Knowledge, Attitudes, and Practices of Parents of Children less than 5 Years towards Seasonal Malaria Chemoprevention in the Mokolo Health District, Cameroon
Andreas Chiabi1, Nelly Kamgaing2, Roger Ngueleodai Tchideme3, Norbert Tarla Njong3,Paul Koki4
2.Department of Pediatrics, Faculty of Medicine and Biomedical Sciences, University of Yaounde 1/ University Teaching Hospital, Yaounde, Cameroon.
3.Department of Pediatrics, Faculty of Medicine and Biomedical Sciences, University of Yaounde I,Cameroon.
4.Department of Pediatrics, Faculty of Medicine and Biomedical Sciences, University of Yaounde 1/The Mother and Child Center, Chantal Biya Foundation, Yaounde, Cameroon.
Citation : Chiabi A, Nelly Kamgaing N, Ngueleodai TR, Njong NT, Koki P. Knowledge, Attitudes, and Practices of Parents of Children less than 5 years towards Seasonal Malaria Chemoprevention in the Mokolo Health District, Cameroon. Clin Res Pediatr 2018;1(2):1-7.
Seasonal malaria chemoprevention strategy (SMC) was introduced in the northern regions of Cameroon in 2016.
The North and Far North regions of Cameroon, with a short seasonal transmission of malaria, record the highest morbidity and mortality rates in the country. We thus undertook this study to assess the knowledge, attitudes, and practices of mothers of under-five children toward this strategy in these regions.
A cross-sectional study was carried out from October 10, 2017, to May 31, 2018. A two-staged cluster sampling was carried out, and 450 mothers were included in the study. Data collection was done with the aid of a questionnaire administered to parents of children aged 3-59 months in the Mokolo health district. The degree of association was evaluated using the P-value with a significance threshold value of P ≤ 0.05 and odds ratio.
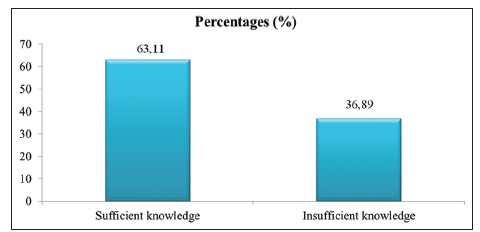
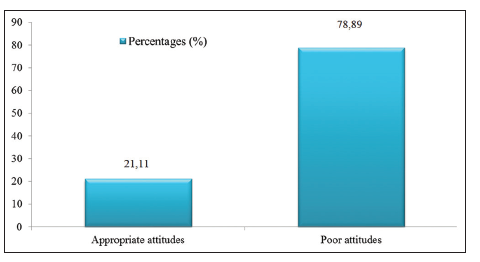
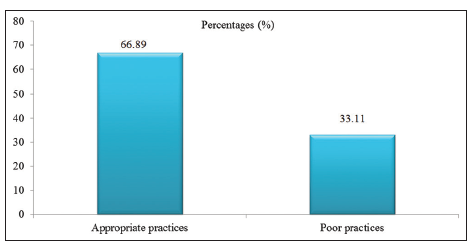
The average age of the parents was 31 years with a sex ratio of 0.71. 92.02% of parents were living as a couple, and 51.33% of the households had a low socioeconomic status. We noted that 63.11% of parents had satisfactory knowledge and 78.89% erroneous attitudes. Most of the parents (66.89%) had appropriate practices. Poor knowledge was associated with the liberal profession, low socioeconomic level, and living as a couple. Poor attitudes were associated with a primary level of education and low socioeconomic level, and poor practices were associated with the 35-45 years age group.
From our results, majority of parents had insufficient knowledge, erroneous attitudes, and inappropriate practices toward the SMC. We thus recommend that information, education, and communication of the population toward this strategy be reinforced.
Cameroon, knowledge, attitudes and practices, malaria, Northern regions, seasonal malaria chemoprevention.
INTRODUCTION
Malaria is a major public health concern in sub- Saharan Africa in general and particularly in Cameroon. Thus, in 2015, the National Malaria Control Program documented almost 2 million cases and 3500 deaths with 70% in children < 5 years [1]. Due to the seasonal transmission in the North and Far North regions, there is a peak in morbidity and mortality in these two regions during the three rainy season months (July-September). In 2015, 60% of malaria-related deaths in Cameroon were reported in this zone, and 50% were children under 5 years [2]. To curb this type of transmission, the World Health Organization since 2012 recommended the seasonal malaria chemoprevention (SMC) in children aged 3-59 months. This strategy consists of the monthly administration of a complete treatment with sulfadoxine-pyrimethamine (SP) and amodiaquine during the high malaria transmission season [3]. The NMPC adopted this strategy in the northern regions of Cameroon in 2016, and since then, no study has been carried out on this subject [1]. As with all community interventions, problems of adherence of the population might occur and are directly influenced by their perception toward the intervention. We thus carried out this study to assess the knowledge, attitudes, and practices of mothers of children aged 3-59 months on SMC in the health district of Mokollo in the Far North Region of Cameroon.
