Blastocystis Hominis Among Pediatric Patients in a Tertiary Hospital in United Arab Emirates
Noura Jasim1, Salwa Al Kaabi2, Aysha Al Kaabi2, Hossam Al-Tatari3
2. Department of Pediatric, Division of General Pediatrics, Tawam Hospital, Al Ain, UAE.
3. Department of Pediatric, Division of Pediatric Infectious Diseases, Tawam Hospital, Al Ain, UAE
Citation : Jasim N, Al Kaabi S, Al Kaabi A, Al-Tatari H. Blastocystis Hominis Among Pediatric Patients in a Tertiary Hospital in United Arab Emirates. Clin Res Pediatr 2018;1(1):1-4.
Blastocystis hominis (Bh) is an intestinal protozoan that is reported among all age groups. However, it is not
clear if it is an enteropathogen and if it should be treated among symptomatic immunocompetent patients.
The
objective of the study was to describe the clinical manifestations and management of Bh among pediatric patients seen in a
tertiary hospital (Tawam Hospital) in Al-Ain city, United Arab Emirates.
A retrospective chart review of 27 patients
with confirmed Bh infection between the ages of 6 months and 15 years who attended Tawam Hospital from January 2010 to
December 2017.
Bh alone was isolated in stool specimens of 27 patients most of whom were males 15/27 (55.6%).
The most common presenting symptoms were diarrhea in 9/27 (33%) patients and abdominal pain in 18/27 (66.7%). The
illness duration was 7 days or less in 15/27 (55.6%). Only 2/27 patients (7.4%) received metronidazole, while the rest improved
spontaneously. 10 patients had coinfection with a different organism. Their course of illness and management seemed to be
slightly different.
The vast majority of our patients improved spontaneously suggesting that supportive treatment
may be sufficient in case of acute infections among immunocompetent patients. However, it is recommended to look for Bh
among patients presenting with chronic abdominal symptoms. It is reasonable to consider antimicrobial therapy in such patients
while observation is recommended on otherwise healthy patients with the acute presentation.
Abdominal pain, Blastocystis hominis, diarrhea, metronidazole, trimethoprim-sulfamethoxazole, vomiting
INTRODUCTION
Blastocystis hominis (Bh) is an intestinal protozoan [1] that is known as the most common intestinal parasite. It is found in humans and a wide range of animal's stool specimens, including mammals, birds, reptiles, and arthropods [2,3]. It has been isolated from patients present with abdominal pain, vomiting, diarrhea (which could be alternating with constipation), fever, and weight loss [4]. However, Bh remained a highly controversial protozoan parasite since it has been regarded as a commensal by some and a pathogen by others. Scientists have wondered whether it is truly an enteropathogen since spontaneous recovery has been reported among most symptomatic immunocompetent patients [5].
The parasite has a worldwide distribution with human prevalence ranging from 2% to 30% in some regions. The prevalence is higher in developing countries compared to developed countries due to poor hygiene, and consumption of contaminated food or water [6]. A recent study showed that 100% of people from low socioeconomic villages in Senegal were infected with Blastocystis species suggesting that transmission was increased due to poor hygiene sanitation, close contact with domestic animals and livestock, and having the water supply directly from well and river [6].
METHODS
A retrospective chart review of 27 patients with confirmed Bh infection between the ages of 6 months and 15 years who attended Tawam Hospital from January 2010 to December 2017. Tawam Hospital is a major tertiary care hospital in the United Arab Emirates with a total of 150 dedicated acute pediatric beds divided between general and subspecialty pediatrics, pediatric surgery, neonatal intensive care, pediatric intensive care, and hematology/oncology wards. The hospital is located in Al-Ain city which is one of the major cities in Al-Ain with high socioeconomical status and easy access to clean water. The clinical features and management of patients, in whom Bh was isolated alone or in conjunction with other organisms was reviewed.
RESULTS
Bh was isolated from stool specimens of 37 patients during the study period. Bh was the only pathogen in 27 patients while it was isolated in conjunction with other protozoa such as Giardia and Endolimax nana and other bacteria such as Salmonella species and Campylobacter jejuni in 10 more cases.
Among the patients who had Bh as a single pathogen, 12/27 (44.4%) of the cases were females, and 15/27 (55.6%) were males suggesting a slight male predominance. 2/27 (7.4%) patient had low-grade subjective fever reported at presentation, but none had a documented fever during the clinical encounters. 9/27 (33%) patients presented with diarrhea and only one of them had bloody diarrhea. 18/27 (66.7%) patients complained of abdominal pain at the time of presentation, and only two of them had nausea and vomiting. The duration of illness varied, but it was 7 days or less in 15/27 (55.6%). Only one patient had symptoms for 2 weeks, and two other patients had symptoms lasting for 2 months. Unfortunately, there was no clear documentation regarding the length of illness in the remaining 9 patients. In terms of therapy, only two patients received metronidazole; one patient received triple therapy (Metronidazole, Amoxicillin, and Omeprazole); while the rest of the patients had spontaneous resolution without any antimicrobials. None of the patients required hospitalization or developed complications on follow-up.
