A Rare Case of a Common Condition: Peroneum OS Fracture Causing Lateral Foot Pain
Pratham Surya1, Saleem Mastan1, Anirudh Gaggil2
2.Foot and Ankle Consultant, Glangwili General Hospital, Dolgwili Rd, Carmarthen SA31 2AF, United Kingdom.
Citation: Surya P, Mastan S, Gaggil A. A Rare Case of a Common Condition: Peroneum OS Fracture Causing Lateral Foot Pain. Clin Res Orthop 2018;1(1):1-3.
Patients presenting with lateral foot pain may have a variety of pathologies. Fractures of the peroneum OS are rare and are not reported widely in the literature. Here, we report a case of a 43-year-old female who presented after a dorsiflexion-inversion injury while exercising the gym. Initial radiographs were thought of being unremarkable. Symptoms persisted, and on further presentation to our clinic, repeat radiographs showed a displaced fracture of the peroneum os. A retrospective examination of the initial radiographs showed a subtle undisplaced fracture of the peroneum os. The patient underwent excision of the proximal half of the peroneum os with reconstruction of the peroneus longus, with an uneventful post-operative phase.
Lateral foot pain, Peroneum Os fracture, Peroneus longus tear.
INTRODUCTION
The os peroneum is a sesamoid bone found in the substance of peroneus longus tendon. Pathologies of os peroneum present as lateral foot pain is often overlooked. The term painful os peroneum syndrome was first coined by Sobel et al.[1] in 1994. These painful conditions can often be acute or chronic. The acute condition can include fractures which can lead to the discontinuity of the peroneus longus tendon. The chronic conditions may include non-union of os peroneum fractures, tenosynovitis, partial rupture, and subluxation of the peroneus longus tendon and can lead to degenerative changes of the pseudoarticulation between cuboid and os peroneum [2].
X-rays are the first line of imaging that should be obtained. The fracture is better identified in an oblique view of the foot [3]. Radiology has shown that when the os peroneum fragment is separated by 6 mm, it is often associated with a full-thicknedd peroneus longus tendon tear. However, when the fragment is separated by only 2 mm or less, it is associated with a partial thickness tear [4]. It may sometimes difficult to distinguish the acute fractures from bipartite os peroneum.
Radiologically, the bipartite os peroneum has smooth edges and sclerotic margins [4].
Ultrasound can be used to diagnose the chronic pathologies as it can evaluate the location, morphology, and echogenicity of the peroneal tendons throughout the entire course of the tendons [5,6].
Magnetic resonance imaging (MRI) scans are an excellent modality in identifying the acute os peroneal fractures as on 20% of the os peroneum is ossified [7] that can be picked up in the X-rays. It can also show the extent of peroneus longus tears.
The operative management includes fixation fracture if possible, excision of the ossicle with either repair of the peroneus longus tendon or tenodesis to peroneus brevis. Some studies recommend surgical treatment in active patients due to concern for incompetence of the peroneus longus tendon, associated loss of eversion strength, and first metatarsal plantar flexion strength [8].
The purpose of this case report was to show the importance of recognizing the os peroneal fracture in the early stages in an inversion injury to the foot, as delays in diagnosis can lead to complications.
CASE REPORT
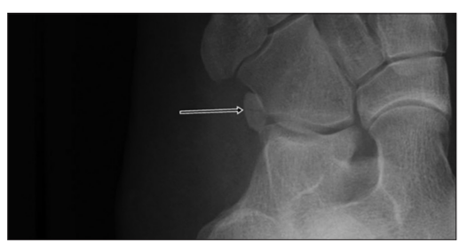
A 43-year female had a dorsiflexion-inversion injury to her left foot on November 27, 2012 while exercising in the gym. She came to casualty on that day with complaints of pain in her lateral aspect of her left foot. On examination, there was tenderness over lateral side of the cuboid bone and rest of the examination was unremarkable [Figure 1]. X-ray was done and was reported to be normal. However, looking at the X-ray's closely, there is an undisplaced fracture of the left os peroneum that was missed [Figure 2].
She then continued hobbling on the foot as she was told that she had no fracture, but on December 05, 2012, she sustained a further severe inversion injury to her left foot. After this, she was unable to weight bear on her left foot; hence, she came to casualty where X-ray was done which showed completely displaced # of os peroneum of 2 cm [Figure 3]. She also had an MRI done which showed complete rupture of left peroneus longus tendon.


