Survey of School for the Blind and Community-based Rehabilitation Program on Childhood Blindness in the States of Meghalaya
Valensha Surong1, S. P. Saikia2, D. Patel3, Ferdinand Rapthap4
2.Mission Nethralaya, Shillong, Meghalaya, India,
3.ICEH, London,
4.Master of Clinical Optometry, Consultant Optometrist at Mission Nethralaya Shillong, Meghalaya, India
Citation : Surong V, Saikia SP, Patel D, Rapthap F. Survey of School for the Blind and Community-based Rehabilitation CBR Program on Childhood Blindness in the States of Meghalaya. Clin Res Ophthalmol 2018;1(2):1-15.
Childhood blindness is considered as one of the most important disability and burden in child life in terms of high number of blind years. The aim of the study is to determine the cause of severe visual impairment (SVI) and blindness among children in the states of Meghalaya to develop appropriate eye care services. No previous data exist for this region of India.
The study was conducted over 4 weeks. Data were collected from the only two integrated schools for the blind in Meghalaya. In addition, data from the districts of Jaintias hills and West Khasi hills were obtained from the community-based rehabilitation (CBR) program from the community. Examination of all the blind/SVI children (< 16 years of age) was done in both the school for the blind and in the community. Findings were recorded on a questionnaire modified from World Health Organization childhood blindness records form.
A total of 87 children from the school for the blind and 35 children through the CBR program in the community with visual disability were examined. Around 89.65% were blind and 9.20% were SVI from the blind school and 77.15% were blind and 11.42% are SVI from the community. No significant differences between male and female were found. The major anatomical site causing blindness among all the children in the blind school was corneal cause of blindness 54.02%, lens related 6.90%, whole globe 13.80%, and in the community corneal cause 34.28% followed by lens related 25.72% and glaucoma/buphthalmos 17%. These differences were not statistically significant between the two settings. Majority of the etiology cause was largely unknown although childhood factor contributes the main cause of blindness/SVI in the community 34.28% and the blind schools is 51.72%. The estimated prevalence extrapolated from the data in the community was 1.2/1000 children in this tribal population.
In this study, we saw blindness/SVI could be of an avoidable cause, in majority of child's life. These findings reflect the importance of primary prevention, for example, high measles immunization coverage, Vitamin A supplement, health and nutrition education, and continued support of the programs for control of Vitamin A deficiency through reproductive and child health programs. There is an urgent need to strengthen pediatrics eye care delivery services and surgical management for cataract and glaucoma. The used of CBR program in detecting the blind children in the community was found to be useful and has the potential of recruiting more numbers of children's with visual disability and also to provides rehabilitation services. The barriers face by the community in accepting eye care services can also be addressed through a strong link through the CBR program.
SVI- Severe visual impairment, CBR- Community based rehabilitation, U5MR- Under five mortality, VAD-Vitamin A deficiency,Ophthalmology,asclepiusopen
INTRODUCTION
In recent years, childhood blindness has been given priority due to the high magnitude of childhood blindness, particularly prevailing in developing countries and the high number of blind years, resulting from childhood blindness. The problems faced by the child, the burden on their families, the society, and the impact on the nation have to be considered[1] most of the blindness in childhood is either avoidable or preventable and many causes of childhood blindness are associated with increased child mortality[2].
An estimate for global blindness is 37 million, of which 1.5 million are children and almost three-quarters of them live in developing countries[3]. The prevalence of blindness in children ranges from approximately 0.3/1000 children in affluent regions to 1.5/1000 in the poorest communities[4]. Even with low prevalence of childhood blindness, it is given high priority under the Vision 2020 Right to Sight program for elimination of blindness.
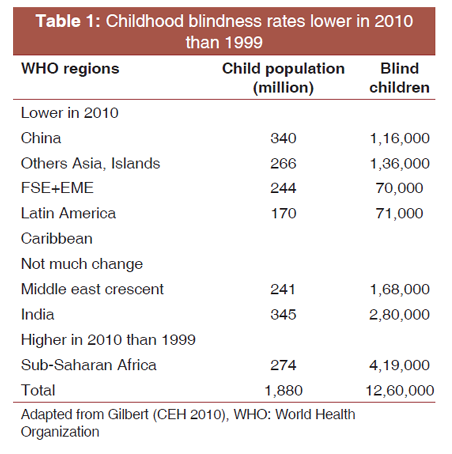
Worldwide, Vitamin A deficiency (VAD) and measles related blindness in children are showing signs of decline, this because of to better measles immunization coverage and Vitamin A supplementation but is still persisting in focal settings in developing countries[5,6]. According to Gilbert and Chandna the revised 2010 estimates, it has been observed that the number of children who are blind worldwide has declined 10% to 1.26 million over last 10 years and this change is seen in China and others Asian countries including the Philippines, Indonesia and Bangladesh were under-five mortality (U5MR) rate and prevalence of blindness has declined in contrast to Sub-Africa where the child population has increased and U5MR is increasing because of HIV epidemic [Table 1][7].
The major cause of blindness in children 0-15 years of age is different from one region to another region. In well-developed countries, the main cause of blindness is due to the higher visual pathway while corneal scarring from VAD, measles, and traditional medicine and cataract is found in poor and low-income countries[2,8,9]. Retinopathy of prematurity is a major contributing cause of blindness in middle-income countries as health services are improving and preterm survival rates go up[9]. Moreover, blindness in children is found to be more prevalent in poor regions as they are more exposed to the various risk factor and there are few well-equipped eye department and scarcity of human resources to deal and managed[10]. The World Health Organization (WHO) adopted a classification system on childhood blindness both on anatomical and etiological categories to focus intervention on those condition that is preventable, treatable, and conditions that need rehabilitation services[11,12].
UNICEF defines childhood as 0-16 years inclusive. The WHO defines blindness as a corrected visual acuity in the better eye of < 3/60 and severe visual impairment as corrected visual acuity in the better eye of < 6/60 but equal to or better than 3/60. Presenting vision < 6/60 has been used to defined blindness in Indian context[13].
For effective planning and designing of program, informative data on childhood blindness are crucial. There are different For effective planning and designing of program, informative data on childhood blindness are crucial. There are different.
This is one of the most accurate methods of assessing the prevalence of childhood blindness, but population-based data are difficult to obtain as register of the blind do not exist in developing countries, and besides large sample sizes are required to get the desired results[14].
Examination of children in special institution is also being carried to provide data on causes of blindness in children, but this method has its own selection bias as school for the blind cater only a proportion of the children, while the children who have other disabilities, pre-school, and poor children from rural areas who do not have access to school are not covered. The advantages in this methods are that a large number of children can be examined in a very short time by a single researcher.
Is another source to obtain data on childhood blindness but it lacks reliability.
