Anthropometric Measurements in Children 6-59 Months Old in the Minawao Refugee Camp, in the Far North Region of Cameroon
Dorine Faine1, Peter Nde Fon1, Lawrence Mbuagbaw2, Steve Cedric Tegang3, Alfred Bruno Etoubou Yobo3, Andreas Chiabi4
2.Department of Pediatrics, Faculty of Health Sciences, University of Buea, Cameroon,
3.Department of Public Health, Minawao Refugee Camp, Extreme North Region, Cameroon,
4.Department of Pediatrics, Faculty of Medicine and Biomedical Sciences, University of Yaounde I, Cameroon
Citation : Faine D, Fon PN, Mbuagbaw L, Tegang SC, Yobo ABE, Chiabi A. Anthropometric Measurements in Children 6-59 Months Old in the Minawao Refugee Camp, in the Far North Region of Cameroon. Clin Res Pediatr 2018;1(2):1-9.
Child malnutrition, both undernutrition and overnutrition, is global public health problems that affect children worldwide. A major cause of morbidity and mortality among refugee children is undernutrition with food insecurity being a major factor. The aim of this study was to determine the prevalence and risk factors associated with malnutrition among children aged 6-59 months old in Minawao refugee camp, Cameroon.
A cross-sectional study was carried out from March to April 2017 in which the anthropometric indicators (weight, height, length, and midupper arm circumference) of 366 children aged 6-59 months were measured and sociodemographic data recorded.
The overall prevalence of undernutrition among the 366 children sampled was 43.2%, i.e., 158 of the children had at least one of the three indices (weight for height, weight for age, and height for age) <-2 Z-score, while 10 (2.7%) had Z-score of >2 for either weight for age or height for age. The prevalence of underweight, wasting, and stunting was 36.3%, 18.9%, and 22.4%, respectively. Large household size was associated with wasting (P = 0.038). Diseases were associated with underweight (P = 0.005).
The result of these study showed that the prevalence of malnutrition in children 6-59 months old in Minawao refugee camp is high and at a precarious level. This situation should be addressed to halt any further deterioration of the nutritional status of the children in the camp.
Anthropometry, malnutrition, refugees, Z-scores
INTRODUCTION
Malnutrition is simply defined as lack of proper nutrition and can be overnutrition or undernutrition when food needed for growth and development is inappropriate[1]. The World Health Organization (WHO) defines malnutrition as a cellular imbalance between the supply of nutrient and energy and the body's demand for them to ensure growth, maintenance, and specific function[2]. Malnutrition remains one of the main causes of morbidity and mortality in children, especially in under-fives[3]. More than half of childhood deaths worldwide are due to malnutrition[4]. In 2016, the United Nations International Children's Emergency Fund - estimated that globally, 22.9% of children suffer from stunting and 7.7% from wasting[5].
About 21.3 million people in the world are refugees[6]. A critical problem faced by refugees is food shortages because most refugees do not have enough food to feed on as they depend on food provided by humanitarian aid.[7-9] As a result of these food shortages, undernutrition tends to be a common problem among refugees in which children are more affected because they are most vulnerable, thereby increasing the rate of morbidity and mortality among refugee children, especially under 5 years of age.[10-12] Studies done among refugee children in some refugee camps in and out of Africa revealed high prevalence of malnutrition.[13-17] Chiabi et al. noted in a study among Central African refugee children in the east region of Cameroon that revealed a prevalence of 39.32% of global acute malnutrition using the midupper arm circumference (MUAC)[18]. Since 2013, the Boko Haram conflict led to the influx of refugees from the Nigerian and Cameroonian borders into the Cameroonian territory, and the majority of these refugees were hosted in the Minawao refugee camp.[19] Giving the prime importance of nutrition in these settings, especially in children we decided to carry out this study aimed at determining the prevalence of malnutrition and the associated risk factors in children 6-59 months old in this refugee camp in the Far North Region of Cameroon.