METHODS
This was an analytical cross-sectional study, carried out from October 10, 2017, to May 31, 2018, during the SMC campaign that took place from July to October 2017.
This study site was carried out in the Mokolo health district which is one of the 28 health districts in the Extreme North region. It extends through half of the Mayo-Tsanaga division (4393 km2). The climate is Soudano-Sahelian, with a long dry season of 9 months (October-June) and a short rainy season of 3 months (July-September) [1].
This health district is composed of 16 health areas: Gadala, Goudour, Ldamang, Magoumaz, Mandaka-Chechem, Minawao, Mokolo I, Mokolo II, Mokong, Moutaz, OuroTada, Toufou, Tourou, Vouzod, Zamay, and Zileng.
Sampling was done through a two-staged cluster sampling. In the first stage, random drawing without replacement of two villages in each health area was done, and in the second stage, random drawing without replacement of the direction to follow with respect to the four cardinal points in each village was done.
The sample size was obtained using the following formula:
N = 2X(P(1-P)(Zα/d)²),
where:
P = 85% is the SMC coverage in the northern regions in 2016;[4]
D = margin of error of 0.05 i.e., 5%;
Zα = 1, 96.
From this formula, a minimum sample size of 430 parents of children of 3-59 months was obtained.
Data collection was carried out with the aid of pre-tested questionnaires given to parents of children aged 3-59 months. Each questionnaire was made up of five main parts with a total of 48 opened and closed-ended questions with an average time of 25 min. The questions were divided as follows: Demographic characteristics (17 questions); knowledge (10 questions); attitudes (10 questions); practices (10 questions), and recommendations (1 question).
The socioeconomic level of homes was evaluated using three parameters: Level of education of family head; profession of family head, and monthly income of the family (FCFA). This score was inspired by studies done in India by Guru et al.[5].
The questionnaire was drawn up in the French language, but for reasons of comprehension, the questions were asked by the investigator in the local languages (Mafa, Foufoulde, Toupouri, etc.,) with the aid of a translator; the results in the local language were then translated into French and filled into a form.
We covered the 16 health areas in the Mokolo health district, following the procedure indicated above. We then proceeded from the residence of the SMC distributor, taking one compound out of two until the administration of 14 questionnaires per village. In cases where we did not have up to 14 homes in a given direction, another draw was done until 14 questionnaires had been filled. In a given direction, compounds without children or without parents were systematically skipped on to the next compound. In compounds having many homes with children aged 3-59 months, we systematically interviewed the parents of the youngest child. In each home, only one parent was interviewed, and if both parents were present, the one to be questioned was drawn by coin flip.
The data collected were entered on the CS PRO 6.3 software, and analysis done using the Statistical Package for the Social Science 21 software. The results were expressed in the form of totals, frequencies, averages, and standard deviations. The Chi-square test was used to determine the association between two variables.
The degree of association was evaluated using the P-value and odds ratio (OR), with a confidence interval of OR at 95% and significance threshold of P = 0.05.
Ethical clearance for our study was obtained from the Institutional Research Board of the Faculty of Medicine and Biomedical Sciences. We equally obtained administrative authorizations, and informed consent from each parent was interviewed. Each parent who took part in this study benefited from an information, education, and communication (IEC) session on SMC.
Data collected during this study were secured and were put into a database to which only the investigators had access.
RESULTS
A total of 462 parents were questioned among which 12 were excluded due to unfinished interviews and 450 were finally retained.
The average age of parents was 31 years ± 5.7 with extremes at 18 and 53 years, and the sex ratio was 0.71. Most of the parents (73.33%) were aged between 25 and 35 years, and 92.02% were living as a couple at the time of the survey. Most of them had a primary level of education (61.33%) and were practicing a liberal profession (89.11%), and more than half (51.33%) of the homes had a low socioeconomic level.
Of the 450 parents questioned, 64.00% could properly define SMC and 49.33% had a third party as a source of information. More than half of the parents knew the modalities for SMC (the target [58.44%]; the distribution site [59.11%]; and the distribution period [54.00%]). Meanwhile, less than a quarter of them knew the number of cycles per campaign (23.11%) and the campaign duration (24.22%). Most of the parents could state at least an advantage (65.78%), and an adverse effect (AE) (70.67%) of SMC [Figure 1].
Of the 450 parents who took part in the study, 53.55% thought that SMC was a curative measure against malaria and 73.78% thought that SMC was the best malaria control method and that the other methods should be abandoned. 90.44% were satisfied with the SMC, and 70.00% of them thought SMC was not harmful to children [Figure 2].