This is also another alternative method to obtain information on a number of blind children results in given district (population-based assessment of childhood blindness done in South India, Southwest Uganda)[14,15] this way a rough estimate on the prevalence of blindness can be obtained in developing countries. The advantage in this methods survey has been done already by the CBR program and is cheaper but the demerits are the information used to obtain data might not be accurate.
This is another reliable method adopted in developing countries to collect information on childhood blindness in communities because it uses volunteers who know their own communities and has gain popularity in recent years and has been applied in countries such as Asia and Africa[16]. The disadvantages in this method are it needs large numbers of key informant who needs to be adequately trained, motivated, and committed to their work.
Childhood blindness is one of the major components for the elimination of blindness in the context of vision 2020[9]. The needs of the blind child and severely visual impaired differ both in treatment and diagnosis this poses a great challenge in the management of childhood blindness. Since in most of the developing countries, for example, India, pediatric ophthalmology is not yet well established as a subspecialty[17].
The main priorities for action are elimination of Corneal scarring due to VAD, measles, harmful traditional medicine and ophthalmia neonatorum, congenital cataract, childhood glaucoma, refractive error, and retinopathy of prematurity in children[9,18] all these conditions will be control or achieved through promotion of primary health care and providing separate pediatric eye care services and low vision services.
The population of India was estimated to be 1.03 billion (2001) approximately 420 million were children under 16 years of age (40.8%) and there is over 320,000 blind children which is a huge burden for the country[19]. The situation of childhood blindness as seen in India lies between the developed countries and developing countries of Asia and Africa[20].
To find out the cause of childhood blindness, a number of studies were carried out in various parts of India. All these studies show significant variation in the different regions of the country. A study in school for the blind in six schools for the blind in Andhra Pradesh, South India, found that the most common anatomical sites of severe visual impairment (SVI)/blindness were retina in 31.1%, cornea in 24.3%, and the whole globe in 20.2%. Hereditary factors contributing to 34.8% and childhood causes to 24% are the leading etiological causes[14,21] another study carried out in the same state which was done as a population-based study, shows that refractive error caused 33.3% of the blindness, followed by 8.3% due to VAD, congenital eye anomalies 16.7%, and retinal degeneration 16.7% [Image 2][9].
A study conducted in 9 states comprising around 1300 children in 1993 showed corneal scarring 26.4%, congenital anomalies of 20.7%, and retinal disease of 19.3%, respectively[22].
In the Northeastern states (NE) of India, studies in 12 schools for the blind reveal that the major anatomical causes of childhood blindness were congenital anomalies 36.1%, corneal condition 36.7%, cataract or aphakia 10.9%, retinal disorders 5.8%, and optic atrophy 5.3%[23]. Similarly, a study done in 13 schools for the blind in Delhi North, India, found that the anatomical sites of SVI/blindness were whole globe 27.4%, cornea 21.7%, retina 15.1%, and lens 10.9%[24].
A study conducted in Maharashtra, Western India, in 35 schools for the blind between 2002 and 2005 found out that the major causes of visual loss were congenital anomalies 41.3% corneal conditions 22%, cataract or aphakia 6%, and retinal disorders 11.2%[25].
Epidemiological data on blindness in children in India are incomplete but population-based studies have estimated as follows 0.65/1000 in children aged 0-15 years in urban and rural Andhra Pradesh,[14] 1.25/1000 in children aged 5-15 years in rural Andhra Pradesh,[26] and 0.53/1000 in children aged 5-15 years in Delhi[27]. These figures[27] are not directly comparable, as blindness has been defined differently in various studies and the samples are of different ages. Overall, the prevalence of childhood blindness in India is estimated to be 0.81/1000 children[26].
India is a rapidly developing nation, but improvement in health services is not uniform throughout the country. According to the various studies conducted, it is observed that in the poor socioeconomic states children were likely to be blind from corneal scarring which suggests that measles and VAD are the contributing factors. In the economically superior states, on the other hand, congenital anomalies and genetic diseases are major contributing factors toward childhood blindness.
Most of the cases of preventable blindness can be managed in the primary health-care level, but those requiring further management and treatment require expertise in pediatric ophthalmology in combination with a comprehensive approach and low vision center. Even though pediatric ophthalmology is being developed as a distinct specialty, the numbers are limited and require a total different set up for its management.
According to the study by Bhattacharjee and colleague[23] for the Blind school conducted in the four states of NE India. The findings showed that out of total 258 students examined corneal opacity accounted for 36.7%, followed by congenital anomalies 36.1% cataract or aphakia 10.9%, and retinal disorder 5.8% and nearly half of the children were blind from avoidable causes[23]. This study shows that corneal blindness was the most common cause of SVI and blindness and VAD and measles-related causes were contributing factors.
These findings suggest the importance of primary prevention through good coverage of Vitamin A prophylaxis, measles immunization, promotion of health, and nutrition education. However, there might be differences in the cause of blindness from the school for the blind when compared to those from the community. A data on childhood blindness from the community will be able to give a clearer picture of the cause of childhood blindness in the whole states, and this can be used for advocacy for better intervention and planning that is necessary for effective eye care services in the states.
This method has been utilized by several researchers to find the cause of blindness in children, a study done in India to find the prevalence of blindness in children aged 0-15 years in Andhra Pradesh was done through the community-based rehabilitation program as a part of comprehensive eye care[28,29].
The role of the CBR workers under this program is discussed below:
CBR workers should have knowledge of common eye diseases and the ability to detect suspected blind or visual impairment while they are doing house to house survey for detection of disability and rehabilitation services through a short training period.
They should be willing, motivated dedicated, cooperative, and committed to participate in the survey.
To should be able to carry out early identification intervention and appropriate referrals. Maintain a system of records and reports and to follow up and monitor the progress. The advantages of the CBR workers are that a lots of useful data can be obtained in a relatively short time saving money and time and linking eye care institutions to CBR partners and projects, as part of their outreach activities, to give a positive step toward a common goal to eliminate avoidable blindness and rehabilitate incurable blindness.
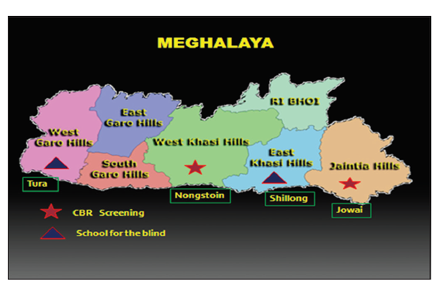
PREAMBLE TO MEGHALAYA - STATE PROFILE
The state of Meghalaya lies in the Northeastern part of India.