METHODS
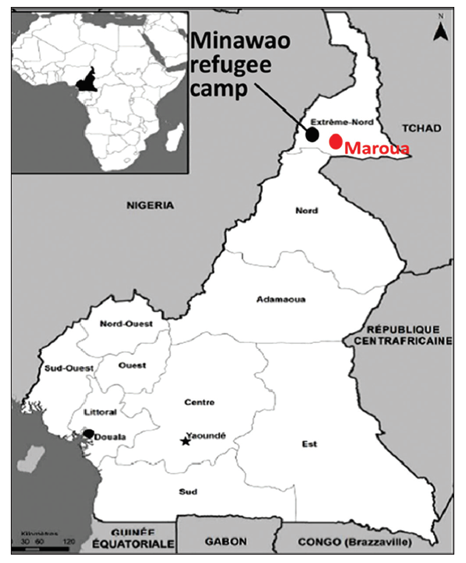
The study was a cross-sectional study in children the Minawao refugee camp in the Far North Region of Cameroon [Figure 1]. This camp is the largest refugee camp in Cameroon located in the Far North Region, hosting victims from the Boko Haram crises. The camp became operational in 2013 with about 7000 refugees, but now, it has a population of 62,565 with an average of four persons per house; (camp records, April 2017)[19]. 97% of the refugees originate from Adamawa state and 2% come from Borno state, respectively, from Nigeria. 1% come from other places[20].
The study included children aged 6-59 months old in the camp whose parents gave consent and who lived in the households that were selected until the sample size was reached between March 20 and April 15, 2017. After obtaining authorization from the administrative authorities of the camp, a systematic sampling method was used to recruit the children for the study until the calculated sample size was reached. The sample size was calculated using Cochran's formula. The geographical arrangement of the houses in the camp enabled us to use a systematic sampling following calculation of the sampling interval which was 39. By random sampling, the first house was chosen. We kept adding the sampling interval to the previous house number until our sample size was obtained. Next, a well-structured questionnaire was used by to collect data by a face-to-face interview from the mothers of the children. Birth dates of child and mother were obtained from the refugee card. Weight was measured using an electronic weighing scale. The child was either naked or with minimum/lightly/clothing and no shoes. Calibration before weighing every child was done to ensure it was at zero. For children more than 2 years, they stood erect on an electronic balance with their heads straight facing forward. The result was read to the nearest 0.1 kg. In case of children aged < 2 years, the mother was first weighed alone and then mother and child weighed together. Weight of mother was subtracted from weight of mother and child to get child's weight. Body length of children age up to 24 months was measured without shoes. The length was read to the nearest 0.1 cm. The children were measured lying down horizontally on the L- shaped height board graded in centimeters with their faces looking upward and with the help of an assistant. The height of children >24 months was measured with the children standing erect with their feet flat on the height board without shoes. Then, height was read to the nearest 0.1 cm. To determine the presence of edema, normal thumb pressure was applied to an area for few seconds then released and checked for pitting; however, we had no case of edema in this study. MUAC was measured on the left arm, in the midpoint between the elbow and the shoulder. It was measured using the three-colored tape.
Data collected involved sociodemographic, clinical, and anthropometric characteristics. Data collected were properly checked before entry into Epi data 3.1 and were exported and analyzed using SPSS version 21.0, Epi info 3.5.1, and the WHO anthropometry.
All variables were categorized and described using frequency distributions. Bivariate associations were described using Chi-square test. A variable was statistically significant when P = 0.05.
Ethical approval for the study was sought from the Institutional Review Board of the Faculty of Health Sciences, Buea. An informed consent was sought from parents, and assent was sought from children who could understand.
RESULTS
Data were obtained from the 366 children enrolled.
Among the 366 children enrolled in our study, the global incidence of malnutrition was 43.2%, 69 (18.9%) had a weight-for-height Z-score (WHZ) of < -2, 82 (22.4%) had a height-for-age Z-score (HAZ) of < -2, 133(36.4%) had weight-for-age Z-score (WAZ) of < -2, and 10 (2.7%) had Z scores of >2.
In this study, we worked among refugee children 6-59 months old. The refugees came from Nigeria and the borders of Cameroon. 97.14%, 1.82%, and 0.09% came from Borno, Adamawa, and Jigawa states, respectively (Nigeria), and 0.97% from other places[21].
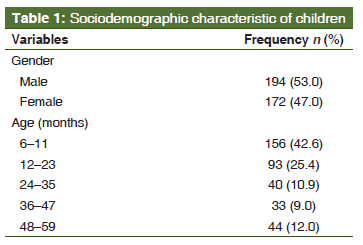
There were a total of about 38,034 children aged 0-17 years old in the camp (from the camp records). 366 children aged 6-59 months were enrolled as the scope of our study. Of the 366 children, 194 (53.0%) were male and 172 (47.0%) females giving a sex ratio of 1.1. The mean age was 19.8 months. Most of children (42.6%) were in the age group of 6-11 months [Table 1].
