Severe Head Injury: Prognostic Factors and Clinical Management
Jose Manuel Ortega Zufiria, Bernardino Choque Cuba, Mario Sierra Rodriguez, Yaiza Lopez Ramirez, Pedro Poveda Nunez, Martin Tamarit Degenhardt, Remedios Lopez Serrano, Noemi Lomillos Prieto, Cristina Dominguez Lubillo
Citation : Zufiria JMO, Cuba BC, Rodriguez MS, Ramirez YL, Nunez PP, Degenhardt MT, Serrano RL, Prieto NL, Lubillo CD. Severe Head Injury: Prognostic Factors and Clinical Management. Clin Res Neurol 2018;1(2):1-14.
Head injury is a very frequent event, associated with high morbidity rates. Classically, more attention has been paid to severe injury. The aim of this study was to describe a large series of adult patients, older than 14 years, who suffer severe head injury, treated at the University Hospital of Getafe, between 1993 and 2015 (n = 86), to study the epidemiological profile, and to analyze the best diagnosis and the treatment carried out, as well as establishing the main prognostic factors that influence the final result. A retrospective study of review of medical records has been carried out and also hospital consultation. In this study, the variables that have been most determinants of the adverse evolution in the patient suffering from severe head injury are age, size, and pupillary reactivity, the worst score obtained by the patient on the Glasgow Coma Scale (GCS) and the lesions found in the computed tomography (CT) of the skull. Lesions in severe head injury can be categorized into nine pathological patterns according to the information provided by the CT. These patterns present an anatomical and clinical profile and a well-defined prognostic significance, associated, in turn, with a behavior pattern of ICP characteristic. Pure extra-axial hematomas are the lesions that present the best prognosis, being the diffuse axonal lesion associated with brain swelling and multiple bilateral contusions which lead to worse evolution. The Rimel scale correctly adjusts to the severity of head injury. The GCS is well related to the final prognosis of the patient with a severe head injury.
Coma, intracranial pressure, severe head injury
INTRODUCTION
In industrialized countries, traumatic injuries are the leading cause of death below 45 years, and brain damage decisively contributes to the fatal outcome in more than half of deaths [1]. The severity of the trauma is undoubtedly the main determinant of the final evolution. Head injury incidence rates vary greatly according to the countries and epidemiological criteria used, ranging from 50 to 4,500/100,000 inhabitants per year [2]. Considering only those that present brain damage data (loss of knowledge, post- traumatic amnesia, or others), the average is 200-300, per 100,000 inhabitants per year. Of the total of cranial traumas, between 75% and 90% of the cases correspond to mild injury, between 5% and 25% to moderate injury, and between 5% and 20% to severe injury, which represents a incidence rate per 100,000 population per year from 150 to 270 for mild injury, from 5 to 60 for the moderate, and from 5 to 50 for the severe, respectively. The great variability of these figures is explained by the fact that they are decisively influenced by the rules for the inclusion and classification of patients employed in the various works. The forces that act on the skull and its contents at the moment of impact are of three types: (I) Contact forces, which affect soft tissues and bone case, and, (II) forces that induce movements of translation, displacing the skull in a transverse or sagittal direction, and (III) forces of angular acceleration, which originate rotation movements. The pathophysiological knowledge of cranial trauma is essential to know the clinical evolution, propose an adequate therapeutic and establish prognostic criteria [3,4].
The prognosis is clearly worse, the higher the patient's age. Children have a better prognosis, although children under 5 years have more mortality than older children or young adults. The mechanism by which age influences negatively is not well known, although it is obvious that the risk increases with factors such as hypertension, arteriosclerosis, and cardiovascular, renal or pulmonary diseases, processes that are more frequent in the elderly. In addition, focal lesions, which generally entail worse prognosis, are more frequent in the elderly (subdural hematomas secondary to falls or aggressions) than in young people (diffuse lesions or epidural hematoma, due to traffic accidents) [5]. It is evident that cerebral atrophy and alterations in cerebral elasticity and vessels predispose to this type of lesions in the elderly. However, the existence of neurological factors that influence the final prognosis is considered, which is less favorable after 45 years regardless of the existence of previous pathologies, and especially after 55 years, especially if there are other associated diseases. When we know more information about the neurobiology of aging, this phenomenon can be clarified. With regard to previous medical pathologies, it is necessary to indicate the high risk of developing intracranial complications in patients with anticoagulant therapy or coagulation disorders, who suffer cranial traumatism [6,7].
The IQ before the trauma has a clear influence on the final cognitive results, and patients with higher educational, economic or professional levels are more likely to return to work. If there is previous emotional instability, there is more risk of suffering psychiatric problems after the injury.
The severity of the injury is undoubtedly the main determinant of the final evolution, as well as the duration of the alteration of consciousness. In severe cranial injury, patients with scores of 3 and 4 have significantly higher mortality than those of 7 and 8, showing a great variability those who score 5 and 6, so in this last subgroup more data are needed to establish prognostic predictions. In this section, it is necessary to indicate that it is estimated that between 10% and 38% of patients with severe injury present a lucid interval in which the physical examination is normal and can be considered mild and subsequently deteriorating to coma. Within the parameters assessed by the Glasgow Coma Scale (GCS) (motor, ocular, and verbal response), the motor response is the one with the greatest prognostic capacity and, therefore, the highest reliability.[8]
Systemic injuries associated with cranial injury are very frequent, and it is estimated that they occur up to 50% of severe injury. Logically, they worsen the prognosis, especially if there is hypotension (in 16% of serious traumas) and hypoxemia (in 37% of them). The thoracic trauma is the systemic lesion that most influences the final evolution of the patient. Extracranial complications that have a significantly greater influence on the final outcome are hypotension, pneumonia, coagulopathy, and septicemia.
Abuses have a worse prognosis, due to the high incidence of associated systemic traumatic injuries, and bicycle or motorcycle accidents have, paradoxically, a better prognosis, mainly due to the younger age average of these patients, always considering the use of helmet. In gunshot wounds, the prognosis depends on the caliber, velocity and trajectory of the projectile, the CT findings, the ICP figures, and the motivation of the incident (suicides have worse evolution).
- Pupillary size and reactivity: Mydriasis and lack of pupillary reflexes indicate poor prognosis. Between 90% and 95% of patients without pupillary reflexes have an adverse course, especially if they are elderly. If these reflexes are normal, only 29% die.
- Oculocephalic and oculovestibular reflexes: If they are absent (data of brain stem injury), between 51% and 95% of patients die, and if they survive, very serious cognitive defects will remain.
The introduction of CT in routine medical practice provided data that cannot be discovered with clinical examination or cerebral arteriography. Patients with very different pathologies can have the same neurological examination and the same Glasgow Coma Scale score, but the type of injury is important in itself, independently of the clinical and the score obtained by the patient. The mortality of patients with scores lower than 9 ranges between 9% and 74% (average of 41%), depends on the type of existing injury. The worst prognosis is associated, in decreasing order, with a subdural hematoma, hemispheric swelling, especially in the elderly, and intracerebral hematomas, especially if they are large or multiple. The deviation of the midline structures also has prognostic value. If it is proportionate to the volume of the lesion, mortality is 39%, and 75% if it is disproportionate to the volume of the lesion. The cisterns of the base also contribute to establish the final evolution. If they are absent, mortality is 72%, 39% if they are compressed, and 22% if they are normal. The compression of the ventricular system and the presence of subarachnoid hemorrhage also worsen the prognosis of the patient suffering from head injury. Finally, it should be remembered that a patient with a normal CT can develop intracranial hypertension if there is associated pulmonary trauma.
The high sensitivity of MRI to detect intraparenchymal lesions makes it a very useful tool in determining the prognosis during recovery of the patient suffering from head trauma, but CT remains the technique of choice during the acute phase,[9] because the exploration with RM lasts a long time, is incompatible with some devices used in ICU, the patient is inaccessible during the examination and, in addition, MRI misdiagnoses subarachnoid hemorrhage. However, in the chronic phase of cranial trauma evolution, MRI detects lesions not visible on CT, mainly in white matter and brainstem, indicating poor neuropsychological recovery and poor prognosis in Glasgow's evolutionary scale.
The elevation of the ICP above 20 mmHg is related to poor prognosis. This is a very reliable parameter, along with age, Glasgow Coma Scale score and pupillary anomalies and is intimately linked to blood pressure figures. In addition, intracranial hypertension causes serious alterations of memory in patients who survive.
Determinations of cerebral blood flow have shown that the presence of hyperemia and/or ischemia is associated with poor prognosis. Studies have also been carried out to quantify the oxygen or glucose consumption index, and the alterations with respect to the normal figures indicate worse evolution.