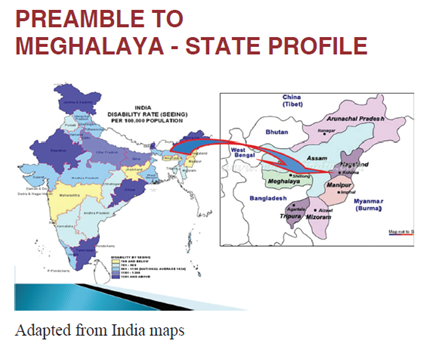
The total area of the state is 22,429 sq.km and has a population of 2.964.007 (2010) and has a density of 132/sq.km. Children under 16 years constitute around 40% of the population. The state comprises a Governor appointed from the center, the elected state chief ministers and his cabinets of ministers.
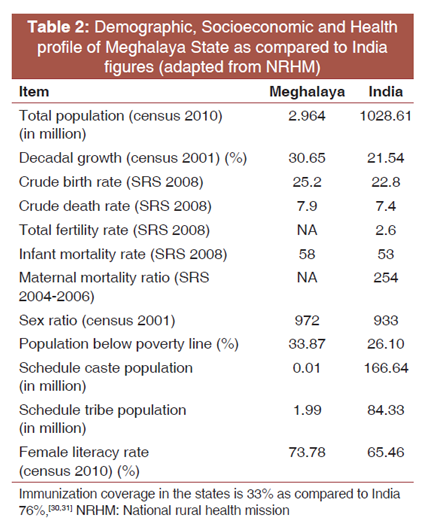
The Health and Family Welfare Department, Government of Meghalaya, is the Administrative Department. It is responsible for overseeing and cocoordinating the functions of the three directorates, that is, The Directorate of Health Services (MI), (Meghalaya Child Health and Family Welfare), (Research) so as to ensure uniform implementation of governmental procedures [Table 2].
Eye care in the states is provided mainly through government, private, and non-government organization (NGO).
Secondary eye care at the three districts is through government hospital in the states and two through NGO in the state capital.
Primary eye care is provided at the health center located in various sub-districts and sub-centers.
Some of the projects are sponsored by international NGP (INGOS) under Vision 2020: The Right to Sight programs. These INGOs includes Sight Savers International, Christian blended mission (CBM) and light for the world. Lions and Rotary have also been funding some of the eye care programs in the states. There are total 21 ophthalmologists in the government section, out of which 4 are operating ophthalmologist while in the private sector there are 6 operating ophthalmologists in the whole state of Meghalaya.
The pediatric ophthalmology services are available in Shillong, capital of Meghalaya, through a NGO hospital. One pediatric-oriented ophthalmologist is available along with other paramedical staff. Infrastructure for pediatric ophthalmology services in this hospital is developed with the support of Austria based INGO - "Light for the World." The pediatric ophthalmology services include pediatric cataract operation, glaucoma surgery, and partially functioning low vision services.
India has estimated 320,000 blind children, more than any other country in the world[18]. There is a need to take steps to identify the causes of childhood blindness and develop appropriate strategies to eliminate avoidable causes among them.
India is a vast country with socioeconomic, political, geographical, and ethnical diverse society in the 28 states and 7 Union territory of India. The seven NE states are geographically isolate from the rest of the country and are different in terms of culture, social, and economic development. The people who reside are predominantly of mongoloid race unlike the rest of Indian population. The topography is rugged; communication is difficult associated with political unrest as compared to other parts of the country. In Meghalaya, no study has been conducted on childhood blindness. Although Bhattacharya et al. had conducted a survey of blind schools of NE states in the year 2007-2008, Meghalaya was not included in that study due to some unmentioned limitation. In the absence of no recent data on childhood blindness, it is difficult to estimate the magnitude and causes of childhood blindness. Nearest study done in the other part of the blind school in NE India shows that corneal blindness is major cause of blindness in this region[17]. There is a need for developing services at all level for prevention and control of childhood blindness. Health and eye care services are available in limited areas (urban) which are not accessible to people living in remote tribal areas.
Recently, Government of India has taken special initiatives to improve the health-care services including the eye care services including childhood blindness in entire Northeast states,[18] but there has been no evidence of magnitude and causes of childhood blindness in the Meghalaya state. The primary objectives of the present study are to determine the causes of blindness in children in schools for the blind in Meghalaya to utilize the findings for the planning of appropriate preventive, curative, and rehabilitation service.
AIMS AND OBJECTIVES
The aim of the study was to determine the causes of SVI and blindness among children in the state of Meghalaya to develop appropriate eye care services.
The objectives are as follows:
1. To estimate the magnitude of childhood blindness and SVI among children of < 16 years in the schools for the blind and children identified by the CBR screening in two districts of Meghalaya.
2. To determine the main causes of childhood blindness among the children in blind schools and CBR program.
3. To estimate and compare the magnitude of preventable and treatable causes of childhood blindness in schools for the blind and CBR program in urban and rural areas.
4. To document the challenges faced by CBR programmed to refer and in providing services to the blind and severely impaired children.
5. To recommend the priorities for prevention and control of blindness in children.
MATERIALS AND METHODS
The study was a cross-sectional study carried out in the two schools for the blind in Meghalaya and also children from the CBR programs that cover two districts of Meghalaya to find blind children in the communities.
The study was done in two schools for the blind of Meghalaya situated in East Khasi Hills and Tura districts in the state of Meghalaya in the Northeastern part of India. The two blind schools included in the study are.
a. Bethany school for the blind in Shillong, East Khasi Hill district (Jyoti Shroat)
b. Montfort school for the blind in Tura district.
Besides this, the two rehabilitation projects running in these districts are also included for the study.
All the children < 16 years of age studying in these two schools for the blind and all the children identified by CBR program with presenting visual acuity in the better eye of < 6/60 were included in the study.
Children above the age of 16 years at the time of study and those whose presenting vision was >6/60 in the better eye were excluded.
The study includes all the available blind children in two blind schools and in the rehabilitation projects in two districts of Meghalaya who fulfilled the inclusion criteria(preliminary numbers approximately 250).
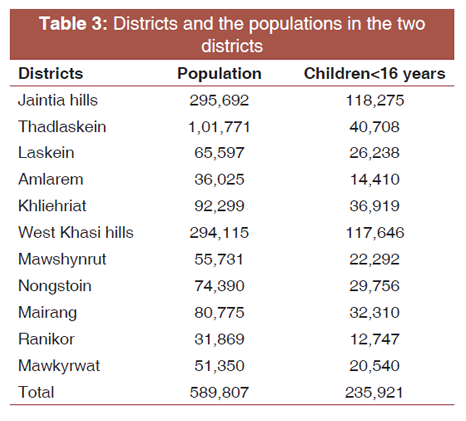
Meghalaya has a population of 2.964.007 population, and around 60% of the population is rural and children under 16 years of age consist of 40% of the population. Two districts randomly Jaintia hills and West Khasi hills were selected from the CBR program, within the Jaintia hills district only a few villages from Laskein were covered by the CBR program as there was lack of manpower and communication. In the West Khasi hills, the CBR program had mostly covered only Nongstoin and Mawkyrwat, Mairang, while the rest of the district is yet to be covered.
