018-26.
- McGlynn SM, Schacter DL. Unawareness of deficit in neuropsychological syndromes. J Clin Exp Neuropsychol 198911, 143-205.
- Mercer B, Wapner W, Gardner H, Benson DF. A study of confabulation. Arch Neurol 1977;34:429-33.
- Moscovitch M. Confabulation and the Frontal System: Strategic Versus Associative Retrieval in Neuropsychological Theories of Memory. In: Roediger HL, Craik FI, editors. Varieties of Memory and Consciousness: Essaysin the Honour of Endeltulving. Hillsdale: Lawrence Erlbaum Associates; 1989. p. 133-160.
- Moscovitch M, Melo, B. Strategic retrieval and the frontal lobes: Evidence from confabulation and amnesia. Neuropsychologia 1997;35:1017-34.
- Nedjam Z, Barba GD, Pillon B. Confabulation in a patient with fronto-temporal dementia and a patient with Alzheimer's disease. Cortex 2000;36:561-77.
- Pezdek K. Forced Confabulation. In: Cutler BL, editor. Encyclopedia of Psychology and Law. Thousand Oaks: Sage; 2008. p. 324-5.
- Schnider A. Spontaneous confabulation and the adaptation of thought to ongoing reality. Nat Rev Neurosci 2003;4:662-71.
- Schnider A. Spontaneous confabulation, reality monitoring, and the limbic system-a review. Brain Res Rev 2001;36:150-60.
- Smith P, Gudjonsson GH. Confabulation among forensic inpatients and its relationship with memory, suggestibility, compliance, anxiety, and self-esteem. Pers Individ Dif 1995;19:517-23.
- Turner MS, Cipolotti L, Yousry TA, Shallice T. Confabulation: Damage to a specific inferior medial prefrontal system. Cortex 2008;44:637-48.
- Vitacco MJ, Jackson RL, Rogers R, Neumann CS, Miller HA, Gabel J. Detection strategies for malingering with the miller forensic assessment of symptoms test: A confirmatory factor analysis of its underlying dimensions. Assessment 2008;15:97-103.