The responses obtained in the evoked potentials have the advantage that they are non-invasive techniques, do not need the collaboration of the patient and are not influenced by the administration of drugs, although they have a high prognostic reliability, they only value the function of certain pathways and neuronal systems and, in addition, are not available in many centers.
It does not relate well with the final forecast. The deeper the coma, the slower the path, but this is greatly affected by the pharmacological therapy received by the patient.
In general, they do not have good prognostic reliability. Several specific enzymatic markers (creatine phosphokinase, BB isoenzyme, lactate dehydrogenase, and glutamic- oxaloacetic dehydrogenase), catecholamine level (adrenaline and noradrenaline), lactate determination, and coagulation
studies have been studied. Up to 72% of patients with severe trauma have coagulopathies, which are manifested by prolongation of prothrombin time, activated partial thromboplastin or thrombin, decrease in the number of platelets and the number of fibrinogen, and increase in the level of degradation products of fibrin.
A variety of systems have been used to indicate the evolution of cranial injury, from mortality rates to sophisticated methods of assessing organic and psychological sequelae. Mortality rates are the most used and the most useful, because of their easy determination, and because most deaths occur shortly after the injury, and it is not necessary to analyze long periods of time.[10,11] It is estimated that up to 60% of patients with severe injury die at the accident site. In the hospital setting, the first indices published at the beginning of the century gave a 70% mortality rate for severe injury, although the figures range from 30% to 76%, with an average of 40%. Considering only mortality, you do not have a real vision of the problem, because many of the patients who survive are severely affected. The residual defects can be physical (contractures and ossifications), neurological (hemiparesis, seizures, and amaurosis), or psychological (alterations of memory, language, and behavior). The recovery process after a cranial trauma is a dynamic phenomenon, and it is important to decide when to assess the final result. Most authors establish it 6 months after the injury, although this is not a strict criterion that prevents thinking that a patient can improve beyond that date. The probability of developing intracranial injury is very variable, ranging between 30% and 80%.
Cranial injury represents one of the main causes of mortality and morbidity in industrialized countries, which constitutes an effort, both as a human and economic level, very important. CT not only shows the extra or intra-axial major lesions at any time of evolution but also it allows to acquire dynamic information about the pathological changes that occur at the intracranial level, either spontaneously or at the request of different medical therapeutic maneuvers or surgical, and can demonstrate certain pathophysiological changes such as cerebral edema and intracranial hypertension. In fact, follow-up with sequential CT and continuous monitoring of Intracranial Pressure provides a knowledge of the intracranial pathophysiology that was unthinkable to have a few years ago, but there are still wide gaps in the understanding of the pathogenesis that limit the development of a therapeutic scheme optimum. In addition, the clinical model of cranial injury is multifactorial, both clinic-pathological terms and treatment, so it is very difficult to determine the effect of a pathological or therapeutic variable on the evolution or the final prognosis of patients. The progress experienced in the management and treatment of patients suffering from severe head injury has allowed a marked improvement in prognosis. Thus, it has been possible to reduce the mortality rate by up to 30%, without increasing the number of patients who remain in a persistent vegetative state or develop severe disability, according to the criteria of the Glasgow Evolutionary Scale, although it is still close to the 40%. At present, it is necessary to determine the most influential factors in the final evolution to establish prognostic models and to be able to draw up therapeutic action plans and rehabilitation, as effectively as possible. The Glasgow Coma Scale and the scale introduced by Rimel et al., which divides injury into mild, moderate, and severe, are universally accepted. The usefulness of these scales, which estimate the severity and prognosis of the injury, has been proven in the patient suffering from severe injury, although they are complemented with the assessment of other parameters. Considering all the previously exposed, this work tries to fulfill the following objectives:
- To collect a wide range of patients who have suffered severe head injury and study their epidemiological profile and clinical presentation.
- To verify the usefulness and efficacy of the GCS and Rimel Scale, in determining the severity and prognosis of cranial injury.
- To study the evolutionary patterns in severe cranial injury, according to the Jennett and Bond scale, and analyze the different variables that can act on them, determining which have greater significance and designing an initial and late prognostic prediction model.
MATERIALS AND METHODS
Inclusion criteria and classification of patients Getafe University Hospital is a center that serves a Reference population of 800,000 inhabitants, and traumas have been classified, following the Glasgow Coma Scale, in mild (patient that obtains 13-15 points), moderate (score from 9 to 12), and serious (score from 3 to 8). The chosen moment to apply the scale for the classification of them has been after 6 h after the trauma. In those cases in which the patient could not be assessed at 6 h (sedo relaxed or anesthetized patients), the best score obtained after non-surgical resuscitation measures were chosen. The variables analyzed in severe head injury are shown in Table 1.
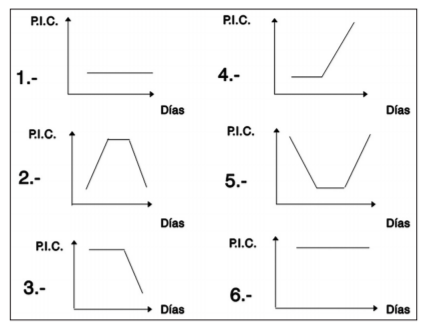
Patients admitted with severe injury were received directly in the ICU, where they underwent a clinical examination to check and normalize, when necessary, the hemodynamic and respiratory situation, and to discard the existence of associated extracranial lesions. The presence of these lesions can seriously compromise the cardiovascular or respiratory function, sometimes demanding an urgent action, which is carried out according to a previously systematized scheme in our center. When the patient's condition was stable, a general radiological study and brain CT were performed, usually without intravenous contrast administration. To define the pathological findings on CT, we have used our own classification. It should be noted that only a part of the patients could be classified on the basis of the initial CT, while other patients they have been based on the findings of the control CT. The ICP was monitored in all patients who showed focal lesion or diffuse swelling that made the development of intracranial hypertension probable. The patterns found in the evolution of the ICP are listed in Table 1. Each of these patterns (represented also in a Cartesian form) takes on significance in the retrospective or final study of each case, but in many patients, the pattern can be predetermined over the basis of the initial ICP and the type of lesion on CT, which can be very useful for designing therapeutic management. The ICP figures have been measured with an intraventricular catheter in the right frontal horn or intraparenchymal sensor, connected to monitors of the Philips type (Model P23D13), two-channel Hellige, and multi-channel Siemens or Camino. The calibration of the base pressure, in the case of the intraventricular technique, was performed against the atmospheric pressure taking as reference the Lundberg point, which corresponds to the roof of the frontal horn of the lateral ventricle. Within the general therapeutic measures, all associated metabolic or systemic problems and convulsive states were treated, although routine anticomicial therapy was not used, the coagulopathy was solved if it existed, a respiratory physiotherapy treatment and early rehabilitation were initiated, and provided an adequate nutritional supplement through parenteral nutrition. The management of focal lesions has followed the guidelines set out in the literature.
The first models were based on evidence based on the Bayes Theorem to calculate the evolution combining several factors, but these tests ignore the interdependence between them. Subsequently, the linear logistic regression was introduced, the most used currently, which assesses the influence of various variables on a previously established model, in general good or bad evolution, making possible the realization of a scale of prognostic factors, and through various mathematical models, a prognostic reliability index. Linear regression allows us to elaborate a classifying model of the various evolutionary indicators. The variables that have been shown to be most useful are, in a decreasing sense, the need for surgical decompression, age, physiological state at admission (presence of hypoxemia, hypercapnia or hypotension, and decreased hematocrit), motor response, and pupillary response. With these models prognostic reliability has been achieved between 30% and 90%, depending on whether they are used early or late, always considering falsely optimistic forecasts so as not to interfere in the possible therapeutic measures that could be applied to the patient. For the descriptive statistics, the most usual parameters have been used, such as means, percentages, standard deviations (s), proportions, and others. The final evolution of the patient with cranial injury has been determined at the time of hospital discharge. Within the chapter of analytical statistics, for the bivariate study we have used Chi-square tests, Spearman correlation coefficient, Student's "t," Wilcoxon tests for independent variables and Kruskal-Wallis, and Fisher's exact test. The limit of statistical significance has been established in a confidence interval of 95% (P < 0.05). The multivariate studies were performed using the linear regression method by maximum likelihood.
RESULTS
A total of 86 patients with severe head injury have been treated. Of these, 35 (40.7%) obtained a score of 8 or 7 (Group 1) on the Glasgow Coma Scale after applying non- surgical resuscitation measures, 25 (29.1%) obtained a score of 6 or 5 (Group 2), and 26 (30.2%) have a score of 4 or 3 (Group 3).
