Fetal Transverse Cerebellar Diameter: Our Experience
Juan Piazze1, Francesco Recchia2, Valerio D'Orazi3, Michele Rosselli4, Massimo Bratta5, Silvio Rea6
2.Department of Oncology, Ospedale Civile di Avezzano, Fondazione "Carlo Ferri", Monterotondo, Rome, Italy,
3.Department of General Microsurgery and Hand Surgery, "Fabia Mater" Hospital, Rome, Italy,
4.Unita Operativa di Oncologia, Ospedale Civile di Frascati, Rome, Italy,
5.Department of Oncology, Ospedale Civile di Rieti, Rome, Italy,
6.Department of Oncology, Chirurgia Oncologica, Universita degli Studi de L'Aquila, Dpt DISCAB, Fondazione "Carlo Ferri", Monterotondo, Rome
Citation : Piazze J, Recchia F, D'Orazi V, Rosselli M, Bratta M, Rea S. Fetal Transverse Cerebellar Diameter: Our Experience. Clin Res Obstetr Gynecol 2018;1(1):1-2.
We have been studying the transcerebellar diameter (TCD) to test its significance in the accurate correlation with gestational age (GA) and how this measurement may help in the management of intrauterine growth-restricted fetuses (IUGRs) and other pregnancy complications.
Cerebral growth has been shown to be reasonably linear from the first trimester to term pregnancies, regarding a comparison with other fetal measurement parameters widely used (biparietal diameter [BPD], head circumference [HC], femur length [FL], and abdominal circumference [AC]), it has no limitations such as BPD and HC in case of molding of fetal head in the third trimester or a not circular profile of AC as the third trimester goes ahead. Other important fact it is the evaluation of the known belief that TCD seems to not to be affected by IUGR. Predictive accuracy of TCD for GA estimation has been used in country scales due to its stronger predictive accuracy for GA compared to other fetal biometric parameters[1]. Complex studies have been performed regarding region-specific growth restriction of the brain following preterm birth[2]. Regional brain sizes in very preterm infants at term-equivalent age differ from those of term-born peers, which have been linked with later cognitive impairments. The callosal thickness and the TCD showed predominant dependence on age at birth over age evaluated by magnetic resonance imaging, suggesting that brain growth after preterm birth was considerably restricted or even became negligible compared with that in utero. In a recent research, the validity of TCD in fetal biometric has been tested in a pilot study. TCD was compared with other existing parameters in evaluating GA in 15-40 weeks gestation pregnancies. In the 29-40 weeks gestation group, TCD revealed the highest correlation with the second more accurate correlation seen for the FL values[3].
We would like to underline in this letter some interesting findings found regarding the TCD evaluation. First of all, we observed that from 18 to 22 weeks gestation the value of TCD in mm almost "corresponded" to the actual GA. It may seem funny; however, it may reveal helpful.
A pregnant woman within the refuge program of one charity association, for whom an obstetrical evaluation was asked. No documents available, French speaking, did not know her age and obviously no idea about the last menses of her present pregnancy. No other information other than "pregnant". The ultrasound evaluation offered a discordant high BPD regarding AC and FL values, TCD was 22.7 mm [Figure 1].
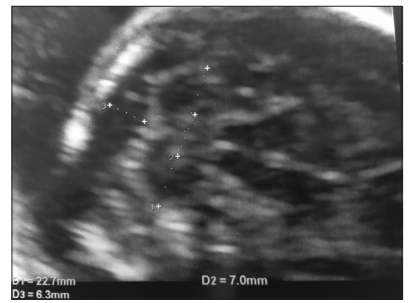
Given the circumstances, we decided to take the TCD as a reliable parameter and considered her pregnancy at 22 weeks gestation. Follow-up was uneventful, with no signs of hydrocephaly related to the higher BPD of the first examination. She gave birth to a healthy baby boy, weighing 3850 g at 40 weeks + 3 days gestation (as stated by first TCD for GA calculation).
An obese 21-year-old pregnant woman presented a fetal TCD of 17.3 mm at structural midgestation 22 weeks evaluation, with no other fetal biometry alteration. A late amniocentesis was performed to discard genetic anomalies, which reported a healthy 46,XY fetus. She was followed by endocrinological other than gynecological staff. This decreased TCD trend was kept and evaluated at 24, 28, 32, and 36 weeks gestation. She gave birth to a healthy 3940 g boy at 38 weeks gestation. Cerebellar development is particularly susceptible to exposure during the prenatal period, including maternal folate status, smoking habit, and alcohol consumption. Koning et al. have shown a prenatal cerebellar growth impairment in higher pre-pregnancy BMI women, which may lead to a detrimental impact on neurodevelopmental health of offspring in later life[4].
A 42-year-old pregnant woman with a trisomy 21 fetus diagnosed by amniocentesis at 18 weeks gestation, arrived for midgestation structural ultrasound evaluation at 21 + 3 weeks gestation. Cerebral hypoplasia was observed (TCD 15.3 mm, < 5th centile for GA). Moreover, TCD trend kept low until birth. This case particularly confirms the utility of TCD as a marker of trisomy 21. The combination of TCD and frontothalamic distance has been demonstrated to be superior to either measurement alone as a marker of Down syndrome[5].
Our research continues regarding TCD validity and the usefulness of this parameter regarding, especially cases with a late growth retardation in pregnancy.
REFERENCES
- Adyekun AA, Orji MO. Predictive accuracy of transcerebelar diameter in comparison with other fo eta biometric parameters for gestational age estimation among pregnant Nigerian women. East Afr Med J 2014;91:138-44.
- Iwata S, Katayama R, Kinoshita M, Saikusa M, Araki Y, Takashimaa S, et al. Region specific growth restriction of brain following preterm birth. Sci Rep 2016;23:33995.
- Redde RH, Prashanth K, Ajit M. Significance of foetal transcerebellar diameter in foetal biometry: A pilot study. J Clin Diagn Res 2017;11:TC01-4.
- Koning IV, Dudink J, Gronenberg IA, Willemsen SP, Reiss IK, Steegers-Theunissen RP. Prenatal cerebellar growth trajetories and the impact of periconceptional maternal and fetal factors. Hum Reprod 2017;32:1230-7.
- Winter TC, Ostrovsky AA, Komarniski CA, Uhrich SB. Cerebellar and frontal lobe hypoplasia in fetuses with trisomy 21: Usefulness ad combiined marker S. Radiology 2000;214:533-8.