1. The population of the two districts covered consists of 589,807 total population.
2. Expected number of children under 16 years is 235,921 [Table 3].
The CBR program is operating in the states of Meghalaya for the past 5 years in different parts of the states under two NGO Organizations Bethany Society and National Social Services Society.
Under this CBR program, there were total of 22 CBR field workers who carried a house to house survey in different villages under the two districts. They identified the children who are either blind or SVI and entered their name in the CBR list. Several centers for examination and particular dates were fixed during the second and third of July 2011 were chosen.
In the west khasi hills, there is a social welfare center in Nongstoin in which all the children identified by them are brought to the center for screening, and in Mawkyrwat two community venues were chosen for screening of those children by the researcher (Ophthalmologist).
In Jaintia hills, there is a center operating under Bethany Society, where all the children are screened in this center.
Money for transport and free meals were given on that day, but this was not informed to the parents/guardian before.
Bethany Society started school for the blind known as Jyoti Shroat school in 1992 an inclusive pre-school until class 10 with special focus of student with visually impaired. It is a nodal ercenter for promoting Braille in Northeast India. Around 80 visually impaired children are enrolled in the school. The school is located right in the center of Shillong city. The source of funding is CBM, Bethany Society and donations.
Montfort center for education is situated in district Tura about 300 km from the state capital has a separate school for the blind for primary education known as Marian school for the blind and integrated and inclusive education in the secondary level. Special education teachers support the children in the school. The institution also offered courses and training for special education on speech and hearing impaired.
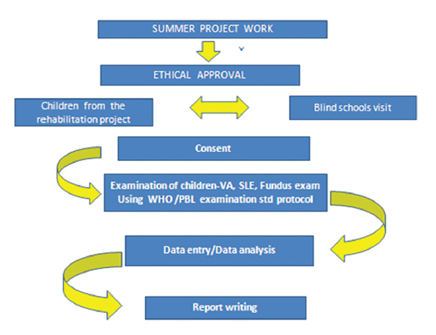
All the identified children from the two schools for the blind and through the CBR program (which was a house to house case detection exercises carried out by local NGO earlier in the year) were enrolled in the study. All the children who have fulfilled the criteria were examined as per the WHO/PBL examination standard protocol. Ethical approval was obtained from the London School of Hygiene and Tropical Medicine and the relevant authorities from the two schools for the blind and CBR program.
The required consent for the children examined was obtained either from the principal/headmaster in the two schools for the blind or the parents/guardians for the community.
Data collection on the children was obtained as follows:
1. Brief demographic details, medical and family history of each participant was possible were recorded.
2. A Snellens E optotypes were used to measure the presenting visual acuity in children over 3 years of age, and ability to follow the light in younger children.
3. Refraction was performed whenever was indicated using a trial lens set and frame.
4. Anterior segment examination was done using portable slit lamp microscopy; intraocular pressure was measured in those cases where there no scarring of cornea.
5. Posterior segment examination was performed using direct and indirect ophthalmoscope after dilatation of pupil.
6. Findings were documented in the WHO/PBL questionnaire, and the CBR workers were interviewed in detail to identify the challenges.
Children identified in need of medical and or surgical services were referred to the tertiary center for further management and evaluation.
RESULTS
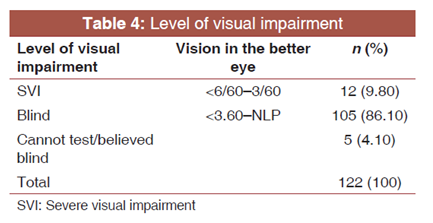
A total of 122 children attending the two schools for the blind and identified from the community by the CBR workers were examined. There were 49 (40.16%) from Bethany school, and 38 (31.15%) from Montfort school, and 35 (28.70%) from the community through the CBR all the children are under 16 years of age. 12 had SVI having a visual acuity of < 6/60 in the better eye and 105 were blind having a visual acuity of < 3/60 in the better eye and 5 could not be tested but believed to be blind due to the young age and uncooperative for visual acuity examination. Of the children referred by CBR workers, six came from Jaintia hills and 29 from the West Khasi hills district. The children were divided into two groups, according to the level of disability that is blind or SVI. The proportions with the said presenting vision are shown in Table 4.
Most of the children in the schools were blind (89%) but, at the same time, over (77%) of the children detected by CBR workers in the community were also blind. This highlights the proportion of previously undetected blindness in the community [Table 5].
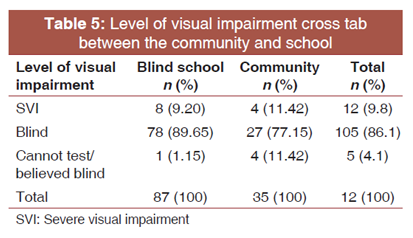
Figure 1 shows that the age 0-5 years children from the community were mainly from the younger age groups than in the blind school. This could be because the children were not yet in the school going age, in the age group 6-10 years and 11-15 years in the community were almost in the same proportion. In the school for the blind children of older age group 11-15 years are present in majority. Overall, the youngest of the children was 1 years and the oldest was 15 years with a mean age of 11.45 years.
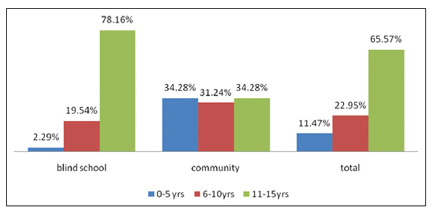
The children from the school for the blind were either in the integrated school or specialized school it is usually the children who are in the primary age of 4-10 years are in the specialized school, and above this age, they are placed in the integrated group. In the case of the community, most of the children with this disability did not attend school due to various reasons the children were of younger age group, the school was far away, or financial constraint and parents were not aware that there is a separate provision that the participant children with a disability could attend school.
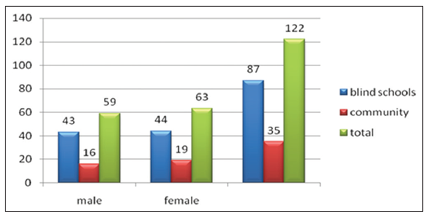
Figure 2 shows that males 43 (72%) in the blind schools compared to females 44 (69.85%). In the community, the participants were found to be female 19 (30.15%) to males 16 (27.12%) and on statistical testing P = 0.7 which is not significant and confidence interval (-16.03-22.09).
