Outcome of Surgical Implant Generation Network Intramedullary Nail in Diaphyseal Femur Fractures at a Tertiary Care Center in Nepal
Praphulla Shrestha1, P. Chalise1, R. K. Shah2, R. P. Singh1, A. K. Mishra1, V. Adhikari1, N. K. Shah3
2.Department of Bone & Joint Surgery, Norvic International Hospital, Kathmandu, Nepal,
3.Department of Trauma Surgery, Janakpur Trauma Hospital, Janakpur, Nepal
Citation : Shrestha P, Chalise P, Shah RK, Singh RP, Mishra AK, Adhikari V, Shah NK. Outcome of Surgical Implant Generation Network Intramedullary Nail in Diaphyseal Femur Fractures at a Tertiary Care Center in Nepal. Clin Res Orthop 2018;1(1):1-5.
Surgical implant generation network (SIGN) is a USA-based humanitarian organization which invented and provided SIGN solid intramedullary interlocking nail to the low- and middle-income countries (LMICs) in the world including Nepal for free. In a LMIC like Nepal, the necessary implants are not affordable for patients especially in a public hospital setting. The SIGN nail is actually designed for tibia, but for our patients, we have been using the same nail for the femur too - both antegrade and retrograde. In this study, we analyzed cases of diaphyseal femur fracture treated primarily with SIGN nails. We studied about the union rate, time taken for union, and the rate of complications including function from the SIGN database.
After the permission from the SIGN office and Ethical Clearance from the institution, we analyzed the cases from our database. A total of 106 cases of femur fracture fixed with SIGN nail were found in our database. Of 106 cases, 63 cases met the inclusion criteria. The data were entered into SPSS 16, and the results were obtained after analyzing the data.
Of 63, 61 (96.83%) fracture united. The average time of union of femur fractures in this study was 13.34 weeks. We encountered 2 (3.17%) cases of non-union. There were 3 (4.76%) cases with minor complications, and 1 (1.59%) patient with non-union was due to deep infection.
SIGN nail provides an acceptable union rate in diaphyseal femur fracture fixation with a low rate of complications.
Femur fracture, surgical implant generation network nail, union,Orthopaedics,asclepiusopen
INTRODUCTION
Surgical Implant Generation Network (SIGN) fracture care international is a non-profit organization which helps the surgeons in the low- and middle-income countries (LMICs) by providing SIGN intramedullary interlocking nails along with its instrument set free of cost. The SIGN concept was developed by Lewis G. Zirkle, MD, the founder and president of SIGN, 40 years ago. He was serving as an army orthopedic surgeon in Vietnam, treating military personnel and injured Vietnamese civilians, when he developed a compassionate concern for their health needs. He worked with like-minded people and developed this concept of teaching, training, and providing the implants to the developing world as a charity[1].
The rate of road traffic accidents is increasing, and the number of fatalities is highest in the LMICs. More than 90% of deaths occur in the LMICs[2]. The most common cause of death in 15-25 years of age group is road traffic injuries[3]. Nepal is also listed in the countries with a higher rate of road traffic accidents[4]. The fractures of diaphysis of femur are a major cause of morbidity and a prominent social issue when the breadwinner of the family is involved in the accident. The most preferred and effective method of treatment in femoral diaphyseal fracture is intramedullary interlocking nail[5].
Intramedullary nailing of femur shaft fractures achieves more than 90% of union rate[5]. SIGN nails are used for both tibia and femur (antegrade and retrograde). It has a 9° bend in the proximal part and the distal end is tapered so that the nail slides smoothly in the cortex during insertion. The nail is solid and is provided with a target arm along with instruments which allow the interlocking screws (including distal screws) to be inserted without an image intensifier[6].
The use of SIGN nails started at Nepal Medical College Teaching Hospital, Kathmandu in Nepal way back in the early 2000, and now, we have many centers which are using the SIGN nails across Nepal. We have been using SIGN nails for femur in our center, but the outcomes of our cases were not studied till this date. This study is aimed at determining the outcome of our own cases which will be evidence to our work and also direct the future in the areas that need to be improved.
