Bilateral Anterior Shoulder Dislocation in a Paratrooper: A Case Report
Amir Oron1, Niv Netzer1, Philip Rosinsky1, Yuval Arama1, Eyal Behrbalk2
2. Department of Orthopedics, Hillel Yaffe Medical Center, Hadera, Israel.
Citation: Oron A, Netzer N, Rosinsky P, Bilateral Anterior Shoulder Dislocation in a Paratrooper: A Case Report. Clin Res Orthop 2018;1(1):1-2.
A case of bilateral anterior glenohumeral dislocation in a 19-year-old soldier is presented. The patient, a 19-year-old soldier, in the Israeli Defense Forces paratrooper core, had been at the end of a strenuous drill, carrying a stretcher and gear for a distance exceeding 20 km. While dismounting the stretcher, the patient hyperextended his humeri in the mid-abducted position, pivoting their heads out of their sockets. Closed reduction under sedation was performed, and there were no complications. After 6 weeks in bilateral broad arm slings, with pendulum exercises from 2 weeks on, the patient started to mobilize his arms and achieved a full range of motion. It may be postulated that the physical exhaustion, combined with sleep deprivation, allowed for the bilateral hyperextension in mid-abduction and the eventual bilateral shoulder dislocation.
INTRODUCTION
Bilateral glenohumeral joint dislocations are rare. The forces acting on both the shoulders should be of similar magnitude, direction, and timing. The most common mechanism causing bilateral shoulder dislocations are cases where epileptic convulsions cause violent muscle contractions which subsequently bring about dislocation of the humeral head, usually in a posterior direction [1]. Other causes of bilateral injuries have included falls [2], electrocution [3], sports activities [4,5], and nocturnal hypoglycemia [6].
Bilateral glenohumeral joint dislocations following sports-related activity and specifically a slow exhaustion derived mechanism were first reported in 1987, in a weightlifter, using a bench press when, due to exhaustion, the athletes' arms were forced into extension, abduction, and external rotation [7]. This mechanism was reported on once again in 1998 by Cresswell and Smith [8] where the humeral shaft gradually pivoted on the bench while using a free weight bar in the bench press position, and thus, the humeral heads were slowly dislocated anteriorly by the weight of the bar. We present a case of bilateral anterior glenohumeral dislocation caused by a similar mechanism where a soldier carrying a folded stretcher as part of his assigned military gear incurred bilateral anterior glenohumeral dislocations when the gear was dismounted.
CASE REPORT
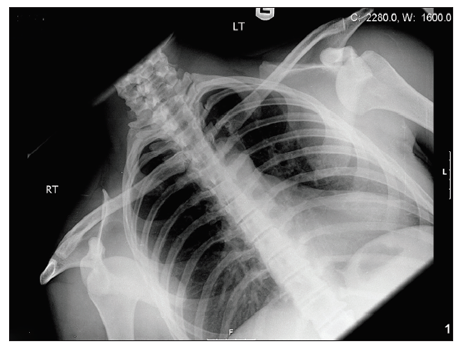
A 19-year-old soldier, in the Israeli Defense Forces paratrooper core, had been at the end of a strenuous drill, carrying a stretcher and gear for a distance exceeding 20 km. While dismounting the stretcher, the patient hyperextended his humeri in the mid-abducted position, pivoting their heads out of their sockets. The soldier relayed that the stretcher which was part of his assigned gear was dismounted forcefully by a fellow soldier who pulled the folded stretcher back while the carrying straps were still surrounding the arms. The patient had sudden pain and disability. He was evacuated to the emergency department where an X-ray was performed [Figure 1] depicting bilateral shoulder dislocation.
The closed reduction under sedation was performed using traction-counter traction technique, and no complications were observed. After 6 weeks in bilateral broad arm slings, with pendulum exercises from 2 weeks on, the patient started to mobilize his arms and achieved a full range of motion. The patient was later lost to follow-up and refused any intervention or treatment.
DISCUSSION
For simultaneous bilateral dislocation of the glenohumeral joints to occur, forces of similar magnitude and direction must act on both joints. The mechanism initially proposed by Jones in 1987 [7] and later corroborated by Cresswell and Smith in 1998 [8] of slow levering of the arms on the edges of a bench press may take effect in our case as the stretcher carrying mount may act as the "bench" in this case, whereas the straps pulling on the anterior aspect of the elbows may allow for the pivoting force otherwise emanating from the free weights bar. Felderman et al [5]. reported bilateral anterior shoulder dislocation following a chin-up exercise in a 44-year-old woman. We believe this mechanism to be somewhat similar to that described but would suggest that it be difficult to conceive such a mechanism causing frank dislocation in a healthy young male with stable glenohumeral joints.
In this case, we believe the stretcher mount structure contributed to the injury itself. Both arms pivoted on the mount while the tugging on the tightened straps across the antecubital fossae acted to dislocate both glenohumeral joints. It may be postulated that the physical exhaustion, combined with sleep deprivation, further allowed for the bilateral hyperextension in mid-abduction and the eventual bilateral shoulder dislocation. The authors believe that when dismounting heavy or large gear strapped to the back care should be instituted so as to avoid hyperabduction of the arms. In extreme cases and specifically within elite unit cores, assisted dismounting of gear should be performed cautiously and responsibly.
REFERENCES
- Litchfield JC, Subhedar VY, Beevers DG, Patel HT. Bilateral dislocation of the shoulders due to nocturnal hypoglycemia.b Postgrad Med J 1988;64:450-2.
- Brown RJ. Bilateral dislocation of the shoulder. Injury 1984;15:267-73.
- Carew-McColl M. Bilateral shoulder dislocation caused by electric shock. Br J Clin Pract 1980;34:251.
- Maffuli N, Mikhail HM. Bilateral anterior glenohumeral dislocation in a weight lifter. Injury 1990;21:254-6.
- Felderman H, Shih R, Maroun V. Chin-up-induced bilateral anterior shoulder dislocation: A case report. J Emerg Med 2009;37:400-2.
- Ozcelik A, Dincer M, Cetinkanat H. Recurrent bilateral dislocation of the shoulders due to nocturnal hypoglycemia: A case report. Diabetes Res Clin Pract 2006;71:353-5.
- Jones MA. Case of bilateral shoulder dislocation (letter). Br J Sports Med 1987;21:139.
- Cresswell TR, Smith RB. Bilateral anterior shoulder dislocations in bench pressing: An unusual cause. Br J Sports Med 1998;32:71-2.