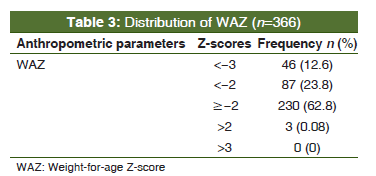
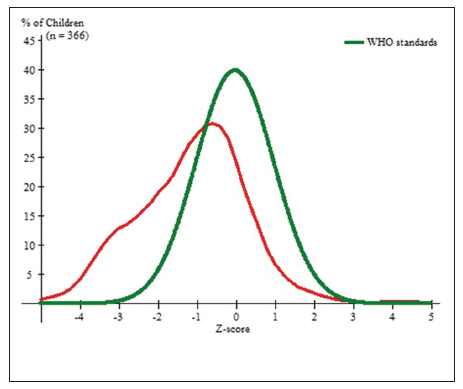
133 (36.4%) had a WAZ < -2 indicating underweight with 46 (12.6%) having WAZ < -3 while 3 (0.08) had WAZ >2 indicating overweight [Table 3].
The curve of our study has moved to the left which is a negative skewing (negatively skewed) with respect to the WHO curve [Figure 2].
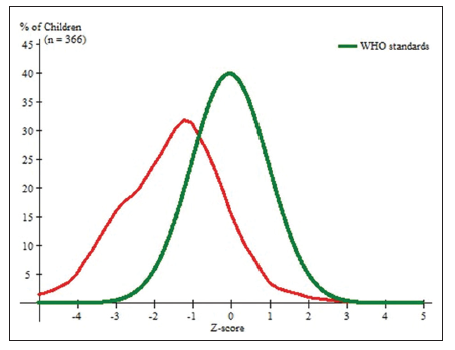
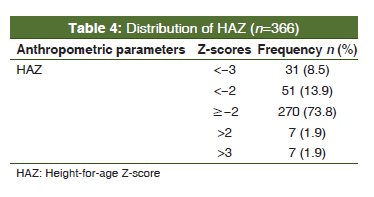
82 (22.4%) had HAZ < -2 while 14 (3.8%) had HAZ >2 [Table 4]. The curve of our study has moved to the left which is a negative skewing (negatively skewed) with respect to the WHO curve [Figure 3].
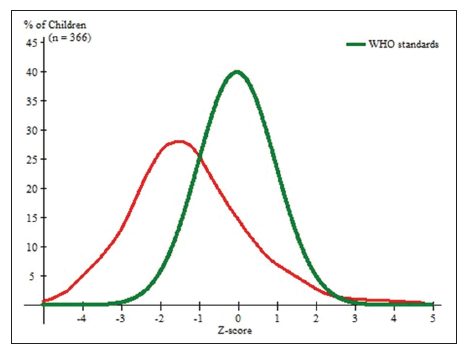
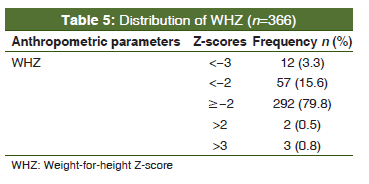
69 (18.9%) had WHZ < -2. 5 (1.3%) had WHZ >2 [Table 5].
The curve of our study has moved to the left which is a negative skewing (negatively skewed) with respect to the WHO curve [Figure 4].
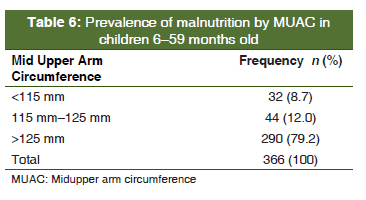
76 (20.7%) had MUAC < 125 mm and 8.7% severely wasted [Table 6].
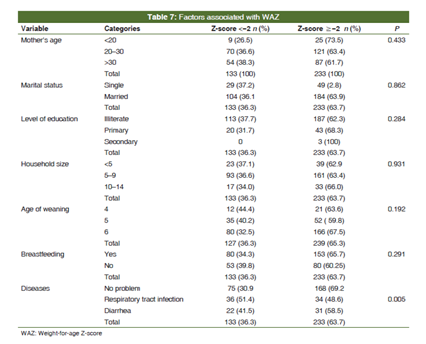
There was an association between diarrhea, respiratory tract infection, and underweight on bivariate analysis [Table 7], but no statistically significant association on multivariate analysis with logistic regression.
