Prolonged use of Furosemide in Pediatrics
Luiz Antonio Del Ciampo1, Ieda Regina Lopes Del Ciampo2
2. Medical Epidemiologist, Master Pediatric Palliative Care, Pediatric Intensive Care Resident, Universidad de Santander, Bucaramanga, Colombia.
Citation : Zarate Vergara AC, Tirado Perez IS. Prolonged use of Furosemide in Pediatrics. Clin Res Pediatr 2018;1(1):1-4..
One of the main diuretics used in pediatric intensive care units is furosemide, which acts on the loop of Henle, causing an
increase in urinary flow and electrolyte excretion. It has multiple uses in the pediatric age, being used in chronic pulmonary,
renal, and cardiovascular pathologies, among other uses. However, its prolonged use can cause different effects from electrolyte
imbalances such as hypokalemia, hypomagnesemia, hypercalcemia, alterations of the base acid state, and nephrolithiasis to
ototoxicity.
Adverse effects, furosemide, pediatric
INTRODUCTION
Furosemide is the most used diuretic in neonatal and pediatric intensive care[1]-3], belongs to the sulfonamide group, and acts by blocking the Na + -K + -2Cl cotransporter in the ascending branch of the Henle loop increasing the urinary excretion of these electrolytes[4,5]. It is widely used for bronchopulmonary dysplasia, water overload, renal dysfunction, heart failure, and post-operative management of cardiovascular surgery [6-9].
Its prolonged use is associated with electrolyte abnormalities such as hypocalcemia, hypomagnesemia, metabolic alkalosis, and hypercalciuria is also described, which increases the risk of developing nephrocalcinosis and renal lithiasis, which has been observed more frequently in low birth weight and premature neonates. They required furosemide [10].
Other effects described in addition to the time of use and high accumulated doses, especially when administered intravenously is the ototoxicity generally irreversible, causing alterations in hearing such as tinnitus, hearing loss, vertigo, and deafness, increasing the risk when associated with drugs such as aminoglycosides[4,11,12]. In this article, an updated and careful review of the published medical literature is made on the adverse effects and recommendations for the prevention of these.
USE OF FUROSEMIDE Electrolyte fluid disorders
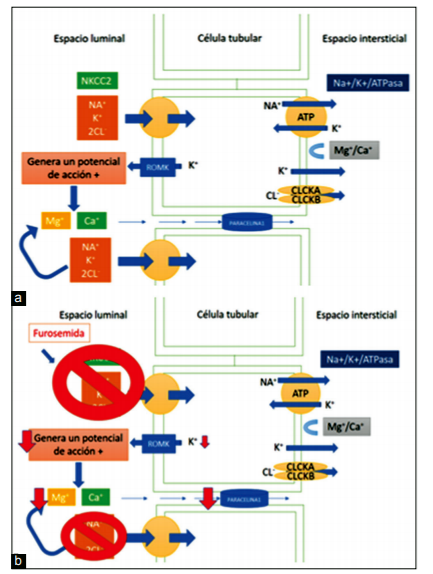
The mechanism of action of furosemide is to inhibit the Na + / K + / 2 Cl, significantly increasing the urinary excretion of Na + and Cl-, but also causes an increase in the excretion of calcium and magnesium due to the alteration in the transepithelial potential difference, the mechanism of action in two situations is explained in Figure 1. It can be explained how in excessive amounts of prolonged diuretic use can lead to alterations in the balance and electrolytes with depletion of water, which can be manifested with hypotension due to the depletion of volume of extracellular fluid, hyponatremia, hypomagnesemia, hypocalcemia, and hypokalemia[5,13,14]. The increase in the release of Na + toward the distal tubule and proximal tubule, triggers an increase in urinary excretion of K + and H +, which produces a metabolic alkalosis and hypokalemia[5], which causes a pseudo-Bartter syndrome giving hypomagnesemia symptoms, hypocalcemia, and persistent metabolic alkalosis as in the case described [15].
Figure 1: Explains the normal mechanism and mechanism during prolonged use of furosemide. (a) The mechanism of action is to inhibit the Na + / K + / 2 Cl, increasing the urinary excretion of Na +, Cl-, Ca and Mg due to alteration in the transepithelial potential difference, the reabsorption of calcium occurs by passive transport of the gradient created by NaCl. (b) His inhibiting causes a decrease in the reabsorption of calcium, magnesium reabsorption is also affected since it also uses a passive transport mechanism through a common paracellular pore, therefore, in excessive quantities or use of the diuretic can lead to alterations in the balance of electrolytes.