MATERIALS AND METHODS
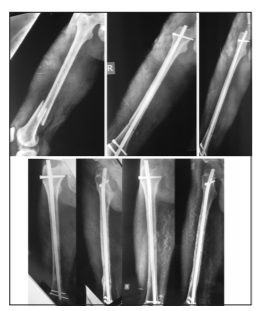
The permission from the SIGN office was obtained before the start of the study for the use of data from the SIGN database. The Ethical Clearance from the Institutional Review Board of Nepal Medical College Teaching Hospital was obtained. We performed a retrospective observational study. The data entries of our cases from SIGN database from 2003 to June 2017 were obtained. A total of 106 cases of femur fracture fixed with SIGN nail were found in our database. Of 106 cases, 63 cases met the inclusion criteria. Two cases were excluded who had bilateral femur fractures. Both cases needed long hospital stay in the intensive care unit due to development of fat embolism. Both patients underwent external fixator for damage control followed by SIGN nails. The fractures healed in both patients. There were cases of infected nonunion, and cases who received SIGN as a secondary treatment, especially the aseptic non-unions, in which they received hollow nail as a primary treatment also were excluded. The patients with lost follow-ups were also excluded from the study. Some patients were also contacted on phone for the ongoing follow-up, and data were entered with the X-rays and the clinical pictures were obtained from the locally available surgeons [Figure 1]. The data were entered into SPSS 16 and the results were obtained after analyzing the data.
The variables measured were the time taken for fracture union, union rate, and rate of complications.
RESULTS
Of 63 cases, 50 patients were males and 13 were females, and their ages range from 18 to 82 years. The most common mode of injury was road traffic accident followed by fall from height. 59 patients had closed fracture, and 4 of them were open Grade 1 and 2. 36 (57%) had a fracture of the midshaft, followed by 14 (22%) in distal and 13 (21%) in proximal shaft. 36 (57%) fractures were reduced closed and 27 (43%) fractures required open reduction. Antegrade approach to femur was used in 48 (76%) patients and retrograde in 15 (24%) patients. Hand reaming was done in 59 cases (94%), and power reaming was used in only 4 cases (6%). In 43 patients (68.2%), the nail of 9 -mm diameter was used. 8 -mm nail was used in 14 patients (22.2%) . The nail lengths commonly used were 360 mm, 320 mm, 380 mm, and 340 mm [Table 1]. Locking was done on both distal and proximal holes in all except one in which proximal locking was not performed. Poller screws were used in two cases only. We did not encounter any complications in 58 patients. 61 patients achieved union and 2 patients went into nonunion. One had deep infection followed by nonunion of the fracture. One patient had aseptic nonunion. Two patients had distal screw problems - in one the screws loosened and other one had distal screw breakage, but the fracture united in both of these patients. One patient had superficial wound infection.

DISCUSSION
Road traffic accident is predicted by the WHO to be the seventh leading cause of death by 2030[2]. In the LMICs like ours, more than 25% of the population lives below poverty line[7] and the health cost is born by the patient themselves. The people who visit the public institution like ours are unable to pay for implants. The SIGN nail which is provided to our institution is a nail designed for tibia. But that nail has also been used in femur and humerus as well[8]. Fractures of the femur pose a lot of morbidity. It can cause life-threatening complications like fat embolism[9]. Perkins traction is considered a viable and cost-effective treatment option in adult diaphyseal femur fracture in some places of the world till now[10]. However, the cost-effectiveness of Perkins traction has been challenged by a study done in Cambodia comparing SIGN nail with Perkins traction. [11]They conclude that, in a particular setting, SIGN intramedullary nailing in adult femoral diaphyseal fractures gives better outcomes at lower costs and is much more cost-effective than Perkins skeletal traction[11]. In the current context, the standard treatment of diaphyseal femur fracture is intramedullary nail[5]. There are different designs available. Unlike other nails, SIGN intramedullary nail is solid, and intraoperative image intensifier is not required for inserting locking screws including the distal locking screws. More than 77% of patients in our study are < 50 years of age. This shows that younger people are more active and are more vulnerable to injury due to their active lifestyles. In the LMICs, the males are mostly the active members of the family and the breadwinner of the family so are vulnerable to injury and trauma. Males are more commonly (79%) affected than females because of the fact that, in our country, males are typically the breadwinner of the family and have to travel or go outside the house for their work [Table 1].