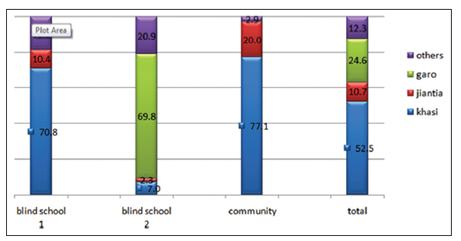
In the Figure 3 shows the distribution of different tribal groups in the two blind schools and the community, in blind school 1 which is located in the East Khasi hills district the majority of the tribal ethnic group are the Khasi which is reflected here in the figure were most of the children belong to this ethnic group (70.8%) then followed by Jaintia (10.4%) and the others (18.8%). As compared to the blind school 2 located in Tura district, the majority of the tribal group belong to the Garo tribes as shown in Figure 3 69.8%, then come the Khasi 7.0%, Jaintia 2.3%, and others 20.9 in the community since it covers by the CBR program mainly in the rural west Khasi hills and some villages of Jaintia hills where these tribes settle in these areas the main ethnic group are Khasi 77.1% followed by Jaintia 20% and the rest 2.9%. This shows that the majority is the Khasi, and the Garo tribes are represented here whereas the Jaintia tribe is less this may explained most of the villages in Jaintia hills have not been mostly covered by the CBR project [Table 6].
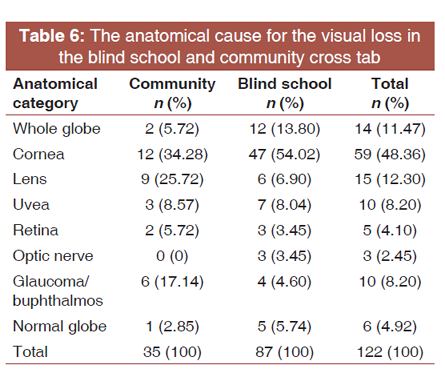
A total of 122 children from the blind schools and community were eligible for examination. The main cause of anatomical blindness and severely visually impaired in the blind school was corneal problem (54.02%), followed by globe abnormalities (13.80%), uvea (8.04%), lens related (6.90%), and glaucoma (4.60%).
As for the community corneal problem (34.28%) is also the major causes for blindness followed by lens related problem (25.72%). However, there is no statistical significant different in anatomical cause of blindness from the community and the blind school were the P value (yates' correction) is 0.104. This data have to be viewed with caution as 50% of the cells have frequency < 5 [Table 7].
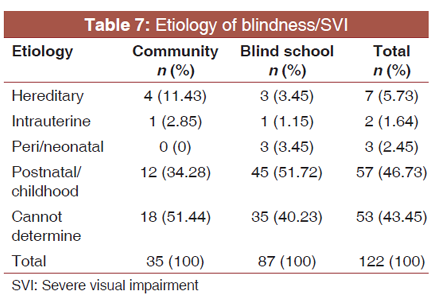
The etiological classification was based on the time of onset of the insult leading to visual loss, and the findings are shown in Table 7 in the blind schools the etiology is mainly the postnatal/ childhood factor 51.72% which is also similar for the children in the community 34.28% while hereditary cause was (5.73.%) it was difficult to identify a clear pattern/specific disease in the population as causes seen include (retinitis pigmentosa, albinism, and optic atrophy). About (43.45%) the cause is undetermined for both the children in the community and the blind school. There is no statistically significant difference in the etiological cause of the blind/SVI in the blind school and community as P = 0.4 which is insignificant [Table 8].
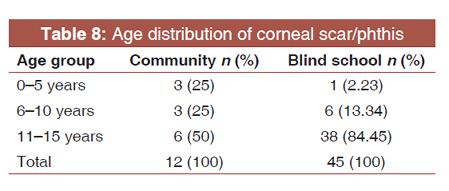
Table 8 shows that the different age distribution in the community and blind school with corneal scar 0-5 years 25% and 6-10 years 25% are of the younger age group in the community when compared to blind schools where the corneal scar is more in the older age group 11-15 years.
Majority of the children had an avoidable cause of blindness which is either preventable or treatable type of blindness. Corneal causes from VAD and measles combined together was the major preventable cause of visual loss 57 (48.7%), and cataract 15 (12.8%), and glaucoma/buphthalmos 10 (8.5%) was the main treatable cause [Figure 4].
The CBR program had been operating in West Khasi hills district for 4 years had been covering two sub-district Nongstoin, Mawkyrwat, and Mairang, and Jaintia hills [Table 9].
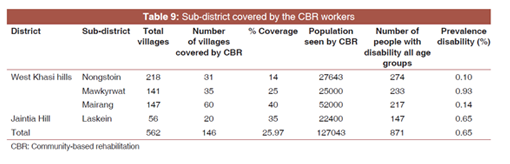
The sub-district covered by the CBR workers in house-to-house survey in the two districts with a total villages covered 146 out of 562 total villages covering total population of 127,043 and total number of disability 871 in all age groups with overall prevalence of 0.65% others type of disability (speech impairment, hearing impairment, locomotors, and mental retardation) this shows that the project had covered only 25.97%. Under this projects, the CBR fields worker do a house-to-house survey covering each village to detect and provides either referral medical services and various rehabilitation and vocational training for the disabled people [Table 10].
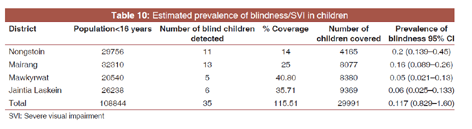
Based on our sample, the overall prevalence of blind/SVI in the children from the area covered by the CBR and the total number of children < 16 years from the total population of the two districts the prevalence is 0.117 (CI 0.829-1.60) making this a prevalence of 1.2/1000 children overall in the areas covered. The estimated prevalence was higher in Nongstoin 0.2 and Mairang 0.16 in both sub-district and lower in Mawkyrwat 0.05 and Jaintia hills 0.06.
Figure 5 shows the gender distribution of the total 22 CBR workers in the two districts who were trained by the local NGO agency with more female field workers 72.73% than men 27.27%.
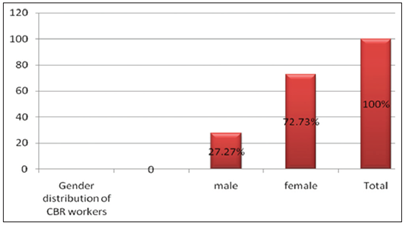
Figure 6 shows that majority of the CBR workers were in the age group 20-25 years 31.82% and 31-35 years of age 31.82%. This shows that these two age groups are more active as a CBR fieldworker and there is no statistically difference in the age of male and female workers as P = 0.2 which is not significant.