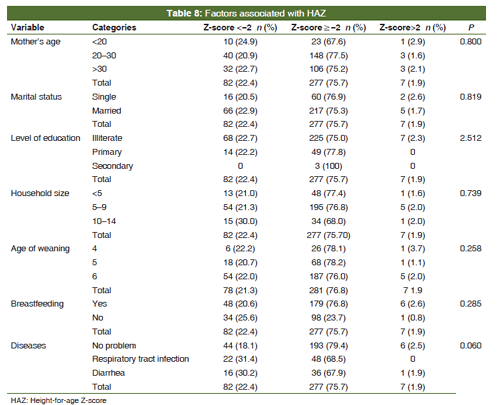
There was no statistical significance between any of the variables and stunting [Table 8].
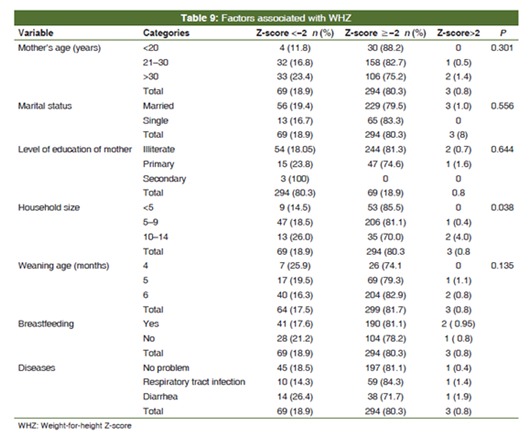
There was a statistical significance between household size and wasting on bivariate analysis [Table 9], but this significance disappeared on multivariate analysis with logistic regression.
DISCUSSION
The study population consisted of 194 (53.0%) males and 172 (47.0%) females with a sex ratio of 1.1. Our population was similar to that of Kelati et al. and Faraj[22]. This result contrasted that of Nwagboso who had more females 316 (55.06%) than males 258 (44.94%) in his study of refugee children in Namibia[23]. The mean age of our study population was 19.81 months, with an age range of 6-59 months. It was noted that most of the children 156 (42.6%) were in the 6-11 months age group. Our study population was similar to that of Faraj and Nwagboso whose age group was 6-59 months, but the mean age in the children was higher.[22,23] Our mean age was also lower than that of Hossain et al. who had 29 months as mean age[15].
We observed that 36.4% of the children were underweight (12.6% severe and 23.8% moderate). Underweight reflects both past (chronic) and present (acute) malnutrition but does not distinguish between the two. It could result from a brief period of food deprivation or disease[24]. Our figure is higher than that of Kelati et al. and Banjong et al., who had prevalence of 33.4% and 33.7%, respectively,[13,25] but lower than that of Nwagboso in a refugee camp in Namibia who noted a prevalence of 45%[23] The negative skewness of the curve of our study population compared to the WHO growth distribution curve indicates that most of the children had a Z-scores < -2. Our median was lower than that of the WHO standards indicating a high prevalence of underweight in our study population.
We observed an incidence of 22.4% of stunting which indicates chronic malnutrition (8.5% severe and 13.9% moderate). Stunting usually results from long-term undernutrition during the periods of growth and development in early life. It can also be due to infectious diseases that last over a long period of time. It is an indicator of the quality of the environment and the socioeconomic status of a population[24]. Our result was lower than those noted by Grijalva-Eternod et al. in Algeria[16] and Nwagboso in Namibia[23]and Oweldo et al. in Uganda[14] who had 29.1%, 41%, and 52.4%, respectively. Our finding showed that chronic malnutrition was average when referenced with the WHO values for severity of malnutrition. We had a negatively skewed height-for-age curve with respect to the WHO curve. This denoted that most of the children had a < -2 Z-score indicating high a level of stunting in our study population.
We had an incidence of 18.9% for wasting which is acute malnutrition (3.3% severe and 15.6% moderate). Wasting is a measure of body mass in relation to height, and it shows the present nutritional status of an individual. It could be greatly influenced by the season during which the study was done[25].
This finding is higher than that observed by Teng and Shariff[17] in Malaysia, Banjong et al. in[25] Thailand, and Nwagbos[23]o in Namibia who noted 16.1%, 8.7%, and 8.17%, respectively, but lower than the 22.6% noted by Kelati et al.[13] in Northern Ethiopia.
Acute malnutrition in this study could have resulted from a recent food scarcity over a recent period before the study or loss in weight due to acute illnesses. The negative skewness of the curve of our study population compared to the WHO curve indicates that the degree of wasting in the children was high.