We had only four cases of open fracture of the femur. One of the open fracture cases suffered deep wound infection. This patient went into infected nonunion. Almost half of the fractures needed open reduction. In Africa, Sekimpi et al.[12] had performed 96% open reduction of the fractures and Ikem et al.[13] had performed 85% open reduction of fractures in their studies. We differ from them in this aspect because, in the study done by Sekimpi et al., [12] they mentioned that they had no fracture table in their center. We have a fracture table in our center and we use it for femur nailing so that might be one reason that the rate of open reduction is less in our study. In the study by Ikem et al.,[13] he has not stratified the long bones and has not separately mentioned how many of the femur shaft fractures were openly reduced so that hinders the comparison with our study. Reaming was almost always by hand in our study using the reamers provided by SIGN Fracture Care International. In four cases, we used power reamers because of the tight intramedullary canal. In these patients, we had to use 8-mm diameter nails due to the narrow diameter of canals. In our series, most of the fractures united at 10-16 weeks and average union time is 13.34 weeks. Sekimpi et al.[12] have reported healing of all fractures in his series but have not mentioned about the union time. In the study by Ikem et al.,[13] average time for union was 12 weeks, but due to non-stratification of long bones, the comparison is not possible with our study. In one study in Nigeria, Ikpeme et al.[14] have reported union time of 17 weeks in average, but their study included malunions and nonunions along with fresh femur fractures. We had union in 61 (97%) cases. Union rate in our study is comparable to other intramedullary nailing procedure in the femur in a Chinese study which showed a union rate of about 97%[15].
We had two cases of nonunion - one was aseptic nonunion and other was infected nonunion. One patient had superficial infection which was treated with extended antibiotic course and dressing. The patient with delayed deep infection and infected nonunion was treated with debridement of the fracture site, reaming of intramedullary canal followed by exchange nailing with larger diameter nail. This treatment has been recommended in an article by Shah et al.[16] Patient with aseptic nonunion was treated with the removal of SIGN nail followed by compression plating of the fracture which eventually united. Although one patient had screw breakage and one had distal screw loosening, both of the femurs went on to unite. One case with midshaft fracture of femur was operated by closed reduction and SIGN nailing with 1 proximal and 2 distal interlocking screws. In her immediate post-operative period, once she started ambulation, she complained of pain at the fracture site with a clicking sound. We thought that it was instability of the distal fragment over the nail. We decided her to take to the operating room after few days, and a poller screw was added to the distal fragment in anteroposterior fashion on the lateral side of the nail just below the fracture site. Following that, the patient's symptoms disappeared and she was comfortably ambulating with support. Later on, the fracture went on to heal without any complications. Poller screw is recommended in fractures to improve fixation and maintain a reduction in proximal or distal tibia fractures,[17] but the use of the poller (blocking) screws in femur also proved to be useful in two cases in our study. We have used cerclage steel wires to maintain fracture reduction in 8 cases, especially in those fractures which were long oblique and were in the distal or proximal shaft of the femur.
Our study is an observational study with a low level of evidence. This study lacks a control group. Due to the paucity of articles on SIGN nail in the femur, comparison of result is very difficult. The study period is too long, and different surgeons were involved at different points of time that might have an impact of observer bias.
CONCLUSION
SIGN nail provides an acceptable union rate of femur fractures with low rate of complications in low- and middle-income countries.
ACKNOWLEDGMENTS
Dr. Lewis Zirkle and SIGN Fracture Care International provided all the nails and its instrumentation free of cost. We thank them for their support. We would like to thank Dr Suman Thapa Magar, Dr Avinash KC and Dr Lalit Chaudhary for their help in data management and analysis.