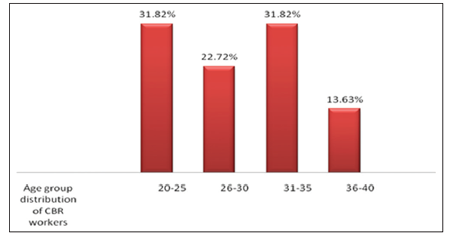
Figure 7 shows that the main challenges faced by the CBR workers to refer the children for further management whether for medical, surgical treatment, low vision services, or rehabilitation services. The main obstacles were financial reasons (33.34%) followed by distances to the center for receiving the services (26.66%) and also in beliefs that it is a disease which cannot be treated or only when the child reach adult age. Besides, lack of awareness about the services available is also another contributing factors face by the CBR workers while referring to the children.
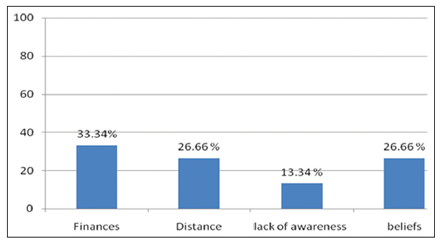
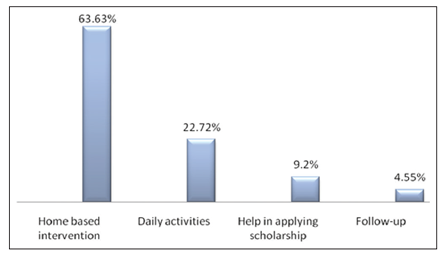
Figure 8 shows the various rehabilitation services provided by the CBR workers to the people in the community who are disabled and those who cannot afford to attend special school for disability due to their ages or due to financial problems or there is no one to accompany them. Around 64% are provided with home-based intervention (environment modification, providing walking sticks, wheelchair, ready-made Braille, hearing aids, etc.) and 23% for each daily activities independent eating, toilet training, personal cleanliness and 9%. Help in applying the various scholarship/grants given by the social workers and about 2% for follows up in the school.
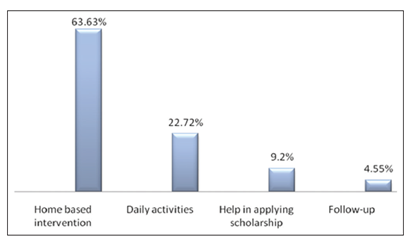
Figure 9 shows the percentages of acceptance from the household while doing house-to-house survey where the majority of the parents of the children or the guardian about (50.00%) accept the services and examination of the children who are disabled 18.8% they do not accept while the rest (31.82%) half will respond after repeated request and home visit and creating awareness of importance of detection and rehabilitation services whether in the institution or the respective houses.
DISCUSSION
This study provided us with the first data on childhood blindness in Meghalaya a predominantly tribal region of India. The methodology used was to describe the childhood blindness as seen in the schools for the blind but also took advantage of a house-to-house survey through the CBR program that has been implemented for the past 4 years for the detection of disabilities (including blindness).
The estimates on the prevalence of childhood blindness were extrapolated from the children in villages already surveyed by CBR program. This was 1.2/1000 children and this finding correlates with the findings of the studies done in the very poor socioeconomic countries where preventable blindness due to corneal scar is high 21%[32] this suggests that higher prevalence of preventable blindness is associated in region with low socioeconomic status due to lack of accessibility and poor quality of health and eye care services available to them. This study reflects that Meghalaya states are still a very poor socioeconomic developed states with underdeveloped health-care provision.
Among children attending school for the blind and community the most common cause of blindness/SVI were corneal blindness (48.36%). There are many factors which contribute to corneal blindness of which VAD is the leading causes of corneal blindness a history of measles; diarrhea can also precipitate vitamin A deficiency were also recorded.[33,34] The high incidence of VAD-related blindness, which is an easily preventable cause of blindness vary from the different region as we had seen in the others states in India like Maharashtra in West India corneal blindness has decreased in these states.[25] However, on comparing with the study done in Northeast Indian states in 12 schools for the blind the major anatomical causes of blindness/SVI were corneal condition 36.4%[23].
In the community, the major cause of blindness/SVI was also corneal blindness 34.28%, and the participant was of younger age group 0-5 years this shows that VAD-related corneal blindness is still persisting in the remote NE states when compared to other states. The reason for this is the unbalanced diets among the poor rural children particularly the pre-school aged children suffering from subclinical Vitamin A. Meghalaya also recorded having a prevalence rate of diarrhea of 6.1%[35] this is due to poor environmental sanitation and unsafe drinking water. Measles immunization coverage in the state is only 33% and high infant mortality rate of 58/1000 (census 2010). The percentage of children receiving Vitamin A is only 24.7% which is below the national average 29.7%. As vitamin A deficiency is linked to childhood mortality[31].
it become public health issue not only for prevention of blindness, but the efforts to achieve high coverage of measles immunization and Vitamin A supplementation coverage still remains in deficit as it was before. Barriers to uptake of measles immunization and vitamin prophylaxis are also believed to be a contributing factor.
Congenital abnormalities of the globe (microphthalmos, anophthalmos, and coloboma) were responsible for 12% of the blindness and visual impairment which are almost comparable to the study in Northeast and a population-based study done in South India where congenital abnormalities are 16.7%; this is a common finding in studies on blind children in other parts of India in Maharashtra as the common cause of blindness which requires rehabilitation services.
Lens related cause for blindness due to cataract was 12.8%, glaucoma 8.5% these are the treatable cause of blindness this shows that the pediatrics quality services and good comprehensive screening program need to be more strengthened in the states.
Majority of the etiological cause was unknown about 40.2% is seen in this study and usually most of the children are presented for examination in the late stages of the diseases in which the causes cannot be ascertain as most of the cases are sporadic and unknown, associated with lack of proper medical history and concrete information. This results also added another consistent report as obtained from others studies in Maharashtra and NE India using similar methods which we can conclude that there is a limitation in further investigations.
It is believed and shown that hereditary factor 5.7% and perinatal 2.5% and intrauterine factor 1.6%, this lower proportion of genetic factor is also found in the similar study in blind school in NE which most likely related to the absence in consanguineous marriage in the states as compared in South India where the genetic cause is the highest[20].
The study shows that the diversity of childhood blindness in the Northeastern region preventable cause of blindness like corneal blindness due to VAD is still the major cause of blindness/SVI in both the blind school (56.25%) and the community (38.70%) followed by treatable cause of blindness/ SVI such as cataract and glaucoma. This is comparable to other studies done in other parts of NE states from different blind school , where nearly half of the children are blind from avoidable blindness and similar findings in studies done in Andhra Pradesh in South India[21]. Congenital abnormalities also posed as a new challenges more research in this field are needed to identify the underlying causes and new advance methods for management is also required [Image 4].
In the blind school participants there were almost equal number of males and females and in the community the same result is seen statistical analysis on the difference in gender proportion, shows a P = 0.7 confidence interval (-16.03-22.09) which shows that it is not significant which suggest that tribal cultural factors are still being followed and a Matriarchal society still exists, where females are empowered and treated equally in all sphere of life[36,37]. This in contrast to others reported studies in the blind school of India where 60% of the children are males[22].