Of the 450 parents questioned, 92.67% gave four cycles of SMC to their children during the last campaign and 79.56% gave the 3 recommended doses. 54.67% of parents accepted to give SMC to their children because it was cheap, efficacious, and available at home. 54.83% of parents administered the medication on the 2nd and 3rd days by themselves, and 55.33% had a proper attitude toward handling adverse drug effects [Figure 3].
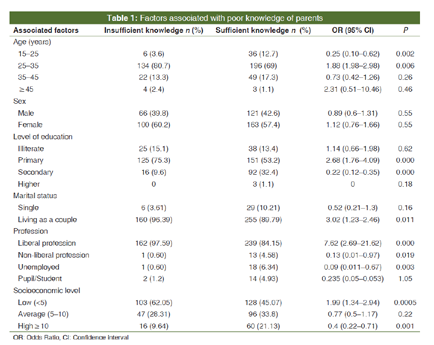
Among the factors analyzed, the 25-35 years of age group, primary level of education, living as a couple, the liberal profession, and low socioeconomic level were associated to poor knowledge of parents [Table 1].
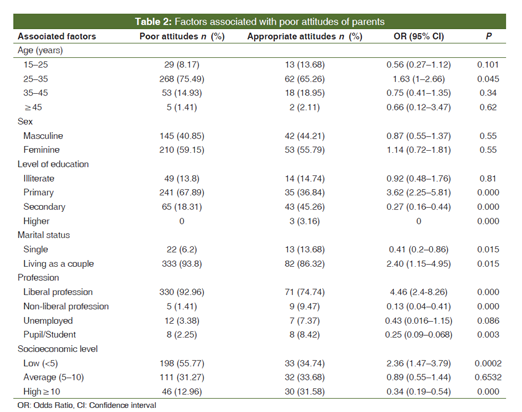
Among the factors analyzed, the 25-35 years age group, primary level of education, the liberal profession, and low socioeconomic level were associated to poor attitudes of parents [Table 2].
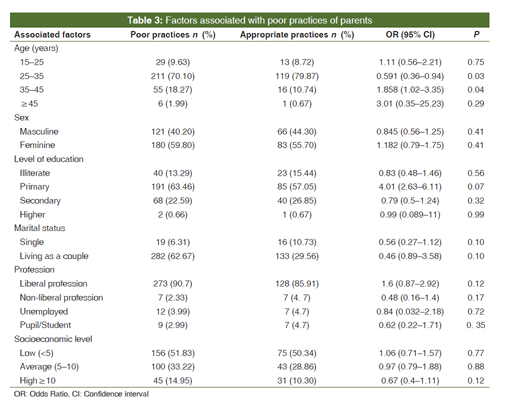
Among the analyzed factors, only the 35-45 years age group was associated with poor practices of parents [Table 3].
Insufficient knowledge of parents on SMC was associated with erroneous attitudes [Table 4].There was no association between the level of knowledge and practices of parents [Table 5]. There was no association between the attitudes and practices of parents [Table 6].



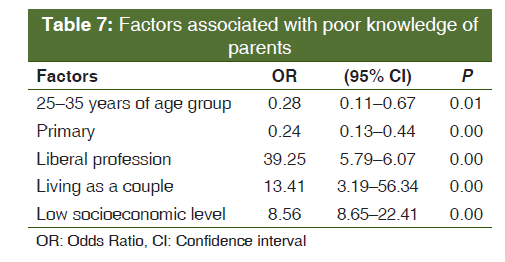
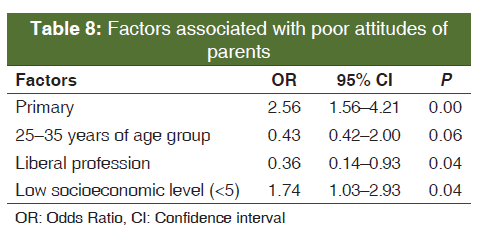
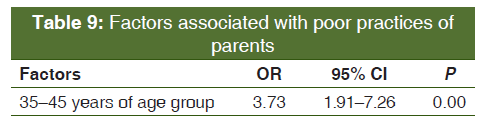
After multivariate analysis with logistic regression, the liberal profession, low socioeconomic level, and living as a couple stood out as factors associated to poor knowledge [Table 7], the primary level of education and low socioeconomic level were factors associated with erroneous attitudes of parents [Table 8]; and the 35-45 years of age group was a factor associated with inappropriate practices of parents [Table 9].