We had an incidence of 20.7% acute malnutrition from the MUAC measurements, with 8.7% severe and 12.0% moderate. MUAC is a predicting indicator of risk of imminent death.[24] Our figure was lower than that of Chiabi et al. in Gado-Bazere refugee camp, who noted 39.32%[18]. Polonsky et al. also had a higher incidence of 43.4% in children in the Dadaab refugee camp in Kenya[26].
The incidence of underweight was higher in children who had respiratory tract infections and diarrhea but statistically none significant on multivariate analysis. Teng et al., Jemal et al., and Faraj presented that there was association between having a disease and malnutrition[17,22,27] Poor sanitation conditions and overcrowding could be responsible for having a disease, which will impact on the nutritional status of the children.
We did not note any statistically significant factor associated with stunting in this study. Olwedo et al. in their study carried out in Uganda had an association between being a male child and being stunted[14].
The incidence of wasting was higher in households with 10-14 people, than in those with < 5. Household size was not significantly associated with wasting on multivariate analysis. Teng et al. and Nwagboso[23]noted a better nutritional status among refugee children who lived in households with less than five persons. This could be due to the fact that as the family size increases the food ration decreases. Decrease in food rations and inadequate intake could be the main factors contributing to malnutrition in the camp. Other studies in refugee camps noted similar findings[13,22,23,28] From the camp's records, the quantity of kilocalories provided per person was initially 2500 kcal but has dropped to 1300 kcal because of the rapidly increasing population in the camp, thus the food supplied to them is no longer enough to produce the energy required per head. The food ration comprises rice, flour, oil, groundnuts, and beans. The quantity of kilocalories of food provided is below the total minimum ration energy requirement established by the world food program (WFP) and the WHO which is a minimum of 2100 kcal per person per day[13].
This situation is worsened by the fact that some refugees sell some of the food rations out of the camp to meet up with their financial needs.
The main limitations of this study are the fact that we did not do a dietary diversity score, because all the refugees in the camp were receiving the same foodstuffs as supplied by United Nations High Commission for Refugees (UNHCR) and the WFP; and also children < 6 months were not included in the study. From this study, we thus recommend that the refugees in this camp be sensitized on good nutrition and health nutritional practices to alleviate the burden of malnutrition. The national and international authorities of the camp should step up efforts to ensure adequate food provision in the camp for the refugees and especially for children who are most vulnerable.
ACKNOWLEDGMENTS
We are grateful to UNHCR representative in Cameroon and all field workers in the Minawao refugee camp for their support and Mr. Nana Celestine for assisting in the data analysis.
References
- Oothuizen D, Oldewage-Theron W, Napier C. A Nutrition Education Programme for Primary School Children: Short-and Long-Term Changes in Nutrition Knowledge. Vaal University of Technology. Available from: https://www.scribd.com/ document/175307231/02. [Las accessed on 2017 Jan 12].
- Harohalli RS. Malnutrition: Practice Essentials, Background, Pathophysiology. Available from: http://www.emedicine. medscape.com/article/985140. [Las accessed on 2017 Jan 12].
- Mengistu K, Alemu K, Destaw B. Prevalence of malnutrition and associated factors among children aged 6-59 months at Hidabu Abote District, North Shewa, Oromia Regional state. J Nutr Disorders Ther 2013;T1:1.
- Bain LE, Awah PK, Geraldine N, Kindong NP, Sigal Y, Bernard N, et al. Malnutrition in Sub-Saharan Africa: Burden, causes and prospects. Pan Afr Med J 2013;15:120.
- UNICEF. Undernutrition Contributes to Nearly Half of All Deaths in Children Under 5 and is Widespread in Asia and Africa. Available from: https://www.data.unicef.org/topic/ nutrition/malnutrition. [Las accessed on 2017 Jan 12].
- UNHCR. Figures at a Glance. Available from: http:// www.unhcr.org/figures-at-a-glance.html. [Las accessed on 2017 Jan 12].
- UNHCR. As food shortages hit 800,000 African refugees, UNHCR and WFP issue urgent appeal. Available from: http://www.unhcr.org/news/latest/2014/7/53b2a1969/food-shortages-hit-800000-african-refugees-unhcr-wfp-issue-urgent-appeal.html. [Las accessed on 2017 Feb 8].
- Food, Water, Sanitation, and Housing in Refugee Camp. Available from: http://www.unite forsight.org/refugee-health/ module3. [Las accessed on 2017 Feb 24].