The results obtained in the different variables analyzed in the severe cranial injury are presented below. Age: Among the patients in Group 1, there are 24 (68.6%) under 35, 8 (22.8%) have between 35 and 65, and 3 (8.6%) are over 65 years old. In Group 2 patients, there are 20 (80%) under 35, 4 (16%) between 35 and 65, and 1 (4%) over 65 years. Among patients in Group 3, there are 11 (42.3%) under 35, 13 (50%) between 35 and 65, and 2 (7.7%) over 65 years. The average age is 33.9 years (s = 16.83), ranging in a range between 14 and 83 years. Sex: In Group 1, there are 27 men (77.1%) and 8 women (22.9%). In Group 2 there are 21 men (84%) and 4 women (16%). In Group 3 there are 21 men (80.8%) and 5 women (19.2%). Origin of the sick: 58.1% (50 patients) come directly from the accident site, and 41.9% (36 patients) are transferred from another hospital. Traumatism-income interval: The average delay between injury and hospital admission is 4.4 h (s = 6.73), ranging from 0.2 to 48 h. Causing mechanisms: In Group 1, there are 15 vehicle occupants (42.8%), 4 who suffer outrage (11.4%), 7 bicycle or motorcycle accident (20%), 8 fall (22.8%), and 1 direct impact (2.8%). Among the patients of Group 2, 13 are vehicle occupants (52%), 3 suffer from being run over (12%), 4 bicycle or motorcycle accident (16%), 3 fall (12%), 1 direct impact (4%), and in 1 case the cause is unknown (4%). Among the patients of Group 3, there are 9 vehicle occupants (34.6%), 1 suffering from being run over (3.8%), 8 bicycle or motorcycle accidents (30.8%), 4 falling (15.4%), 2 injuries by firearm (7.7%), and in 2 cases the cause is unknown (7.7%). Medical history: 82.6% of the patients have no known pathological history, 10 patients (11.6%) have a history of alcohol intake or drug use, 1 patient (1.2%) history of generalized seizures, and 4 patients (4, 6%) other antecedents.
Associated traumatic injuries: Among the patients in Group 1, there are 18 patients with associated injuries (51.4%), with 2 cases of spinal trauma (11.1%), 5 facial injury (27.7%), and 3 thoracic-abdominal traumas (16, 7%), 3 orthopedic injury (16.7%), and 5 traumas (27.7%). In Group 2, 11 patients have associated injuries (44%), with 3 cases of facial injury (27.3%), 3 thoracic-abdominal traumas (27.3%), 3 orthopedic injury (27.3%), and 2 multiple traumas (18.2%). Of the patients in Group 3, 18 had associated injuries (69.2%), with 1 case of spinal injury (5.5%), 2 facial injury (11.1%), and 4 thoracic-abdominal traumas (22.2%), 4 orthopedic traumas (22.2%), and 7 polytraumatisms (38.9%).
Clinical signs of cranial base fracture: In 17 patients (19.8%), there are clinical signs of cranial base fracture (rino or otolicuorragia, periorbital or retromastoid hematoma). Worst score on the Coma Glasgow Scale. In Group 1, 13 patients (37.1%) obtained a score of 6 or 5 on the Glasgow Coma Scale before establishing non-surgical resuscitation measures and 12 (34.3%) score of 4 or 3. In Group 2, 15 patients (60%) had a score of 4 or 3, before the application of the resuscitation measures. Presence of hypotension and hypoxemia: There are 21 patients (24.4%) who present hypotension (systolic blood pressure < 90 mmHg) and 13 (15.1%) who have hypoxemia (pO2 < 60 mmHg) at the time of admission. Presence of neurological focality: In Group 1, there are 16 patients (45.7%) with focal neurological examination, 12 (48%) in Group 2, and 20 patients (76.9%) in Group 3. Only 2 patients presented generalized seizures (2.3%). Pupillary size and reactivity: There are 34 patients (39.5%) with normal pupils, 10 (11.6%) that initially show normal pupils develop unilateral mydriasis, 3 (3.5%) that progress to bilateral mydriasis, 20 (23.2%) with unilateral initial mydriasis, and 19 (22.1%) with bilateral mydriasis from the beginning. 85% of mydriatic pupils are completely reactive.
Simple radiology: A simple skull radiograph was performed on 82 patients (95.3%), with a fracture detected in 49 (59.8%). The fracture is linear in 39 patients (79.6%) and sunk in 10 (20.4%). CT: The results obtained in the different variables analyzed in the initial CT are presented below. Type of injury among the patients in Group 1, there are 1 that shows normal CT (2.8%), 9 diffuse axonal injury (25.7%), 1 diffuse axonal lesion with associated swelling (2.8%), 9 diffuse cerebral swelling (25.7%), 2 pure epidural hematoma (5.7%), 3 epidural hematoma with associated swelling (8.6%), 3 pure subdural hematoma (8.6%), 5 subdural hematoma with associated swelling (14, 3%), 1 focal contusion (2.8%), and 1 bilateral multiple contusions (2.8%). In Group 2, there is 1 patient with normal CT (4%), 10 cases of diffuse axonal injury (40%), 6 cases of diffuse cerebral swelling (24%), 2 pure epidural hematomas (8%), 1 subdural hematoma with associated swelling (4%), 1 focal contusion (4%), 2 unilateral multiple contusions (8%), and 2 bilateral multiple contusions (8%). In Group 3, 6 cases of diffuse axonal injury (24%), 3 of diffuse axonal injury with associated swelling (12%), 11 of diffuse swelling (44%), 1 pure epidural hematoma (4%), 3 subdural hematomas with associated swelling (12%), and 1 unilateral multiple contusion (4%). Subarachnoid hemorrhage: In Group 1, there are 18 patients (51.4%) with subarachnoid hemorrhage, 14 (56%) in Group 2, and 16 patients (61.5%) in Group 3. In total, 55.8% of patients have subarachnoid hemorrhage. Intraventricular hemorrhage: In Group 1, there are 9 patients (25.7%) with intraventricular hemorrhage, 7 (28%) in Group 2, and 14 patients (53.8%) in Group 3. In total, 34.9% of the patients have an intraventricular hemorrhage. Pneumocephalus: In 17 patients (19.8%), the presence of air in the intracranial compartment was observed on CT.
Volume of injuries: The average volume is 27.1 cc. (s = 49.91), oscillating in a range between 0 and 270 cc. The volume is < 25 cc. in 59 patients (73.7%), between 25 and 50 cc. in 8 (10%), and >50 cc. in 13 patients (16.3%). Deviation of the middle line: The average deviation is 4.9 mm. (s = 6.93), oscillating in a range between 0 and 26 mm. The deviation of the midline is < 7 mm in 56 patients (70%), between 7 and15 mm in 13 (16.2%), and >15 mm in 11 patients (13.8%). Cisternal system: In Group 1, cranial base cisterns are normal in 14 patients (40%), compressed in 14 (40%), and absent in 7 patients (20%). In Group 2, mesencephalic cisterns are normal in 12 patients (48%) and are compressed in 13 (52%). In Group 3, they are normal in 5 patients (18.9%), appear compressed in 10 (40.5%), and absent in 10 patients (40.5%). Ventricular system: In Group 1, the ventricles are normal in 14 (40%) and are compressed in 21 (60%). In Group 2, they are normal in 12 (48%) and appear compressed in 13 (52%). In Group 3, they are normal in 5 (19.2%) and are shown compressed in 21 (80.8%). Medical treatment: Sedo relaxation is practiced in 86 patients (100%) and hyperventilation in 80 (93.1%). Treatment was established with Mannitol in 37 (43.1%) and with Thiopental in 22 (25.6%). Surgical treatment: In Group 1, 19 patients were not intervened (54.3%), fracture elevation was performed in 1 patient (5%), surgical debridement in 1 (5%), lobectomy in 3 (15%), decompressive surgery in 3 (15%), burr holes in 4 (20%), and evacuation of the lesion in 8 patients (40%). In Group 2, 15 patients were not operated on (60%), fracture elevation was performed in 3 patients (25%), lobectomy in 4 (33.3%), burr holes in 3 (25%), and evacuation of the injury in 2 (16.7%). In Group 3, 9 patients were not intervened (34.6%), lobectomy was performed in 4 (18.2%), decompressive surgery in 7 (31.8%), burr holes in 5 (22.7%), and evacuation of the lesion in 6 patients (27.3%). In 32 (80%) of the 40 patients operated on (46.5%), 1 intervention was performed, and in 8 (20%), 2 interventions were performed. The average score on the Glasgow Coma Scale at the time of surgery is 4.2 (s = 1.44), ranging from 3 to 8.