Basic blood investigations were obtained in all the 27 patients. All had normal electrolytes except for one patient who had mild hypokalemia of 3.1 mmol/dl. All patients had normal BUN and creatinine, white blood cell counts, hemoglobin levels, and blood sugar levels. However, some of them had abnormal platelet counts at the time of presentation: 3/27 (11%) had mild thrombocytosis ranging between 458 and 536, and one patient had thrombocytopenia of 30. All blood cultures were negative.
DISCUSSION
There is an ongoing debate over the pathogenicity of Bh, with some experts believing that it is pathogenic while others argue strongly against that [7]. Therefore, there is still no agreement on whether it should be treated or not. Those who believe in its pathogenicity have tried several therapeutic options. Nassir et al. and Valsecchi et al. reported successful therapy with Metronidazole [8,9]. Other experts such as Pasqui et al. used Metronidazole in combination with other antimicrobials such as Paromomycin or Trimethoprim-Sulfamethoxazole (TMP-SMX) [10].
Tan et al. suggested that only patient with chronic abdominal pain and diarrhea that cannot be explained by any other pathology should be considered for antimicrobial therapy[11] While Metronidazole has historically been the drug of choice, Bh resistance to this agent seems to be in the rise[12,13] Other agents to be considered include TMPSMX [14], in addition to Nitazoxanide, Emetine, Furazolidone, Iodochlorhydroxyquin, and Pentamidine [15].
The vast majority of our patients resolved without therapy. Only two of our patients received Metronidazole therapy. In addition, 12 years-old boy received triple therapy (Metronidazole, Amoxicillin, and Omeprazole) for presumed Helicobacter pylori infection. Due to the retrospective nature of the study, it is hard to judge if this treatment resulted in prompt recovery or they recovered spontaneously just like the rest of our patient cohort.
Ten patients were excluded from the above analysis since they had coinfection with another organism as detailed in Table 1.
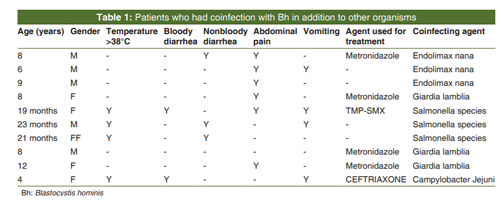
Unlike isolated Bh infections, all the patients who had coinfection with a bacterial pathogen were febrile at the time of presentation. Patients with coinfections were more likely to have diarrhea (5/10 or 50%) and vomiting (4/10 or 40%). They were also more likely to receive antimicrobial therapy. Whether the presence of Bh was coincidental in those cases, or it created an inflamed environment that made the intestine more amenable to infections, is not clear. The coinfection with Endolimax nana, however, is of special interest since it has been recognized as a cause of chronic diarrhea in immunocompetent patients [16,17].
Two of our patients had prolonged symptoms ranging between 2 and 6 months. They were a 12 years-old boy and an 8 years-old girl. Both had documented family medical history of irritable bowel syndrome (IBS). There has been increasing interest over the past few years in studying the prevalence of Bh infections, and its possible relations to IBS. Because Bh causes symptoms that are similar to those attributed to IBS such as diarrhea, abdominal pains, cramps, and nausea; it is logical to assume the association of this parasite and IBS. It is also possible that the change in the environment in the intestine caused by IBS may allow for the conditions favored by Bh. Alternatively, it has been proposed that a possible mechanism for the IBS-like symptoms might be the low-grade inflammation through persistent antigenic exposure in a chronic Bh infection [7,18,19].
Finally, although the isolated parasite was reported in all of our cases as Bh, this has not been confirmed by genetic studies at the time. Although Tan and Suresh suggested that clinical manifestation could be type dependent [20], more recent studies suggested that there are no specific pathogenic or nonpathogenic species of Blastocystis; and that the clinical course could be modified by the patient's underlying condition rather than the infecting species [21]. Therefore, we believe that it would be prudent to include genetic studies to properly identify the subspecies in any future prospective studies, and hence verify if one species is more pathogenic than the others.
CONCLUSION
Despite having a high socioeconomical standard and easy access to clear water, Bh seems to be not a rare infection in the United Arab Emirates among children. Due to the retrospective nature of our study and the lack of surveillance system, we believe that the numbers in our study could be an underestimate of the real prevalence of this parasite in our community.