The exhaustion of magnesium plays a very important role, this is important in the enzymatic reaction, in energy-producing metabolism, and in protein synthesis, and membrane transport. Depletion of magnesium plays a role very important, by the enzymatic reaction in the production of energy metabolism and synthesis and membrane protein transport. The main site of reabsorption of magnesium is a renal level in the loop of Henle in 70-80%, which affects prefaced using furosemide decreasing intracellular magnesium and excessive loss in the urine to hypomagnesemia causing, for example, the myocardial involvement with arrhythmias such as atrial fibrillation[14,16-19].
Magnesium and calcium are reabsorbed paracellularly creating tight junctions known as paracelin-1 or claudin1. In the distal tubule, resorption is described by an active mechanism using the TRPM67 magnesium channel, while the active mechanism in the thick loop of Henle and distal tubule is unknown, thought to be driven by the electrochemical gradient of the Na +/K + -ATPase pump when the magnesium reabsorption is inhibited, the potassium channels are reversibly inhibited by altering the NKCC2 cotransporter and in the production of the electric gradient generated with the potassium exit Figure 1b[20].
Nephrolithiasis also this diuretic use is related to the formation of nephrolithiasis is urolithiasis or nephrocalcinosis, secondary to given hypercalciuria cations Ca 2 + is reabsorbed in the loop of Henle by passive mechanisms of transport of chloride sodium. Nephrocalcinosis refers to calcium deposits in the kidney tissue, can be spinal cord, cortical or diffuse, and histologically intratubular and interstitial, and was described for the 1st time in 1982 in premature patients with prolonged use of furosemide; the rate of prevalence ranges between 7 and 64% in premature with low weight for gestational age[21-23]. He is explained by their renal immaturity that facilitates the retention of the crystal and its low rate of glomerular filtration. In premature patients who used cumulative dose of furosemide 10 mg/kg may increase the risk of nephrocalcinosis up to 48 times more, and in some studies, this is considered the factor with greater risk for nephrocalcinosis[21,24-26].
Andrioli et al. conducted a retrospective study of patients under 1 year of age with renal lithiasis and nephrocalcinosis, where they evaluated their follow-up, 44% of these patients had received furosemide, 22% corresponded to nephrocalcinosis, and found that 37% of these cases diagnosed patients presented renal lithiasis in their evolution[27]. Other studies of nephrocalcinosis follow-up in children have shown a spontaneous resolution, establishing that around 57.1% of patients with premature nephrocalcinosis at 1 year had spontaneous resolution[24,25].
Furosemide is part of the most common drugs that produce ototoxicity; this occurs because the transporter Na K 2Cl, also present in marginal cells and stria vascularis, leads to inhibition of potassium reabsorption and decreased endocochlear potential, and usually, its affectation is bilateral and usually reversible, although permanent damage has been described. High doses of furosemide, prolonged treatment, and intravenous administration increase this risk, it has also been described that when it is administered with drugs such as aminoglycoside-type antibiotics the toxicity synergy increases[28-31].
For its prevention of these effects with the use of furosemide, it has been described that low initial dose should be used until achieving an adequate fluid balance and urine production between 1 and 3 ml/kg/h, and not to exceed cumulative dose of 10 mg/kg[32,33].
Gulbis and Spencer conducted a systematic review, evaluating the efficacy of continuous intravenous furosemide, and found that this form of administration maintained a sustained diuresis unlike intravenous furosemide administered intermittently after cardiovascular surgery[34], other studies also support use in cardiovascular pathologies, the use of furosemide infusion continues on intermittent use, as advantage shown diuresis steadily but described side effects as the disorder of the electrolytes and long-term deterioration of renal function; so it is recommended for use only in unstable patients to maintain a restricted use[35-40].
In our case, we can observe that I present as adverse effects to this loop diuretic, electrolyte disorders, which could be due to the initiation of continuous intravenous furosemide in its postsurgical or prolonged use of it later, requiring corrections in electrolytes daily in your stay at pediatric intensive care; it is common that these electrolyte disorders lead us to other pathologies and especially in our pediatric population to pathologies of genetic origin such as Bartter syndrome, which is why it is important to know about the adverse effects of drugs used, for their prevention and proper use.