Monitoring the ICP: The ICP is monitored in 22 patients in Group 1 (62.8%), in 14 patients in Group 2 (56%), and in 13 patients in Group 3 (50%). In 38 (77.5%) of the 49 patients monitored (56.9%) intraventricular technique is practiced and in 11 (22.5%), intraparenchymal technique [Figure 1]. The average duration of monitoring is 7.8 days (s = 5.68), ranging from 1 to 23 days. The duration is < 7 days in 28 patients (57.1%), and is comprised between 7 and 14 days in 14 (28.6%), and is >14 days in 7 (14.3%). Initial ICP: In Group 1, the initial ICP is < 20 mmHg in 11 patients (50%) and >20 in 11 (50%). In Group 2, it is < 20 mmHg in 6 patients (42.8%) and >20 in 8 (57.1%). Among patients in Group 3, it is < 20 mmHg in 6 (46.1%) and < 20 in 7 patients (53.8%). Evolution of the ICP:. In Group 1, the ICP follows pattern 1 (low) in 6 patients (27.3%), pattern 2 (low/high/low) in 6 (27.3%), pattern 3 (high/low) in 4 (18.2%), pattern 4 (low/high) in 1 (4.5%), pattern 5 (high/ low/high) in 1 (4.5%), and pattern 6 (elevated) in 4 patients (18.2%). Among patients in Group 2, the ICP follows pattern 1 in 6 (46.1%), pattern 2 in 2 (15.4%), pattern 3 in 3 (23.1%), pattern 4 in 1 (7.6%), and pattern 6 in 1 patient (7.6%). In Group 3, the ICP follows pattern 1 in 4 (30.8%), pattern 2 in 2 (15.4%), pattern 3 in 3 (23.1%), pattern 4 in 2 (15.4%), and pattern 6 in 2 patients (15.4%). ICP more representative: In Group 1, the most representative ICP is < 20 mmHg in 8 patients (36.4%) and >20 in 14 (63.6%). In Group 2, the most representative ICP is < 20 mmHg in 7 patients (50%) and >20 in 7 (50%). In Group 3, the most representative ICP is < 20 mmHg in 5 patients (38.5%) and >20 in 8 patients (61.5%).
Clinicaldeteriorationoccursin18 patientsofGroup 1 (51.4%), in 3 of Group 2 (12%), and in 2 patients of Group 3 (7.7%). The cause of clinical deterioration in Group 1 is elevated ICP in 4 patients (22.2%), increased hematoma in 4 (22.2%), the appearance of new hematoma in 3 (16.7%), infection neurological in 1 (4.5%), and systemic causes in 6 (33.3%). In Group 2, the cause of the deterioration is the increase of hematoma in 2 (66.7%) and systemic problems in 1 (33.3%). Among patients in Group 3, the origin of the deterioration is increased hematoma in 1 (50%), and systemic causes in 1 (50%). The mean delay between injury and clinical deterioration is 23.4 h (s = 42.36), ranging from 1 to 192 h. The average score on the Glasgow Coma Scale at the time of deterioration is 4.1 (s = 1.41, range: 3-8). Findings on control CT: In Group 1, the control CT shows improvement in 8 patients (21.6%) and does not show variations in 4 (10.8%). Diffuse cerebral swelling appears in 7 (18.9%), epidural hematoma in 1 (2.7%), subdural hematoma in 1 (2.7%), focal contusion in 4 (10.8%), multiple contusions in 4 (10.8%), and other injuries (infarction, subarachnoid, or other hemorrhage) in 8 patients (21.6%). In Group 2, the control CT is better in 5 patients (20%) and does not show variations in 8 (32%). Diffuse cerebral swelling appears in 2 (8%), epidural hematoma in 1 (4%), focal contusion in 2 (8%), and multiple contusions in 7 patients (28%). In Group 3, the control CT improved in 3 patients (16.7%) and did not show variations in 2 (11.1%). Diffuse cerebral swelling appears in 3 (16.7%), epidural hematoma in 2 (11.1%), focal contusion in 2 (11.1%), multiple contusions in 3 (16.7%), and other lesions in 3 patients (16.7%). Control CT was performed in 76 patients, and there was worsening in 46 (60.5%). The control CT is performed on average at 2.1 days (s = 0.81), ranging in a range between 1 and 5 days. The average number of control CTs is 3.1 (s = 1.49), ranging from 1 to 7.
In Group 1, there is 1 patient who presents good recovery (2.8%), 9 who develop moderate disability (25.7%), 7 severe disability (20%), 4 persistent vegetative state (11.4%), and 14 who die (40%). In Group 2, 3 patients presented moderate disability (12%), 7 severe disability (28%), 4 persistent vegetative state (16%), and 11 died (44%). In Group 3, there is 1 patient with moderate disability (3.8%), 1 severe disability (3.8%), 5 persistent vegetative state (19.2%), and 19 who die (73.1%). Of the total number of patients who die, 10 (22.7%) do so within a few hours of their hospital admission. The average duration of the coma is 18.2 days (s = 18.24), ranging from 1 to 75 days. Among patients who survive, 15 have residual involvement of cranial nerves (35.7%), 26 have residual hemiparesis (61.9%), and 29 have personality alterations (69.1%). Chronology of the exitus: The death occurs in the 1st week in 26 patients (59%). Of these, it occurs on the 1st day in 10 (38.5%), in the 2nd in 7 (26.9%), in the 4th in 3 (11.5%), in the 5th in 2 (7.7%), and in the 7th in 4 (15.4%). The exitus takes place between days 7 and 14 in 11 patients (25%) and from day 14 in 7 (16%). Causes of the exitus: Among patients of Group 1, the exits are due to intracranial hypertension in 7 cases (22.6%), increase in hematoma in 2 (6.4%), diffuse cerebral swelling in 4 (12.9%), cerebral herniation in 3 (9.7%), cerebral infarction in 1 (3.2%), neurological infection in 1 (3.2%), systemic infection in 2 (6.4%), respiratory failure in 5 (16.1%), and systemic medical complications in 6 patients (19.3%). In Group 2, the exitus are secondary to intracranial hypertension in 2 patients (8.7%), increased hematoma in 1 (4.3%), diffuse cerebral swelling in 2 (8.7%), cerebral herniation in 2 (8.7%), cerebral infarction in 1 (4.3%), systemic infection in 2 (8.7%), respiratory failure in 4 (17.4%), systemic medical complications in 5 (21.7%), and systemic injury in 4 patients (17.4%). Among patients of Group 3, the exits are due to intracranial hypertension in 9 cases (23.1%), increased hematoma in 1 (2.6%), diffuse cerebral swelling in 4 (10.2%), cerebral herniation in 5 (12.8%), cerebral infarction in 3 (7.7%), systemic infection in 2 (5.1%), pulmonary insufficiency in 5 (12.8%), systemic medical complications in 3 (7, 7%), systemic surgical complications in 2 (5.1%), and systemic polytraumatism in 5 patients (12.8%).
A bivariate study of every one of the variables has been carried out, showing the most important results below. Age and the causative mechanisms correlate significantly (P < 0.001). Among those under 35 years of age, there are 28 vehicle occupants (53.8%), 2 who suffer outrage (3.8%), 16
bicycles or motorcycle accident (30.7%), 5 fall (9.6%), and 1 injury by firearm (1.9%). In the group of patients between 35 and 65 years old, there are 7 vehicle occupants (36.8%), 1 who suffers a bicycle or motorcycle accident (5.3%), 8 fall (42.1%), 2 impacts direct (10.5%), and 1 injury by firearm (5.3%). Among patients over 65 years of age, 3 suffer from being run over (60%) and 2 fall (40%). Age and CT findings are significantly related to each other (P < 0.001). Among patients younger than 35 years, there are 2 with normal CT (3.6%), 22 with diffuse axonal injury (39.3%), 2 with diffuse axonal injury and associated swelling (3.6%), 14 with diffuse swelling (25%), 7 with epidural hematoma (12.5%), 3 with subdural hematoma (5.3%), 1 with focal contusion (1.8%), 3 with unilateral multiple contusions (5.3%), and 2 with bilateral multiple contusions (3.6%). In the age group between 35 and 65 years, 2 patients have diffuse axonal injury (9.5%), 2 diffuse axonal injury with associated swelling (9.5%), 10 diffuse cerebral swelling (47.6%), 1 epidural hematoma (4.8%), 5 subdural hematoma (23.8%), and 1 bilateral multiple concussion (4.8%). Among patients older than 65 years, 1 presented diffuse axonal injury (16.7%), 4 epidural hematoma (66.7%), and 1 subdural hematoma (16.7%). Age is significantly related to the final evolution (P < 0.001). Among patients younger than 35 years old, there are 1 with good recovery (1.8%), 11 who develop moderate disability (20%), 13 severe disability (23.6%), 8 remain in a persistent vegetative state (14.5%), and 22 die (40%). In the group of patients between the ages of 35 and 65, 2 develop moderate disability (8%), 2 severe disability (8%), 5 remain in a persistent vegetative state (20%), and 16 die (64%). The 6 patients over 65 years of age die (100%).