REFERENCES
- Carsen S, Park SS, Simon DA, Feibel RJ. Treatment with the SIGN nail in closed diaphyseal femur fractures results in acceptable radiographic alignment. Clin Orthop Relat Res 2015;473:2394-401.
- Toroyan T. Global status report on road safety. World Heal Orgain 2015;318. Available from: http://www.who. int/violence_injury_prevention/road_safety_status/2013/ en/%5Cnhttp://www.who.int/violence_injury_prevention/ road_safety_status/2015/en. [Last accessed on 2018 Jul].
- World Health Organization. International traffic safety data systems improvement participant workbook data. Gen Assem Sixty-Eight Sess 2004;11:1-164. Available from: http:// www.link.springer.com/chapter/10.1007/978-88-470-2131-0_11%5Cn%3CGo to ISI%3E://WOS:000281167600012. [Last accessed on 2018 Jul]
- Huang L, Poudyal AK, Wang N, Maharjan RK, Adhikary KP, Onta SR. Burden of road traffic accidents in Nepal by calculating disability-adjusted life years. Fam Med Community 2017;5:179-87.
- Ricci WM, Gallagher B, Haidukewych GJ. Intramedullary nailing of femoral shaft fractures: Current concepts. J Am Acad Orthop Surg 2009;17:296-305.
- Zirkle LG, Shearer D. SIGN technique for retrograde and antegrade approaches to femur. Technol Orthop 2009;24:247-52.
- Index Global Hunged. 2010 Global Hunger Index: The Challenge of Hunger: Focus on the Crisis of Child Undernutrition; 2010. Available from: http://www.ebrary.ifpri. org/cdm/ref/collection/p15738coll5/id/4764. [Last accessed on 2018 Jul].
- Zirkle LG. Technique manual of SIGN IM nail and interlocking screw system insertion and extraction guide. Sign Fract Man 2012;1-47. Available from: http://www.signfracturecare.org. [Last accessed on 2018 Jul].
- Silva JJ, de Diana DA, Salas VE, Zamboni C, Neto JS, Christian RW. Fat embolism syndrome in femoral shaft fractures: Does the initial treatment make a difference? Rev Bras Ortop 2017;52:535-7.
- Bezabeh B, Wamisho BL, Ecsa FC. Treatment of femur shaft fractures using Perkins' traction at Addis Ababa university: An Ethiopian experience. East Afr Orthop J 2010;4:12-8.
- Gosselin RA, Heitto M, Zirkle L. Cost-effectiveness of replacing skeletal traction by interlocked intramedullary nailing for femoral shaft fractures in a provincial trauma hospital in Cambodia. Int Orthop 2009;33:1445-8.
- Sekimpi P, Okike K, Zirkle L, Jawa A. Femoral fracture fixation in developing countries: An evaluation of the surgical implant generation network (SIGN) intramedullary nail. J Bone Joint Surg Am 2011;93:1811-8.
- Ikem IC, Ogunlusi JD, Ine HR. Achieving interlocking nails without using an image intensifier. Int Orthop 2007;31:487-90.
- Ikpeme I, Ngim N, Udosen A, Onuba O, Enembe O, Bello S. External jig-aided intramedullary interlocking nailing of diaphyseal fractures: Experience from a tropical developing centre. Int Orthop 2011;35:107-11.
- Ma YG, Hu GL, Hu W, Liang F. Surgical factors contributing to nonunion in femoral shaft fracture following intramedullary nailing. Chin J Traumatol 2016;19:109-12.
- Shah RK, Singh RP, Quasem MF, Faruquee SR, Harrison J. SIGN interlocking nail for the treatment of infected nonunion. Tech Orthop 2009;24:289-96.
- Shah RK. Treatment of diaphysio-metaphyseal fracture of tibia by intramedullary nail in combination with poller screw. J Bone Res Rep 2015; 1:1-5.