DISCUSSION
In our study, the average age of parents was 31 years with a sex ratio of 0.71. This female predominance in our study is explained by the societal framework of the northern regions where women stay at home to take care of domestic chores and the children's education while the men go out to fend for the needs of the family. 73.33% of parents were aged between 25 and 35 years, and 92.22% were living as a couple at the time of the study[6]. This is due to the fact that early marriages and stigma attached to divorce are common in this community. More than half of them (61.33%) attained a primary level of education. This is explained by the fact that the Cameroon government and its partners made primary education free and obligatory since many years [6,7]. Most of the parents (89.11%) practiced a liberal profession,[6] mainly agriculture, and 51.33% of these parents had a low socioeconomic level [8]. This may be due to the fact that most parents did not further their education after the primary level nor did they undergo any professional training. This obliges them to turn to the informal sector. More than half of the parents (63.11%) had sufficient knowledge on SMC [7]. This result could be ameliorated if both parents were involved in the process. Actually, health agents are more interested in mothers of children for the institution of SMC. More than a third (78.89%) of parents had poor attitudes toward SMC. These erroneous and sometimes hostile attitudes toward SMC were due mainly to three factors. Parents did not understand the principle of prevention and therefore found it absurd that free medication was given to healthy children but was made to pay for the treatment of sick children. The occurrence of AEs in seemingly healthy children made them think that SMC made the children sick. Moreover, a good number of parents due to insufficient knowledge thought that the management of AE was to be paid for. More than half (66.89%) of the parents had appropriate practices toward SMC [7]. These still inadequate results can be explained by the fact that, with SMC being a quite recent measure, most parents do not yet have the reflex to appropriately administer the SMC nor do they have the reflex to run to health facilities in case of the occurrence of AE.
As concern associated factors, the liberal profession, low socioeconomic level, and living as a couple were associated to poor knowledge. Actually, most parents were farmers (liberal profession), a profession which sometimes made them unavailable during the rainy season for the IEC sessions. Living as a couple is a factor associated to poor knowledge. To better understand this, it is a proper highlight that 58.45% of people living as a couple were women, 73.43% were aged between 25 and 35 years, 61.35% of these people attained a primary level of education, and 89.91% practiced a liberal profession. Moreover, parents of both the sexes were included in our study, but some fathers were not included in the IEC on SMC.
Poor attitudes were associated with a primary level of education and a low socioeconomic level. This may be due to the fact that parents not having proper education or having a low income found it absurd to give medication to healthy children and refuse to treat the sick ones freely.
CONCLUSION
At the end of our study, we conclude that the knowledge, attitudes, and practices of parents of children aged 3-59 months toward SMC in the Mokolo health district are, respectively insufficient, erroneous, and inappropriate.
We thus recommend that IEC toward SMC be reinforced, and health facilities in the area should systematically organize counter visits to ensure the effective administration of the drugs by the parents.
ACKNOWLEDGMENT
We express our sincere thanks and appreciations to all the parents who accepted to participate in this study.
References
- Programme National De Lutte Contre Le Paludisme Cameroun. Guide de Mise en OEuvre de la Chimio-Prevention du Paludisme Saisonnier Dans les ReGIONS du Nord et de l'Extreme-Nord. Yaounde; 2016. p. 66.
- Programme National de Lutte Contre le Paludisme Cameroun. Manuel de Formation Pour la Chimio-Prevention du Paludisme Saisonnier Dans Les Regions du Nord et de l'Extreme-Nord: A l' Intention des Formateurs. Yaounde. Juillet; 2016. p. 71.
- Organisation Mondiale de la Sante. Chimio-prevention du Paludisme Saisonnier Par Administration de Sulfadoxine- Pyrimetamine et d'Amodiaquine aux Enfants: Guide De Terrain. Bibliotheque de l'OMS. CH-1211 Geneve 27 - Suisse; 2013. p. 56.
- Actu-Plus. Selon Andre Mama Fouda, la Mortalite due au Paludisme au Cameroun est passe de 30% a 12,4% entre 2012 et 2016. Disponible sur: Available from: https://www.actu-plus-plus.cm/2017/04/selon-andre-mama-foudala-mortalite-due-au-paludisme-au-cameroun-est-passe-de-30-a-12-4-entre-2012-et-2016. [Last accessed on 2017 Nov 11];[Last cited on 2017 Apr 28].
- Guru R, Shilpa S, Maheshwaran R. Revised socio-economic status scale for urban and rural. Int J Sci India 2015;4:167-74.
- Diop S, Kaly J, Lawson D, Diop M, Diop B. Connaissances, attitudes, et pratiques des meres ou gardiennes d'enfants surla chimio prevention du paludisme saisonnier. Med Mal Infect 2017;4:S97.
- Salissou I, Moustapha ML, Yerima B, Alkassoum I, Hadiza D, Ibrahim ML. Perception de la chimio prevention du paludisme saisonnier au Niger. Int J Biol Chem Sci 2016;10:2710-5.
- Institut National de la Statistique. Deuxieme Enquete sur le Suivi des Depenses Publiques et le Niveau de Satisfaction des Beneficiaires Dans les Secteurs de L'education et de la sante au Cameroon; 2010. p. 45.