On January 23, 2013, she underwent surgery for reconstruction of peroneus longus with excision of proximal half of os peroneum as distal fragment was too deep to be excised. Post-operative period was uneventful and the patient was discharged home with below knee POP with the left foot immobilized in eversion.
DISCUSSION
The os peroneum fractures are a rare type of fracture. They require great clinical acumen to be identified. This is the case as these fractures present with non-specific symptoms and there are several conditions, which present similarly. Typically, patients complain of pain on the lateral aspect of the foot. They can also present with swelling, bruising, and difficulty in fully weight-bearing. On examination, there can be tenderness and bruising over the lateral aspect of the foot over the calcaneocuboid joint. It is vital to note in this case report that the patient only complained of pain and there was no bruising or swelling.
From limited case reports and case series, the treatment of the fracture can be conservative or surgical. The conservative management includes short period of immobilization with protected weight bear and physiotherapy. Smith et al [9]. reported a case of os peroneum fracture in a high-level athlete which was managed conservatively. The fracture was minimally displaced and was managed with walking boot with 2 weeks of non-weight-bearing. After 2 weeks, physiotherapy was started with light jogging and returned to playing tennis in 8 weeks of time. After 2 months, the patient returned to full competitive tennis with any residual symptoms.
X-ray is the first line of investigation; however, only 20% of os peroneum are ossified. Consequently, majority of fractures would be missed. Therefore, MRI is the gold standard as they pick the acute fractures and also show the extent of peroneus longus tears. It is imperative to pick these fractures early as if left untreated it can result in the rupture of the peroneus longus as seen in this case.
Undisplaced fractures can even be managed non-operatively with short period of immobilization with protected weight bear and physiotherapy.
Surgical management include fixation of the fracture if possible, excision of the ossicle with either repair of the peroneus longus tendon or tenodesis to peroneus brevis. As seen with this case, the patient required repair of the peroneus longus tendon. Had the fracture been detected on X-ray, surgery may have been avoided and the fracture managed non-operatively. This reiterates the importance to have a clinical suspicion of os peroneum fracture in inversion injuries of the foot with lateral foot pain. Furthermore, to remember that X-rays can miss majority of these fractures, and MRI is the best imaging modality available.
REFERENCES
- Sobel M, Pavlov H, Geppert MJ, Thompson FM, DiCarlo EF, Davis WH. Painful os peroneum syndrome: A spectrum of conditions responsible for plantar lateral foot pain. Foot Ankle Int 1994;15:112-24.
- Gokkus K, Sagtas E, Demirci E, Saylik M, Aydin AT. Degenerative arthritis of pseudo articulation between the os peroneum and cuboid: A rare cause of lateral foot pain. Foot Ankle Surg 2015;21:e9-11.
- Chagas-Neto FA, de Souza BN, Nogueira-Barbosa MH. Painful os peroneum syndrome: Underdiagnosed condition in the lateral mid foot pain. Case Rep Radiol 2016;2016:8739362.
- Brigido MK, Fessell DP, Jacobson JA, Widman DS, Craig JG, et al. Radiography and US of os peroneum fractures and associated peroneal tendon injuries: Initial experience. Radiology 2005;237:235-41.
- Bianchi S, Abdelwahab IF, Tegaldo G. Fracture and posterior dislocation of the os peroneum associated with rupture of the peroneus longus tendon. Can Assoc Radiol J 1991;42:340-4.
- Vethanayagamony T, Patel H, Lomasney LM, Demos TC, Rottier FJ. Migration of the os peroneum associated with rupture of the peroneus longus tendon. Orthopedics 2013;36:741, 807-10.
- Sarrafian SK, editor. Osteology. In: Anatomy of the Foot and Ankle. Philadelphia, PA: JB Lippincott; 1983. p. 35-106.
- Sammarco VJ, Cuttica DJ, Sammarco GJ. Lasso stitch with peroneal retinactuloplasty for repair of fractured os peroneum: A report of two cases. Clin Orthop Relat Res 2010;468:1012-7.
- Smith JT, Johnson AH, Heckman JD. Non operative treatment of an os peroneum fracture in a high-level athlete: A case report. Clin Orthop Relat Res 2011;469:1498-501.