The causative mechanisms and findings on CT are significantly correlated (P < 0.01). Among vehicle occupants there are 2 with normal CT (5.5%), 12 with diffuse axonal injury (33.3%), 1 with diffuse axonal injury and associated brain swelling (2.8%), 11 with diffuse cerebral swelling (30.5%), 5 with epidural hematoma (13.9%), 2 with subdural hematoma (5.5%), 1 with unilateral multiple contusion (2.8%), and 2 with multiple bilateral contusions (5.5 %). Of the patients who suffer traumas, 4 have diffuse axonal injury (50%), 1 epidural hematoma (12.5%), 2 subdural hematoma (25%), and 1 focal contusion (12.5%). Among patients suffering bicycle or motorcycle accident, 9 have diffuse axonal injury (47.4%), 1 diffuse axonal injury with associated brain swelling (5.3%), 8 diffuse cerebral swelling (42.1%), and 1 unilateral multiple contusion (5.3%). Of the patients who suffer a fall, 2 have diffuse axonal injury with associated swelling (13.3%), 3 diffuse cerebral swelling (20%), 2 epidural hematoma (13.3%), 5 subdural hematoma (33.3%), 1 focal contusion (6.7%), 1 unilateral multiple contusion (6.7%), and 1 bilateral multiple concussion (6.7%). Among patients affected by direct impact, 1 has diffuse cerebral swelling (50%) and 1 has subdural hematoma (50%). The mechanisms causing the trauma correlate significantly with evolution (P < 0.001). Of the vehicle occupants, 6 develop moderate disability (16.2%), 6 severe disability (16.2%), 10 remain in a persistent vegetative state (27.1%), and 15 die (40.5%). Of the patients who suffer a stroke, 1 develops moderate disability (12.5%), 2 remain in a persistent vegetative state (25%), and 5 dies (62.5%).
Among patients suffer bicycle or motorcycle accident, 1 case of good recovery (5.3%), 4 moderate disabilities (21.1%), 7 severe disabilities (36.8%), and 7 deaths (36.8%). Of the patients suffering fall, 2 develop moderate disability (13.3%), 2 severe disability (13.3%), 1 remains in a persistent vegetative state (6.7%), and 10 dies (66.7%). Among patients who suffer direct impact, 2 dies (100%), and 2 with firearm injuries also die (100%). The lesional volume, the deviation of the cerebral midline and the compression of the cisternal and ventricular systems are related to the most representative ICP figures (P < 0.05). The higher the volume of injury, deviation or compression, the higher the figures of more representative ICP. The findings in the initial CT correlate significantly with the findings in the control CT (P < 0.001). The 2 initially normal CT patients show normal controls (100%). Of the patients with initial diffuse axonal injury, 12 show unchanged controls (50%), diffuse cerebral swelling (4.2%), 2 epidural hematoma (8.4%), 3 multiple contusions (12, 6%), in 2 (8.4%), other lesions appear (infarction, subarachnoid hemorrhage, or others), and in 4 patients the control shows improvement (16.7%). Among patients with diffuse axonal injury and initial associated brain swelling, there is 1 control that shows improvement (100%). Of the patients with initial diffuse cerebral swelling, 7 did not show changes in controls (20.6%), 3 presented epidural hematoma (8.8%), 4 focal contusion (11.7%), 7 multiple contusions (20, 6%), 9 have other lesions (26.5%), and in 4 patients the control shows improvement (11.8%). Of the patients with initial epidural hematoma, in 1 the control shows important remains of the hematoma (11.1%), in 1 diffuse cerebral swelling (11.1%), in 1 focal contusion (11.1%), in 2 bruises multiple (22.2%), in 1 other lesions (11.1%), and in 3 patients the control showed improvement (33.3%). In patients with initial subdural hematoma, 1 control shows significant remains of the hematoma (6.7%), 2 diffuse cerebral swelling (13.3%), 1 focal contusion (6.7%), 4 multiple contusions (26.7%), 4 other injuries (26.3%), and in 3 the control shows improvement (20%).
Of the patients with initial focal contusion, 1 control shows an increase in its size (33.3%), 1 unilateral multiple contusions (33.3%), and 1 other lesions (33.3%). In the 2 patients with initial unilateral multiple contusion and who have control, no variations appear (100%). Of the patients with initial bilateral multiple contusion, 1 control showed associated brain swelling (20%), 3 showed an increase in the size of the contusions (60%), and 1 other lesions (20%). The presence of peritraumatic hypotension correlates significantly with evolution (P < 0.01). Among the patients who have hypotension at admission, 15 die (71.4%), 2 remain in a persistent vegetative state (9.5%), and 4 develop severe disability (19.1%). Of the patients without hypotension, 26 die (41.9%), 11 remain in a persistent vegetative state (17.7%), 11 develop severe disability (17.7%), 13 moderate disability (20.9%), and 1 presents good recovery (1.6%). The existence of hypoxemia is related to evolution (P < 0.01). Of the patients who have hypoxemia on admission, 9 die (69.2%), 2 remain in a persistent vegetative state (15.4%), and 2 develop moderate disability (15.4%). Among the patients without hypoxemia, 33 died (45.8%), 11 remain in a persistent vegetative state (15.7%), 15 develop severe disability (21.4%), 11 moderate disability (15.7%), and 1 presents good recovery (1.3%). The types of injuries in the initial CT are significantly related to the pattern of behavior of the ICP and evolution (P < 0.001). Of the patients with normal CT there are 2 who develop moderate disability (100%). Among those with diffuse axonal injury, 8 die (32%), 6 remain in a persistent vegetative state (24%), 7 develop severe disability (28%), 3 moderate disability (12%), and 1 have good recovery (4%). The 4 patients with diffuse axonal injury and associated brain swelling die (100%). Of the patients with diffuse cerebral swelling, 15 died (57.7%), 5 remain in a persistent vegetative state (19.2%), 4 develop severe disability (15.4%), and 2 moderate disability (7.7%).
Of the patients with epidural hematoma, 4 die (36.4%), 1 is left in a persistent vegetative state (9.1%), 3 develop severe disability (27.3%), and 3 moderate disability (27.3%). Among patients with subdural hematoma, 19 die (65.5%), 4 remain in a persistent vegetative state (13.8%), 2 develop severe disability (6.9%), and 4 moderate disability (13.8%). Of the patients with pure extra-axial hematoma, 6 developed moderate disability (85.7%) and 1 severe disability (14.3%). Among patients with focal contusion, 4 died (57.1%) and 3 remain in a persistent vegetative state (42.9%). Of the patients with unilateral multiple contusion, 4 die (66.7%), 1 remain in a persistent vegetative state (16.7%), and 1 develops severe disability (16.7%). All patients with bilateral multiple contusion die (100%). The presence of subarachnoid or intraventricular hemorrhage correlates significantly with evolution (P < 0.01). Of the patients with subarachnoid hemorrhage, 30 die (62.5%), 7 remain in a persistent vegetative state (14.6%), 8 develop severe disability (16.7%), and 3 moderate disability (6.3%). Of the patients without subarachnoid hemorrhage, 12 die (33.3%), 6 remain in a persistent vegetative state (16.7%), 7 develop severe disability (19.4%), 10 moderate disability (27.8%), and 1 has good recovery (2.8%). Among patients with intraventricular hemorrhage, 20 die (66.7%), 6 remain in a persistent vegetative state (20%), 3 develop severe disability (10%), and 1 moderate disability (3.3%). Of the patients without intraventricular hemorrhage, 22 die (40.7%), 7 remain in a persistent vegetative state (12.9%), 12 develop severe disability (22.2%), 12 moderate disability (22.2%), and 1 presents good recovery (1.8%).