- WHO. Child Health in Complex Emergencies. WHO. Available from: http://www.who.int/bulletin/volumes/84/1/019570/en/.[Las accessed on 2017 Mar 2].
- Toole MJ, Waldman RJ. An analysis of mortality trends among refugee populations in Somalia, Sudan, and Thailand. Bull World Health Organ 1988;66:237-47.
- UNHCR. Refugee Health. Available from: http://www. unhcr.org/excom/scaf/3ae68bf424/refugee-health.html. [Last accessed on 2017Feb 9].
- Khan MU, Munshi MH. Clinical illnesses and causes of death in a Burmese refugee camp in Bangladesh. Int J Epidemiol 1983;12:460-4.
- Kelati H, Mengiste B, Alemayehu T, Damtew B. Prevalence of acute malnutrition and its associated factors among children aged 6-59 months in Mai-Aini Eritrean Refugees Camp, Northern Ethiopia. J Nutr Food Sci 2014;5:336.
- Olwedo MA, Mworozi E, Bachou H, Orach CG. Factors associated with malnutrition among children in internally displaced person's camps, Northern Uganda. Afr Health Sci 2008;8:244-52.
- Hossain SM, Leidman E, Kingori J, Al Harun A, Bilukha OO. Nutritional situation among Syrian refugees hosted in Iraq, Jordan, and Lebanon: Cross sectional surveys. Confl Health 2016;10:26.
- Grijalva-Eternod CS, Wells JC, Cortina-Borja M, Salse-Ubach N, Tondeur MC, Dolan C, et al. The double burden of obesity and malnutrition in a protracted emergency setting: A cross-sectional study of Western Sahara refugees. PLoS Med 2012;9:e1001320.
- Teng TS, Shariff ZM. Nutritional status of Rohingya children in Kuala Lumpur. Malays J Med Health Sci 2011;7:41-9.
- Chiabi A, Ehouzou MC, Kamo S., Tetanye N, Assim M. Health campaign for children in catastrophic situations :The case of the Central African refugee camp in Gado-Badzere in East Cameroon. Med Afr Noire 2016;63:192-200.
- UNICEF. Life in Minawao Refugee Camp. Moments of Joy Amid an Uncertain Future; 2015. Available from: https:// www.medium.com/photography-and-social-change/life-in-minawao-f8bd72bf677e. [Last accessed on 2017 May 12].
- UNHCR. Minawao: Profil du camp au 13 Mai; 2016. Available from: http://www.reliefweb.int/sites/reliefweb.int/ files/resources/Profil_Camp_Minawao_13052016.pdf. [Last accessed on 2017 May 12].
- UNHCR: Minawao. Profil du camp. Fevrier; 2017. Available from: http://www.relief web.int/sites/relief\web.int/files/ resources/Profile_Camp_Minawao_Fevrier_2017.pdf. [Last accessed on 2017 May 25].
- Faraj N. Nutritional status of Under Five Year Old Burmese Refugee Children in Thailand. [Hawaii]: University of Hawaii; 2005. Available from: http://www.scholarspace.manoa.hawaii.edu/bitstream/10125/10528/1/uhm_ms_3953_r.pdf. [Last accessed on 2018 May 5].
- Nwagboso GC. An Evaluation of the Nutritional Status of Refugee Children in Namibia. [Namibia]: University of the Western Cape; 2014. Available from: http://www.etd.uwc.ac.za/ xmlui/handle/11394/1644. [Last accessed on 2018 May 5].
- Chiabi A, Nem D, Kobela M, Mbuagbaw L, Obama MT, Ekoe T. Anthropometric measurements of preschool children in North Cameroon. East J Med 2011;2011:240-7.
- Banjong O, Menefee A, Sranacharoenpong K, Chittchang U, Eg-kantrong P, Boonpraderm A, et al. Dietary assessment of refugees living in camps: A case study of Mae la camp, Thailand. Food Nutr Bull 2003;24:360-7.
- Polonsky JA, Ronsse A, Ciglenecki I, Rull M, Porten K. High levels of mortality, malnutrition, and measles, among recently-displaced Somali refugees in Dagahaley camp, Dadaab refugee camp complex, Kenya, 2011. Confl Health 2013;7:1.
- Jemal Y, Haidar J. Chronic malnutrition and its determinants among refugee children: Evidence from refugee camp of Ethiopia. East Afr J Public Health 2014;11:816-22.
- World Food Programme (WFP). Centers for Disease Control and Prevention (CDC). A Manual: Measuring and Interpreting Malnutrition and Mortality; 2005.