The distribution of age group in the community and blind school participant is as expected in any others blind school study where the participant of younger age group is less whereas the older age group is in majority. This fact likely as quoted by others to introduce selection bias in a blind school as the participant who was not enrolled might be different from the participants who were not in the school.
The KIM methods use to identified children of younger age group was been adopted in many others countries but in this study we used the CBR workers to identify younger age group as this is also found to be very useful in identifying children from the community at an earlier age and receive treatment early. The key differences here that the CBR program has a broader remit to identify all disabilities and also provide referral and community based support as compared to the community as a whole. It is, however, key methods to reach tribal population in remote, isolated areas.
The CBR projects which have been running for 5 years in the different states of Meghalaya covering different parts of the district, in this study, so far we had covered only two districts the West Khasi hills and the Jaintia hills with a total number of the population are 127043 at present. Under this projects, the CBR detect the people with disability and provides services to them not only in terms of medical facilities but also offers various services for rehabilitation, social inclusion, and poverty reduction[38].
The study the main challenges faced by the CBR workers was to refer the children for further management the main barriers at the community level were financial reasons, followed by lack of transport and far distances to nearest center, lack of awareness and beliefs, these findings are incomparable with other studies for causes of barriers in receiving eye care services. As we have seen in our study that most of the participants are from the remote, interior villages where road condition are bad most of the year, difficult terrain to take a visually disabled child to the referral center of the town imposed a burden to the parents and family members lack of awareness and beliefs is also cited here as also another contributing factors, where cultural beliefs about scientific medicines cannot cure these type of blindness and resorting to other traditional alternative. This study shows the importance of establishing an accessibility, affordability, and acceptability of eye care services to the people in the rural areas is urgently needed in the state since majority of the blindness/SVI in the children are preventable and treatable and eye problem is a condition which need immediate treatment and good referral system with a good linkage between the primary and the secondary eye care centers.
In the study, the CBR workers provided rehabilitation services to the community who were suffering from irreversible blindness and others disability and not attending any integrated/special school due to the many barriers. About 64% are provided home-based intervention such as household environment modification, wheelchair, walking stick, ready printing Braille, and printing materials which are provided free of cost, and the rest to teach daily activities in the household such as toilet training, independent eating, and personal cleanliness and help in applying for disability certificates and grants scholarship from district social welfare boards. Further, it is found that the majority of the services are accepted by the community, and the response to examination is about 50% in the household.
The CBR worker is a key link, especially the female workers between the ages of 20-35 years. Moreover, this findings are similar to others study in key informant methods[16] this reflect the fact that men are less likely to be motivated, to take a social welfare job and prefer migrating to the cities for better opportunities.
Meghalaya has multiple difficulties - high prevalence of blindness among the remote tribal populations, underdevelopment of treatment and rehabilitation services. Most of the causes are preventable if the primary intervention of measles immunization and Vitamin A supplementation can be strengthened. The work done by CBR workers to identify and support communities is an essential step and should be strongly supported with good referral systems and health education programs.
This is a pilot study, and due to various constraints, the sample size was small (n = 122). We estimated around 250 children to be investigated; however, it was a monsoon season and many participants who were already identified by the field worker were absent because of landslides and poor road condition. Second, there was a strike called by fundamental group on1 7-20th July and movement to the field got restricted. Finally, the investigator also could not reach few destinations due to the poor climatic condition and time constraint. In the blind school, some of the students are missed who did not come back in time after the summer break. As shown in the statistical analysis of the data, no concrete report on the estimation of the magnitude of childhood blindness can be made on the data that we collected.
CONCLUSION
The high incidence of avoidable blindness was found in this study, which is a major cause of blindness in the state and is similar to the studies done in other parts of NE India. These findings suggest the importance of primary prevention and the need to expand, improve the quality and provide accessibility and affordability of pediatric eye care services in the state. It can be concluded that Vitamin A related blindness is still a major problem in NE India with poor primary health care.
The use of CBR workers to identify the children and to referring them for further management was found to be useful as they can be used to engage for more extensive research studies and to provide services such as follow-up of the child, rehabilitative services, and a link between the community and health providers.
RECOMMENDATIONS
Short-terms measures (next 6 months):
1. To disseminate the results of this study with various key stakeholders-NGO, CBR workers, schools for the blind, maternal and child health programs with the active involvement of medical and paramedical staff to coordinate and strengthen the existing health system.
2. To strengthen in case of detection among children in the community by offering additional training to the CBR workers in identifying different causes of visual impairment.
3. Advocate ministry of health and NGOs in the state for the need of comprehensive primary health-care strategies and improved the quality of facilities at the primary level mainly for measles, early management of diarrheal diseases, infections, and malnutrition can bring significant reduction in U5MR and Vitamin A related blindness.
4. Primary eye health should be included in the primary health by training the existing health workers, the staff from maternal child health clinic, traditional birth attendant about the common eye problem and treatment, detection and referral of any abnormality. Training can be provided using visually charts as has been tried in Tanzania[39]
5. Advocacy with government, stakeholders, partner agency to coordinate and strengthen Measles immunization coverage, and Vitamin A prophylaxis.
6. Needs further expands and improved pediatrics ophthalmic services in the states, established a low vision clinic, rehabilitation services, and improved referral system.
7. To establish a standard protocol with the two schools for the blind for the recommendation of preliminary screening by an ophthalmologist before entry to the school and regular follow-up.
Medium terms measures (next 2 years):
1. Strengthen food supplementation program for children < 6 years and pregnant and lactating mothers and food fortification with Vitamin A.
2. Urgent needs to established and strengthen the network of eye banks and awareness on corneal donation to managed corneal blindness and treatment facilities [Images 1 and 3].




Long-terms measures (next 5 years):
1. Behavioral changes in food habits in consuming food items rich in Vitamin A which are easily available and affordable
2. Efforts for comprehensive development of the community by encouraging community participation, addressing the development of others sectors such as education, poverty alleviation, agriculture, environmental sanitation, and safe drinking water.
3. The accessibility and socio-cultural acceptability of intervention of VAD through prophylaxis program need to be assessed.
4. Inclusion to encourage access of people with disability in all mainstreams services, for example, education, employment, social welfare services, political field, and increase public awareness.
ACKNOWLEDGMENT
I would like to thank God for blessing me and my family so that I can complete my course.