CONCLUSIONS
Compression toxicities and electrolyte disturbances secondary to loop diuretics like furosemide are a neglected subject, by which you want to show because the prolonged use of this medication must be especially careful, you should create awareness that the use of diuretics requires a careful use, take into account time of use, dosage, avoiding high doses, to reduce doses toxic and high concentrations in addition to take into account that the therapy long-term power all adverse effects.
References
- Clark RH, Bloom BT, Spitzer AR, Gerstmann DR. Reported medication use in the neonatal intensive care unit: Data from a large national data set. Pediatrics 2006;117:1979-87.
- Hsieh EM, Hornik CP, Clark RH, Laughon MM, Benjamin DK, Smith PB. Medication use in the neonatal intensive care unit. Am J Perinatol 2014;31:811-22.
- Favia I, Garisto C, Rossi E, Picardo S, Ricci Z. Fluid management in pediatric intensive care. Contrib Nephrol 2010;164:217-26.
- Pacifici GM. Clinical pharmacology of furosemide in neonates: A review. Pharmaceuticals 2013;6:1094-129.
- Reilly RF, Jackson EK. Regulation of renal function and vascular volume. In: Goodman and Gilman's the Pharmacological Basis of herapeutics. 20th ed. New York: McGraw-Hill Education; 2011. p. 682-6.
- Slaughter JL, Stenger MR, Reagan PB. Variation in the use of diuretic therapy for infants with bronchopulmonary dysplasia. Pediatrics 2013;131:716-23.
- Laughon MM, Chantala K, Aliaga S, Herring AH, Hornik CP, Hughes R, et al. Diuretic exposure in premature infants from 1997 to 2011. Am J Perinatol 2015;32:49-56.
- Segar JL. Neonatal diuretic therapy: Furosemide, thiazides, and spironolactone. Clin Perinatol 2012;39:209-20.
- Moffett BS, Price JF. National prescribing trends for heart failure medications in children. Congenit Heart Dis 2015;10:78-85.
- Girardi A, Raschi E, Galletti S, Poluzzi E, Faldella G, Allegaert K, et al. Drug-induced renal damage in preterm neonates: State of the art and methods for early detection. Drug Saf 2015;38:535-51.
- Robertson CM, Tyebkhan JM, Peliowski A, Etches PC, Cheung PY. Ototoxic drugs and sensorineural hearing loss following severe neonatal respiratory failure. Acta Paediatr 2006;95:214-23.
- Stewart AL, Brion LP. Routine use of Diuretics in Very-low birth-weight Infants in the Absence of Supporting Evidence. Vol. 31. United States: Journal of Perinatology : Official Journal of the California Perinatal Association; 2011. p. 633-4.
- Dias CR, Leite HP, Nogueira PC, Brunow de Carvalho W. Ionized hypocalcemia is an early event and is associated with organ dysfunction in children admitted to the intensive care unit. J Crit Care 2013;28:810-5.
- Alexander RT, Dimke H. Effect of diuretics on renal tubular transport of calcium and magnesium. Am J Physiol Renal Physiol 2017;312:F998-1015.
- Bartoli E, Rossi L, Sola D, Castello L, Sainaghi PP, Smirne C. Use, misuse and abuse of diuretics. Eur J Intern Med 2017;39:9-17.
- Cohen N, Almoznino-Sarafian D, Zaidenstein R, Alon I, Gorelik O, Shteinshnaider M, et al. Serum magnesium aberrations in furosemide (frusemide) treated patients with congestive heart failure: Pathophysiological correlates and prognostic evaluation. Heart 2003;89:411-6.
- Wester PO. Electrolyte balance in heart failure and the role for magnesium ions. Am J Cardiol 1992;70:44C-9.
- al-Ghamdi SM, Cameron EC, Sutton RA. Magnesium deficiency: Pathophysiologic and clinical overview. Am J Kidney Dis 1994;24:737-52.
- Whang R, Hampton EM, Whang DD. Magnesium homeostasis and clinical disorders of magnesium deficiency. Ann Pharmacother 1994;28:220-6.
- Gonzalez EP, Rodriguez FS, Garcia EC. Magnesium homeostasis. Etiopathogeny, clinical diagnosis and treatment of hypomagnesaemia. A case study. Nefrologia (Madr.) 2009;29:518-24.