The volume of lesions correlates significantly with evolution (P < 0.01). Of the patients with lesions smaller than 25 cc., 27 dies (46.5%), 10 remain in a persistent vegetative state (17.2%), 11 develop severe disability (18.9%), 9 moderate disability (15, 5%), and 1 has good recovery (1.7%). In the group of patients with lesions between 25 and 50 cc., 4 dies (44.4%), 2 remain in persistent vegetative state (22.2%), 1 develop severe disability (11.1%), and 2 moderate disability (22.2%). Of patients with lesions larger than 50 cc., 8 dies (61.5%), 1 remains in a persistent vegetative state (7.7%), 2 develop severe disability (15.4%), and 2 moderate disability (15, 4%). The deviation of the midline correlates significantly with evolution (P < 0.01). Among patients with deviation < 7 mm, 24 dies (42.8%), 10 remain in a persistent vegetative state (17.8%), 11 develop severe disability (19.6%), 10 moderate disability (17, 8%), and 1 has good recovery (1.8%). Of the patients with a deviation between 7 and 14 mm, 7 dies (53.8%), 2 remain in persistent vegetative state (15.4%), 3 develop severe disability (23.1%), and 1 moderate disability (7, 7%).
Of the patients with deviation >14 mm, 8 dies (72.7%), 1 remains in a persistent vegetative state (9.1%), and 2 develop moderate disability (18.2%), and ventricular is also related to evolution (P < 0.01). Of the patients with normal cisterns, 10 dies (31.2%), 7 remain in a persistent vegetative state (21.9%), 7 develop severe disability (21.9%), 7 moderate disability (21.9%), and 1 has good recovery (3.1%). Among patients with compressed cisterns, 22 dies (66.7%), 3 remain in a persistent vegetative state (9.1%), 4 develop severe disability (12.1%), and 4 moderate disability (12.1%). Of the patients with absent cisterns, 7 dies (43.7%), 3 remain in a persistent vegetative state (18.7%), 4 develop severe disability (25%), and 2 moderate disability (12.5%). Of the patients with normal ventricles, 9 dies (29.1%), 7 remain in a persistent vegetative state (22.6%), 7 develop severe disability (22.6%), 7 moderate disability (22.6%), and 1 presents good recovery (3.2%). Among patients with compressed ventricles, 30 dies (60%), 6 remain in a persistent vegetative state (12%), 8 develop severe disability (16%), and 6 moderate disability (12%). The need for barbiturate treatment is significantly related to evolution (P < 0.01). Of the patients requiring Thiopental, 11 dies (50%), 4 remain in a persistent vegetative state (18.2%), 5 develop severe disability (22.7%), and 2 moderate disability (9.1%). Of the patients who do not need it, 33 dies (51.6%), 9 remain in a persistent vegetative state (14.1%), 10 develop severe disability (15.6%), 11 moderate disability (17.5%), and 1 has good recovery (1.6%). The need for surgical treatment is related to evolution (P < 0.05).
The need for surgery leads to a worse prognosis. The worst score obtained by the patient in the GCS correlates with the evolution (P < 0.001), and the best score is also related (P < 0.01). The figures for initial ICP and evolution correlate significantly (P < 0.01). Of the patients with initial ICP < 20 mmHg, 10 die (43.5%), 4 remain in a persistent vegetative state (17.4%), 5 develop severe disability (21.7%), and 4 moderate disability (17, 4%). Among patients with initial ICP >20, 14 dies (56%), 5 remain in a persistent vegetative state (20%), 5 develop severe disability (20%), and 1 moderate disability (4%). The pattern of behavior of the ICP correlates with the final evolution (P < 0.001). Of the patients with pattern 1, 5 dies (31.2%), 4 remain in a persistent vegetative state (25%), 5 develop severe disability (31.2%), and 2 moderate disability (12.5%). In the group with pattern 2, 4 dies (40%), 1 remains in a persistent vegetative state (10%), 3 develop severe disability (30%), and 2 moderate disability (20%). In the group with pattern 3, 3 dies (30%), 4 remain in persistent vegetative state (40%), 2 develop severe disability (20%), and 1 moderate disability (10%). In the groups with paern 4, 5 and 6, all the patients die (100%). The most representative ICP figures are also related to evolution (P < 0.01). Of the patients with more representative ICP figures < 20 mmHg, 7 dies (35%), 4 remain in a persistent vegetative state (20%), 6 develop severe disability (30%), and 3 moderate disability (15%). Among the patients with more representative ICP figures >20 mmHg, 16 dies (61.5%), 5 remain in a persistent vegetative state (19.2%), 3 develop severe disability (11.5%), and 2 moderate disability (7.7%). Pupillary exploration is related to evolution (P < 0.001). The absence of reactivity leads to a worse prognosis.
Of the patients with normal pupils, 14 dies (41.8%), 3 remain in a persistent vegetative state (8.8%), 6 develop severe disability (17.6%), 10 moderate disability (29.4%), and 1 has good recovery (2.9%). Among patients with initially normal pupils who subsequently develop unilateral mydriasis, 2 dies (20%), 2 remain in a persistent vegetative state (20%), 4 develop severe disability (40%), and 2 moderate disability (20%). Of the patients with initially normal pupils and who later develop bilateral mydriasis, 2 dies (66.7%), and 1 remains in a persistent vegetative state (33.3%). Of the patients with initial unilateral mydriasis, 11 dies (55%), 6 remain in a persistent vegetative state (30%), 2 develop severe disability (10%), and 1 moderate disability (5%). Of the patients with bilateral mydriasis from the beginning, 12 dies (75%), 1 remains in a persistent vegetative state (6.2%), and 3 develop severe disability (18.7%). The duration of coma is related to evolution (P < 0.001). Among patients in whom the coma past < 8 days, 25 dies (83.3%), 4 develop moderate disability (13.3%), and 1 has good recovery (3.3%). Of which the duration comprises between 8 and 14 days, 9 dies (47.4%), 1 remains in a persistent vegetative state (5.3%), 4 develop severe disability (21.1%), and 5 moderate disability (26,3%).
Of which the duration is >14 days, 7 dies (20%), 13 remain in a persistent vegetative state (37.1%), 11 develop severe disability (31.4%), and 4 moderate disability (11.4%). The findings in control CT correlate with evolution (P < 0.001). Of the patients with normal control CT, 2 develop moderate disability (100%). Among the patients whose control does not show variations, 3 dies (21.4%), 5 remain in a persistent vegetative state (35.7%), 5 develop severe disability (35.7%),and 1 moderate disability (7.1%).
Of the patients whose control CT shows improvement, 5 dies (31.2%), 1 remain in a persistent vegetative state (6.2%), 4 develop severe disability (25%), 5 moderate disability (31.2%), and 1 has good recovery (6.2%). Among the patients in whose control CT diffuse cerebral swelling appears, 8 dies (66.6%), 1 remains in a persistent vegetative state (8.3%), 2 develop severe disability (16.7%), and 1 has moderate disability (8.3%). Of patients in whose control epidural hematoma appears, 1 remains in a persistent vegetative state (33.3%), 1 develops severe disability (33.3%), and 1 moderate disability (33.3%). In the patients in whose control subdural hematoma appears, 1 dies (100%). Of patients in whose control focal contusion appears, 1 dies (16.7%), 2 remain in a persistent vegetative state (33.3%), 2 develop severe disability (33.3%), and 1 moderate disability (16.7%). Of the patients in whose control multiple contusion appears, 8 dies (61.5%), 3 remain in a persistent vegetative state (23.1%), 1 develop severe disability (7.7%), and 1 moderate disability (7.7%). Among the patients in whose control other lesions appear (subarachnoid hemorrhage, cerebral infarction, or others), 2 dies (66.6%) and 1 remain in a persistent vegetative state (33.3%).
DISCUSSION
Recognizing that trauma is currently the main cause of death in people under 45 years of age and that 50-75% of accident deaths are due to head injury, has led to the acceptance that trauma cranial nerve represents a public health problem of the first magnitude. Efforts to reduce mortality have obviously focused on severe injury, where, despite new diagnostic techniques (CT and MRI) and monitoring of intracranial pressure, and advances in treatment, there has been no achieved a great decrease in morbidity and mortality rates, mainly due to the fact that the prognosis is closely linked to the brain damage that the patient already presents at the time of care (hence the enormous importance of the use of seat belts, air bags, and helmets, to reduce traumatic damage). At present, all patients with a score on the Glasgow Coma Scale of 8 or less tend to be included in the category of severe head trauma, after the application of non-surgical resuscitation measures, and those that deteriorate to that level score in the first 48 h immediately following the trauma. Therefore, a patient with cranial injury that is initially classified as mild or moderate, and that subsequently deteriorates, must strictly be included among the serious traumas, and its prognosis is similar to that of the latter [12]. Analyzing the serious cranial injury, this continues to predominate in children under 35 years of age, and again the proportion of males is higher than that described, in general, in the literature. The patients are transferred mainly in a mobile ICU, with good quality of care during the transfer, achieving a small delay between the injury and the hospital admission.