My sincere gratitude to my course Director and my supervisor Dr. Daksha Patel for continuous support and encouragement during the course and completion of my project. I would like to thank Dr. GVS Murthy for his advice and encouragement and special thanks to Dr. Babar Quereshi for making it possible for me to enroll into this course. Thanks to my sponsors Task force sight for life, Dutch Lions and British Council for prevention of blindness for sponsoring me so that I can pursue in this challenging course. I would also want to thank Dr. Patnaik for his guidance. Many thanks to Mr. Carmo Naroha for helping me and involved in conducting the survey, my friend Dr. Harish Mudgal for his help thanks you very much. I would to express my thanks to my husband Dr. S. P. Saikia for his love and support to me and my daughter Tanvi Rowena.
REFERENCES
- Foster A. Childhood blindness in India and Sri Lanka. Indian J Ophthalmol 1996;44:57-60.
- Gilbert C, Foster A. Childhood blindness in the context of VISION 2020--the right to sight. Bull World Health Organ 2001;79:227-32.
- World Health Organisation. Preventing Blindness in Children in WHO/IAPB Scientific Meeting 1999. Hyderabad, India.
- Rahi JS, Gilbert CE, Foster A, Minassian D. Measuring the burden of childhood blindness. Br J Ophthalmol 1999;83:387-8.
- Gilbert C, Muhit M. Twenty years of childhood blindness: What have we learnt? Community Eye Health 2008;21:46-7.
- Gogate P, Kalua K, Courtright P. Blindness in childhood in developing countries: Time for a reassessment? PLoS Med 2009;6:e1000177.
- Chandna A, Gilbert C. When your eye patient is a child. Community Eye Health 2010;23:1-3.
- Foster A, Gilbert C. Epidemiology of visual impairment in children. In: Taylor D. Paediatric Ophthalmology. London: Blackwell Science; 1997. p. 3-12.
- Thylefors B. A global initiative for the elimination of avoidable blindness. Community Eye Health 1998;11:1-3.
- Gilbert C. New issues in childhood blindness. Community Eye Health 2001;14:53-6.
- McMeel JW, Jack RL. Who/Pbl eye examination record for children with blindness and low vision. Br J Opthalmol 1995;4:15.
- Gilbert C, Foster A, Negrel AD, Thylefors B. Childhood blindness: A new form for recording causes of visual loss in children. Bull World Health Organ 1993;71:485-9.
- Mohan M. National Survey of Blindness-India. NPCB-WHO Report. New Delhi: Ministry of Health and Family Welfare, Government of India; 1989.
- Dandona R, Dandona L. Childhood blindness in India: A population based perspective. Br J Ophthalmol 2003;87:263-5.
- Moulton L. Community based rehabilitation and prevention of blindness in South West Uganda. Community Eye Health 1998;11:51-2.
- Muhit MA, Shah SP, Gilbert CE, Hartley SD, Foster A. The key informant method: A novel means of ascertaining blind children in Bangladesh. Br J Ophthalmol 2007;91:995-9.
- Murthy G, John N, Gupta SK, Vashist P, Rao GV. Status of pediatric eye care in India. Indian J Ophthalmol 2008;56:481-8.
- Resnikoff S, Pascolini D, Etya'ale D, Kocur I, Pararajasegaram R, Pokharel GP, et al. Global data on visual impairment in the year 2002. Bull World Health Organ 2004;82:844-51.
- Banthia JK. Census Commissioner, Census of India, 2001. New Delhi: Controller of Publiations; 2003.
- Rahi JS, Sripathi S, Gilbert CE, Foster A. The importance of prenatal factors in childhood blindness in India. Dev Med Child Neurol 1997;39:449-55.
- Hornby SJ, Adolph S, Gothwal VK, Gilbert CE, Dandona L, Foster A, et al. Evaluation of children in six blind schools of Andhra Pradesh. Indian J
- Rahi JS, Sripathi S, Gilbert CE, Foster A. Childhood blindness in India: Causes in 1318 blind school students in nine states. Eye (Lond) 1995;9 Pt 5:545-50.
- Bhattacharjee H, Das K, Borah RR, Guha K, Gogate P, Purukayastha S, et al. Causes of childhood blindness in the northeastern states of India. Indian J Ophthalmol 2008;56:495-9.
- Titiyal JS, Pal N, Murthy GV, Gupta SK, Tandon R, Vajpayee RB, et al. Causes and temporal trends of blindness and severe visual impairment in children in schools for the blind in North India. Br J Ophthalmol 2003;87:941-5.
- Gogate P, Deshpande M, Sudrik S, Taras S, Kishore H, Gilbert C, et al. Changing pattern of childhood blindness in Maharashtra, India. Br J Ophthalmol 2007;91:8-12.
- Dandona R, Dandona L, Srinivas M, Sahare P, Narsaiah S, Munoz SR, et al. Refractive error in children in a rural population in India. Invest Ophthalmol Vis Sci 2002;43:615-22.
- Murthy GV, Gupta SK, Ellwein LB, Munoz SR, Pokharel GP, Sanga L, et al. Refractive error in children in an urban population in New Delhi. Invest Ophthalmol Vis Sci 2002;43:623-31.
- Nirmalan PK, Krishnaiah S, Shamanna BR, Rao GN, Thomas R. A population-based assessment of presbyopia in the state of Andhra Pradesh, South India: The Andhra Pradesh eye disease study. Invest Ophthalmol Vis Sci 2006;47:2324-8.
- IVE, A.G.L.O.B.A.L.I. and O. DABLE, Community Eye Health.
- Bhatia V, Swami HM, Rai SR, Gulati S, Verma A, Parashar A, et al. Immunization status in children. Indian J Pediatr 2004;71:313-5.
- Sharma S. Immunization coverage in India. In: Institute of Economic Growth. New Delhi: University of Delhi; 2007.
- Steinkuller PG, Gilbert C, Collins ML, et al. Childhood blindness. J Am Assoc Pediatr Ophthalmol Strabismus 1999;3:26-32.
- Foster A, Sommer A. Corneal ulceration, measles, and childhood blindness in Tanzania. Br J Ophthalmol 1987;71:331-43.
- Miller M, Humphrey J, Johnson E, Marinda E, Brookmeyer R, Katz J, et al. Why do children become Vitamin A deficient? J Nutr 2002;132:2867S-2880S.
- Murkherjee S. Geo-Medical Aspects of Acute Diarrhoel Diseases in Meghalaya Third Intrnational Conferences on Environmental and Health Chennai; 2003. p. 276-83.
- Chakrabarty B. A Survey of the Status of Young Children in North-East India. Undoing our Future: A Report on the Status of the Young Child in India; 2009. p. 144.
- Passah P. Changes in the Matrilineal System of Khasi-Jaintia Family. Matriliny in Meghalaya: Tradition and Change. New Delhi: Regency Publications; 1998. p. 74-9.
- WHO-World report on Disability 2011. 2011.
- Byamukama E, Courtright P. Knowledge, skills, and productivity in primary eye care among health workers in Tanzania: Need for reassessment of expectations? Int Health 2010;2:247-52.