- Narter F, Narter F, Sarica K. Urinary stones in neonates: Dilemma between urolithiasis and nephrocalcinosis. J Urol Surg 2015;1:1-6.
- Hufnagle KG, Khan SN, Penn D, Cacciarelli A, Williams P. Renal calcifications: A complication of long-term furosemide therapy in preterm infants. Pediatrics 1982;70:360-3.
- Vervaet BA, Verhulst A, D'Haese PC, De Broe ME. Nephrocalcinosis: New insights into mechanisms and consequences. Nephrol Dial Transplant 2009;24:2030-5.
- Chang HY, Hsu CH, Tsai JD, Li ST, Hung HY, Kao HA, et al. Renal calcification in very low birth weight infants. Pediatr Neonatol 2011;52:145-9.
- Mohamed GB, Ibrahiem MA, Abdel Hameed WM. Nephrocalcinosis in pre-term neonates: A study of incidence and risk factors. Saudi J Kidney Dis Transpl 2014;25:326-32.
- Gimpel C, Krause A, Franck P, Krueger M, von Schnakenburg C. Exposure to furosemide as the strongest risk factor for nephrocalcinosis in preterm infants. Pediatr Int 2010;52:51-6.
- Andrioli V, Highmore K, Leonard MP, Guerra LA, Tang K, Vethamuthu J, et al. Infant nephrolithiasis and nephrocalcinosis: Natural history and predictors of surgical intervention. J Pediatr Urol 2017;13:355.e1-355.
- Girardi A, Raschi E, Galletti S, et al. Drug-Induced Renal Damage in Preterm Neonates: State of the Art and Methods for Early Detection. Drug Safety 2015;38:535-51.
- Humes HD. Insights into ototoxicity. Analogies to nephrotoxicity. Ann N Y Acad Sci 1999;884:15-8.
- Shine NP, Coates H. Systemic ototoxicity: A review. East Afr Med J 2005;82:536-9.
- Szczepek AJ. Ototoxicity: Old and new foes. In: Advances in Clinical Audiology. Department of ORL, Head and Neck Surgery, Charite University Hospital, Berlin, Germany. InTech; 2017.
- Miller JL, Thomas AN, Johnson PN. Use of continuous-infusion loop diuretics in critically ill children. Pharmacotherapy 2014;34:858-67.
- Buckley MS, Leblanc JM, Cawley MJ. Electrolyte disturbances associated with commonly prescribed medications in the intensive care unit. Crit Care Med 2010;38 6 Suppl:S253-64.
- Gulbis BE, Spencer AP. Efficacy and safety of a furosemide continuous infusion following cardiac surgery. Ann Pharmacother 2006;40:1797-803.
- Palazzuoli A, Pellegrini M, Ruocco G, Martini G, Franci B, Campagna MS, et al. Continuous versus bolus intermittent loop diuretic infusion in acutely decompensated heart failure: A prospective randomized trial. Crit Care 2014;18:R134-4.
- Amer M, Adomaityte J, Qayyum R. Continuous infusion versus intermittent bolus furosemide in ADHF: An updated meta-analysis of randomized control trials. J Hosp Med 2012;7:270-5.
- Pivac N, Rumboldt Z, Sardelic S, Bagatin J, Polic S, Ljutic D, et al. Diuretic effects of furosemide infusion versus bolus injection in congestive heart failure. Int J Clin Pharmacol Res 1998;18:121-8.
- Alsuhebany N, Aqel R, Alballa H, Al-Ayoubi F, Bawazeer G, Alhabib K, et al. 31. Differential effects of intravenous bolus furosemide and continuous furosemide infusion on in-hospital management and outcomes among patients admitted with acute decompensated heart failure. J Saudi Hear Assoc 2016;28:199-200.
- Allen LA, Turer AT, Dewald T, Stough WG, Cotter G, O'Connor CM. Continuous versus bolus dosing of furosemide for patients hospitalized for heart failure. Am J Cardiol 2010;105:1794-7.
- Caetano F, Mota P, Almeida I, Fernandes A, Botelho A, Leitao Marques A. Continuous infusion or bolus injection of loop diuretics for patients admitted for severe acute heart failure: Is one strategy better than the other? Rev Port Cardiol (English Ed) 2015;34:95-102.