The vast majority of our patients improved spontaneously. However, we recommend to look for Bh among patients presenting with chronic abdominal symptoms. More prospective studies are needed to look at the prevalence of this parasite mainly among patients with chronic intestinal disorders, and whether antimicrobial therapy would be of real value in such cases. However, and until such studies are conducted, we believe a trial of an active agent such as Trimethoprim-Sulfamethoxazole or Nitazoxanide may be reasonable in such cases. Otherwise supportive treatment without antimicrobial therapy is recommended in otherwise healthy patients with the acute presentation.
References
- Abdulsalam AM, Ithoi I, Al-Mekhlafi HM, Ahmed A, Surin J, Mak JW. Drinking water is a significant predictor of Blastocystis infection among rural Malaysian primary school children. Parasitology 2012;139:1014-20.
- Leelayoova S, Siripattanapipong S, Thathaisong U, Naaglor T, Taamasri P, Piyaraj P, et al. Drinking water: A possible source of Blastocystis Spp. Subtype 1 infection in school children of a rural community in Central Thailand. Am J Trop Med Hyg 2008;79:401-6.
- Eroglu F, Koltas IS. Evaluation of the transmission mode of Blastocystis hominis by using PCR method. Parasitol Res 2010;107:841-5.
- Behera HS, Srigyan D, Gupta M. A dilemma for Blastocystis: Asymptomatic or symptomatic infection in humans. EC Microbiol 2017;8.5:246-51.
- Farthing MJ. Treatment options for the eradication of intestinal protozoa. Nat Clin Pract Gastroenterol Hepatol 2006;3:436-45.
- Safadi DE, Gaayeb L, Meloni D, Cian A, Poirier P, Wawrzyniak I, et al. Children of Senegal river basin show the highest prevalence of Blastocystis sp. Ever observed worldwide. BMC Infect Dis 2014;14:164.
- Stark D, van Hal S, Marriott D, Ellis J, Harkness J. Irritable bowel syndrome: A review on the role of intestinal Protozoa and the importance of their detection and diagnosis. Int J Parasitol 2007;37:11-20.
- Nassir E, Awad J, Abel AB, Khoury J, Shay M, Lejbkowicz F. Blastocystis hominis as a cause of hypoalbuminemia and anasarca. Eur J Clin Microbiol Infect Dis 2004;23:399-402.
- Valsecchi R, Leghissa P, Greco V. Cutaneous lesions in Blastocystis hominis infection. Acta Derm Venereol 2004;84:322-3.
- Pasqui AL, Savini E, Saletti M, Guzzo C, Puccetti L, Auteri A. Chronic urticaria and Blastocystis hominis infection: A case report. Eur Rev Med Pharmacol Sci 2004;8:117-20.
- Tan KS. New insights on classification, identification, and clinical relevance of Blastocystis spp. Clin Microbiol Rev 2008;21:639-65.
- Yakoob J, Jafri W, Jafri N, Islam M, Asim Beg M. In vitro susceptibility of Blastocystis hominis isolated from patients with irritable bowel syndrome. Br J Biomed Sci 2004;61:75-7.
- Haresh K, Suresh K, Anus AK, Saminathan S. Isolate resistance of Blastocystis hominis to metronidazole. Trop Med Int Health 1999;4:274-7.
- Moghaddam DD, Ghadirian E, Azami M. Blastocystis hominis and the evaluation of efficacy of metronidazole and trimethoprim/sulfamethoxazole. Parasitol Res 2005;96:273-5.
- Sekar U, Shanthi M. Blastocystis: Consensus of treatment and controversies. Trop Parasitol 2013;3:35-9.
- Graczyk TK, Shiff CK, Tamang L, Munsaka F, Beitin AM, Moss WJ. The association of Blastocystis hominis and Endolimax nana with diarrheal stools in Zambian school-age children. Parasitol Res 2005;98:38-43.
- Shah M, Tan CB, Rajan D, Ahmed S, Subramani K, Rizvon K, et al. Blastocystis hominis and Endolimax nana co-infection resulting in chronic diarrhea in an immunocompetent male. Case Rep Gastroenterol 2012;6:358-64.
- Tungtrongchitr A, Manatsathit S, Kositchaiwat C, Ongrotchanakun J, Munkong N, Chinabutr P, et al. Blastocystis hominis infection in irritable bowel syndrome patients. Southeast Asian. J Trop Med Public Health 2004;35:705-10.
- Yakoob J, Jafri W, Beg MA, Abbas Z, Naz S, Islam M, et al. Blastocystis hominis and Dientamoeba fragilis in patients fulfilling irritable bowel syndrome criteria. Parasitol Res 2010;107:679-84.
- Tan TC, Suresh KG. Predominance of amoeboid forms of Blastocystis hominis in isolates from symptomatic patients. Parasitol Res 2006;98:189-93.
- Stensvold CR, Lewis HC, Hammerum AM, Porsbo LJ, Nielsen SS, Olsen KE, et al. Blastocystis: Unravelling potential risk factors and clinical significance of a common but neglected parasite. Epidemiol Infect 2009;137:1655-63.