The incidence of hypotension and hypoxemia in our series is low, compared to the figures reported by other authors. The most frequent cause of severe cranial injury remains the traffic accident, with a significant proportion of associated systemic injuries, highlighting the low incidence of direct impacts due to aggression in our environment, compared to the data collected in other urban sectors, industrialized or less developed countries. Abuses and falls predominate in elderly patients. The CT findings have been systematized into nine pathological patterns that indicate the need to monitor the ICP and predict the behavior of the same. Diffuse cerebral or non-focal lesions are the most frequently observed (66.3% of diffuse lesions vs. 33.6% of focal lesions), with a significant proportion of cases presenting subarachnoid and/ or intraventricular hemorrhage. Although focal lesions tend to be more frequent in older patients, there is no distribution of pathological findings as clear as in patients with mild and moderate injury. At present, a new classification of serious injury has been described based on the information provided by the CT scan. The degree of compression of the mesencephalic cisterns, the deviation of the cerebral midline, and the presence or absence of focal masses is evaluated. The diffuse axonal lesion is divided into 4 groups, which are: (I) There is no pathology visible on CT, (II) pure diffuse axonal injury with patent cisterns, deviation of the midline < 5 mm, and/or focal lesions of volume < 25 cc, (III) diffuse axonal lesion plus swelling associated with compressed or absent cisterns, deviation of the midline < 5 mm and focal lesions of volume < 25 cc, and (IV) diffuse axonal lesion with associated swelling, deviation of the median line >5 mm and focal lesions of volume < 25 cc. There is a direct relationship between these four categories and the mortality rate. When used in conjunction with the rest of the CT patterns (extra- axial epi or subdural hematoma, contusions, or others), the prognostic reliability increases relative to the probability of developing intracranial hypertension with adverse evolution, and the therapeutic decision is facilitated [13].
The medical and surgical treatment has followed the global guidelines currently collected in the literature. The classification of the behavior of the ICP in 6 well-defined patterns is very useful at the time of deciding the establishment of a specific therapy and very guiding of the final prognosis of the patient. The values of initial ICP and most representatives ICP have less significance with respect to the final evolution of the patient, but represent correct indicators in the clinical and therapeutic management. The incidence of worsening of the control CT is very high, which shows its importance when planning the treatment of the patient who suffers serious injury and confirms the severity of the traumatisms collected in our series. This is also verified by the high incidence of pupillary changes and the average of the worst score obtained by the patient in the Glasgow Coma Scale, which is 4.4. As has been demonstrated in previous publications and is evident in the present series, these two parameters considered in isolation have a remarkable prognostic and definitive value of the final evolution of the patient suffering from severe head injury.
The mortality of the serious cranial injury is high, although we must consider that 22% of the patients die in the first 24 h. In fact, due to the broad inclusion criteria of patients used in this study, all those with necessarily fatal injuries or whose chances of survival are very remote have been admitted. In the work of the "North American Data Bank" mortality of 36% is collected, ranging from 76% in patients with a score of 3 in the GCS and 18% in patients who obtain 8 or 7 points. Among patients with diffuse lesions (general mortality of 31%), the prognosis is worse in patients with diffuse axonal injury Types III and IV, according to the scheme discussed above. Among patients with focal lesions, mortality is 39%. As already mentioned in the introduction chapter, prognostic estimation during the acute phase of severe head injury is of great importance. In studies carried out during the past two decades, only clinical data easy to obtain and applicable in any center were considered. In more recent works, other data or diagnostic and therapeutic parameters with more or less prognostic influence have been incorporated. Different authors have tried to develop a method to calculate the probability of a certain evolution occurring, describing the advantages and disadvantages of the various statistical techniques. However, the information provided in most of these studies,[14] although of undeniable value, is difficult to apply in practice when considering a specific patient. Therefore, it seems essential to establish a statistical method that is reliable and easy to apply. This method should use a group of really useful prognostic indicators that have little variability among different observers and will have to demonstrate real validity after being tested or applied to a wide range of patients [15].
To design a system like the one indicated, it is necessary first of all to purify the parameters or variables with true prognostic significance, since not all of them have a clearly significant influence on the final evolution. Among the findings collected in the initial CT, the collapse of the mesencephalic cisterns and the deviation of the midline, both radiological indices of transtentorial herniation, are associated with elevated ICP and poor final prognosis. Patients with normal or pathological CT, but without alterations of the cisterns or deviation of the midline, present normal or moderately elevated ICP and easily controllable and have a better final evolution. The prognostic value of the status of mesencephalic cisterns has been repeatedly indicated in several studies and has sometimes been the finding with the greatest value in predicting the final evolution [4,14]; in fact, some authors show that, with the exception of patients who do not brace or do not have any response after the initial resuscitation measures, the degree of collapse of the cisterns is revealed as the most decisive and independent prognostic factor in the 1st h after the injury, and conclude that if the cisterns appear collapsed or compressed in the first CT, the evolution tends to be much less favorable than if they are patent or show no distortion, especially in patients who score between 6 and 8 in the Glasgow Coma Scale. The results of our study are similar and confirm that the risk of death in patients with severe head injury is greater if there is a collapse of the mesencephalic cisterns. We also found that the pathology or type of lesion causing the cisternal collapse does not influence the aforementioned correlation. Likewise, we observed that the risk of elevation of ICP in patients with abnormal cisterns is three times higher than in patients with normal cisterns. In some publications, it has been pointed out that there is no significant correlation between the displacement of the cerebral midline and the levels of ICP [16].
However, we have found that the deviation of the midline in the CT is an indicator of elevation of the ICP and that there is an important correlation between the degree of displacement and the final evolution, independently of the underlying pathology that causes said deviation. Ventricular asymmetry has been considered by some authors as an unreliable parameter to establish prognostic predictions. In our series, the decrease in ventricular size or its asymmetry is related to elevation of the ICP and worse prognosis, as occurred in other studies. This discrepancy may be due to the difficulty of adequately assessing the ventricular size and to the variations of the moment in which said estimation is carried out, which may refer to the initial CT after admission or to the subsequent control CT. In our series, it is proven that subarachnoid hemorrhage is associated with a worse final prognosis, even when it is not combined with intracranial hypertension. In this regard, it has been speculated whether the mechanism by which traumatic subarachnoid hemorrhage leads to a worse final prognosis is the same as that which operates in patients with aneurysmal rupture [17]. The incidence of vasospasm in severe cranial injury ranges from 5% to 30% in different studies. In studies based on transcranial Doppler examination to determine the presence of vasospasm, an incidence close to 40% is recorded, being observed that it occurs mainly in patients with a large accumulation of blood in the basal cisterns. The authors consider that the incidence of vasospasm in traumatic and aneurysmal subarachnoid hemorrhage is superimposable, suggesting that the pathophysiology of the same is similar in both pathological circumstances.
Other CT data, such as the presence of intraventricular hemorrhage or large volume in the case of focal lesions, are also associated with a worse prognosis in the final evolution. The grouping of patients based on the nine patterns of intracranial lesion collected in the CT has undoubted prognostic significance. The patterns with worse evolution are diffuse axonal injury associated with brain swelling and bilateral multiple contusions. The poor prognosis in patients with multiple unilateral or bilateral contusions is linked to the development of medically intractable intracranial hypertension. In the case of extra-axial hematomas, the CT immediately after the surgery of the hematoma is the parameter that best indicates the possible uncontrollable elevation of the ICP and the fatal prognosis. The type of hematoma has been described as a predisposing factor to the appearance of associated brain swelling, which is more frequent in subdural hematomas than in epidural hematomas. The interval between the establishment of the coma and the moment of the evacuation surgery is also a clear factor that influences the development of this complication. Early surgery seems to be the only means to prevent the development of associated brain swelling, which is triggered when the intensity and duration of the compressive effect exerted by the hematoma on the underlying cerebral hemisphere exceed a critical level, causing diffuse ischemia and acute edema of the brain tissue. The lesion with the best prognosis is the pure extra- cerebral hematoma. The favorable evolution is easy to predict in those patients operated on an extra-axial hematoma who do not develop associated pathology after surgical evacuation. In them, post-operative ICP is low, as in most patients with contusion, managed medically, or surgically.
The prognosis of diffuse axonal injury without associated brain swelling is at an intermediate level. These patients do not present a lucid interval, which indicates that the lesion occurs at the moment of impact, and may show pupillary changes without there being herniation of the temporal lobe at the tentorial level. When no mass-occupying mass effect occurs, this lesion does not present with an elevation of the ICP, despite which many of these patients remain in a prolonged coma, subsequently developing a severe disability or remaining in a persistent vegetative state. Among the epidemiological variables, age is a very influential factor in the evolution of the patient with severe head trauma. In our study, as in others published in the literature, advanced age is associated with a progressive increase in mortality figures. In this sense, it should be noted that mortality in older patients is also related, or is due in part, to the higher incidence of medical complications in this subgroup.
Another clinical fact ofgreatprognosticimportance, especially when considered in relation to the type of intracranial lesion, is pupillary size and reactivity [18]. The presence of one or bilateral mydriasis decisively worsens the prognosis. Among the clinical parameters, the alteration of the oculocephalic and oculovestibular reflexes, which reflects the presence of a mesencephalic lesion, has been indicated in several studies as the best index of poor evolution. However, the validity of this parameter is pending confirmation. We have not valued the prognostic utility of these reflexes because we consider, like other authors, that they can be easily seen by the use of pharmacological therapy, as well as by the subjectivity of the researcher. The score obtained by the patient in the Glasgow Coma Scale is related to the final prognosis, with the worst score being the most decisive. Of the clinical parameters that are assessed in the Glasgow Coma Scale, the most useful and representative to estimate the severity of the injury is the motor response. The mechanism causing the serious injury has been revealed as a factor that conditions the final evolution, although this is not always admitted in the different published works. In our study, falls, direct impacts, and firearm injuries lead to worse evolution, and within the group of patients who suffer a traffic accident, those with associated systemic lesions have a higher incidence of peritraumatic hypotension and hypoxemia, with significantly higher mortality. The pattern of behavior of the ICP is of great influence on the final result. Patterns 4 (low/high), 5 (high/low/high), and 6 (high) are associated with 100% mortality. The uncontrolled elevation of the ICP is the most frequent cause of death.
The prognostic value of this variable is modified according to the moment in which it is considered, and thus the pattern of behavior over successive days is more decisive than the initial figures, although these help outline the therapeutic management and guide the prognostic prediction, in the patient suffering from severe head trauma. The need for barbiturate treatment is associated with a less favorable evolution. This is logically related to the patterns of behavior of the ICP, being necessary therapy with thiopental in those cases with high ICP figures that cannot be managed medically with other measures. The need for decompressive surgery is related to adverse prognosis. It is necessary to consider that this is practiced fundamentally in patients with ICP of difficult control, and who present TC patterns that condition bad prognosis by themselves. In the multivariate study, the pattern of behavior of the ICP, age, pupillary examination, the worst score on the Glasgow Coma Scale, the type of lesions on the control CT, the lesions on the initial CT, and the best score in the Glasgow Coma Scale are the parameters that, in this order, have been more influential in the final evolution of the patient with severe head injury. In the different works collected in the literature, the prognostic reliability of multivariable models ranges between 30% and 45% if applied on the 1st day, between 53% and 61% if used between the 2nd and 3rd days, and between 53% and 90% if applied between the 4th and 7th days.
Considering, on the one hand, that most deaths occur during the 1st week and that as the duration of coma increases, the proportion of patients who remain in a persistent vegetative state or who develop severe disability increases, it is easy to understand importance of prognostic estimates in the early stages of evolution [19]. The number of patients included in our series of severe cranial injury is low, so few parameters acquire significance in multivariable studies and the reliability is not very high. It is expected that as the number of patients increases, new parameters appear in the multivariable models and their reliability increases. In addition, and due to the great prognostic capacity of the patterns collected in the CT, the fact of elaborating models similar to the one described for each of the groups in which the patients can be classified according to these patterns, will increase the reliability even more.
CONCLUSIONS
- Severe head injury is more frequent in males than in females (4/1), predominantly in patients under 35 years of age. The most frequent causative mechanism is also the traffic accident (43.1%), followed by the accident of bicycle or motorcycle (22.1%), the fall (17.4%), the outrage (9.3%), the direct impact (2.3%), and the injury by firearm (2.3%).
- Lesions in severe head injury can be categorized into nine pathological patterns according to the information provided by the CT. These patterns have a well- defined anatomical and clinical profile and prognostic significance, in turn, associated with a pattern of behavior of the characteristic CIP. Pure extra-axial hematomas are the lesions that present the best prognosis, being the diffuse axonal lesion associated with brain swelling and multiple bilateral contusions which lead to worse evolution.
- The most influential parameters in the final evolution, according to the Bond scale, of the patient with severe head injury are, in this order, the type of behavior pattern of the ICP, age, size, and pupillary reactivity, the worst score obtained by the patient in the Glasgow Coma Scale, the findings in the initial and control CT, and the best score obtained by the patient in the Glasgow Coma Scale.
- The GCS correctly adjusts to the severity of head injury. The GCS is well related to the final prognosis of the patient suffering from a severe head injury.
REFERENCES
- Boye ND, Mattace-Raso FU, Van der Velde N, Van Lieshout EM, De Vries OJ, Hartholt KA, et al. Circumstances leading to injurious falls in older men and women in the Netherlands. Injury 2014;45:1224-30.
- van Hensbroek P, Mulder S, Luitse JS, van Ooijen MR, Goslings JC. Staircase falls: High-risk groups and injury characteristics in 464 patients. Injury 2009;40:884-9.
- Ragg M, Hwang S, Steinhart B. Analysis of serious injuries caused by stairway falls. Emerg Med 2000;12:45-9.
- Friedland D, Brunton I, Potts J. Falls and traumatic brain injury in adults under the age of sixty. J Community Health 2014;39:148-50.
- Albrecht-Anoschenko J, Uhl E, Gilsbach JM, Kreitschmann- Andermahr I, Rohde V. Head injury after a fall on stairs: Poorer prognosis in inebriated patients? Zentralbl Neurochir 2005;66:59-62.
- Spaniolas K, Cheng JD, Gestring ML, Sangosanya A, Stassen NA, Bankey PE, et al. Ground level falls are associated with significant mortality in elderly patients. J Trauma 2010;69:821-5.
- Honkanen R, Smith GS. Impact of acute alcohol intoxication on the severity of injury: A cause-specific analysis of non-fatal trauma. Injury 1990;21:353-7.
- Available from: http//www.aaam.org/abbreviated-injury-scale- ais. [Last accessed on 2017 Jun 25].
- Baker SP, O'Neill B, Haddon W Jr. Long WB. The injury severity score: A method for describing patients with multiple injuries and evaluating emergency care. J Trauma 1974;14:187-96.
- Johnston JJ, McGovern SJ. Alcohol related falls: An interesting pattern of injuries. Emerg Med J 2004;21:185-8.
- Sterling DA, O'Connor JA, Bonadies J. Geriatric falls: Injury severity is high and disproportionate to mechanism. J Trauma 2001;50:116-9.
- Aitken LM, Burmeister E, Lang J, Lang J, Chaboyer W, Richmond TS. Characteristics and outcomes of injured older adults after hospital admission. J Am Geriatr Soc 2010;58:442-9.
- Yeung JH, Chang AL, Ho W, So FL, Graham CA, Cheng B, et al. High risk trauma in older adults in Hong Kong: A multicentre study. Injury 2008;39:1034-41.
- Kehoe AD, Smith JE, Lecky F, Yates D. Presenting GCS in elderly patients with isolated traumatic brain injury is higher than in younger adults. Emerg Med J 2014;31:775-7.
- Irwin ZN, Arthur M, Mullins RJ, Hart RA. Variations in injury patterns, treatment, and outcome for spinal fracture and paralysis in adult versus geriatric patients. Spine Phila Pa 1976 2004;29:796-802.
- Hsiao KH, Dinh MM, McNamara KP, Bein KJ, Roncal S, Saade C, et al. Whole-body computed tomography in the initial assessment of trauma patients: Is there optimal criteria for patient selection? Emerg Med Australas 2013;25:182-91.
- DaviesRM,ScrimshireAB,SweetmanL,AndertonMJ,HoltEM. A decision tool for whole-body CT in major trauma that safely reduces unnecessary scanning and associated radiation risks: An initial exploratory analysis. Injury 2016;47:43-9.
- Brown JB, Gestring ML, Forsythe RM, Stassen NA, Billiar TR, Peitzman AB, et al. Systolic blood pressure criteria in the national trauma triage protocol for geriatric trauma: 110 is the new 90. J Trauma Acute Care Surg 2015;78:352-9.
- Malhotra S, Kasturi K, Abdelhak N, Paladino L, Sinert R. The accuracy of the olfactory sense in detecting alcohol intoxication in trauma patients. Emerg Med J 2013;30:923-5.