Serum 30-day Dose-response Test (+S30DR) to Evaluate Vitamin A Deficiency among Brazilian Male Adolescents
Ivan Savioli Ferraz1, Cristiane Simoes Bento de Souza1, Carlos Eduardo Martinelli Jr1, Luiz Antonio Del Ciampo1, Alceu Afonso Jordao Jr2, Helio Vannucchi2, Ieda Regina Lopes Del Ciampo1, Carlos Alberto Nogueira-de-Almeida3
2.Department of Internal Medicine, Ribeirao Preto Medical School, University of Sao Paulo, Ribeirao Preto-SP, Brazil.
3.Department of Medical, Federal University of Sao Carlos - UFSCAR, Sao Paulo, Brazil.
Citation : Ferraz IS, de Souza CSB, Martinelli CE Del, Ciampo LA, Jordao AA, Vannucchi H, Del Ciampo IRL, Nogueira-de-Almeida CA. Serum 30-day Dose-response Test (+S30DR) to Evaluate Vitamin A Deficiency among Brazilian Male Adolescents. Clin Res Pediatr 2018;1(2):1-5.
Vitamin A deficiency (VAD) is prevalent in low-income countries and it has been little studied in adolescents. The aim of the study was to identify VAD among Brazilian male adolescents.
A total of 80 healthy male adolescents were analyzed by the serum 30-day dose-response (+S30DR) test, which consists of the determination of serum retinol concentration (SRC) before and after supplementation with 200,000 IU retinyl palmitate.
About 43.7% (35/80; 95% CI: 30.3-59.9%) of the adolescents presented VAD. The mean SRC before and after supplementation was 1.30 µmol/l (SD: 0.41) and 1.54 µmol/l (SD: 0.41), respectively (P = 0.01). There was no association between increased serum C-reactive protein concentrations and VAD. No adolescent had xerophthalmia.
A high prevalence of low reserves of Vitamin A was observed. A dose of 200,000 IU retinyl palmitate caused a favorable change in Vitamin A status. The +S30DR proved to be a useful tool for the detection of VAD subclinical in adolescents
Adolescent, Vitamin A, Vitamin A deficiency
INTRODUCTION
Vitamin A deficiency (VAD) is one of the most common and widespread nutritional deficiencies in the world and constitutes a significant public health problem [1-4]. In addition, it is one of the more common causes of potentially avoidable blindness and is responsible for the increases in morbidity-mortality due to diarrhea and respiratory causes, particularly in developing countries [1-10]. In Brazil, studies have shown a high prevalence of VAD in various regions of the country [11,12].
The use of serum retinol concentration (SRC) measurements by high-performance liquid chromatography (HPLC) is recommended as a method to assess Vitamin A status of populations [13-15]. SRC ≥ 1.05 µmol/l is proposed to be adequate for populations considered to be well nourished;[13-17] however, this indicator is not a reflection of the Vitamin A liver stores and it can be normal even though liver reserves are low. Due to its strict homeostatic control, SRC is associated with Vitamin A status in the organism only in the extreme situations of deficiency and toxicity [10,14,18,19]. Furthermore, it may be influenced by some factors such as infection, inflammation, and recent dietary intake [10,13,14]. The change of SRC to a standard oral dose of Vitamin A takes in account that when Vitamin A liver reserves become low,retinol-binding protein (RBP) accumulates in the liver before SRC decreases. Thus, when a standard dose of Vitamin A is administered, retinol binds to RBP accumulated and releases into the serum [13-21]. Relative dose response (RDR), the precursor of these tests, requires two blood samples from the same individual within a 5-h interval. The serum 30-day dose response (+S30DR) works on the same principle as the RDR test but requires the second sample within a 30-45-day interval. It has the advantage of being diagnostic and therapeutic since the oral administration of 200,000 IU retinyl palmitate is required for its application, and this dose may be sufficient for the treatment of subclinical VAD [16].
Preliminary studies on the community where this study was conducted showed an elevated prevalence of VAD among healthy children,[21-23] but few data are available on Vitamin A status in adolescents. Thus, this study aimed to determine the prevalence of VAD in adolescents at a general pediatric outpatient clinic using the +S30DR.
SUBJECTS AND METHODS
This was a descriptive cross-sectional study of prevalence conducted from September 2009 to August 2010. Regarding the potential risk of teratogenic effects in the fetus,[14,24-26] the study was conducted only among males. All adolescents aged ≥10-< 19 years followed up at a Primary Health Care Unit of Ribeirao Preto, Brazil, were invited to participate in the study and 100 agreed, but the ones with chronic diseases or diarrhea that might compromise their nutritional status and intestinal absorption, as well the adolescents that did not attended the second blood collection and were excluded from the final analysis, resulting in 80 participants.
The blood sample obtained after 6 h of fasting was used for the determination of serum retinol (pre-supplementation) and of C-reactive protein (CRP) and, then, an oral dose of 200,000 IU retinyl palmitate was administered. A small greasy meal with a low retinol concentration was offered after supplementation to facilitate retinol absorption. After the first collection, the adolescents were instructed to come to the unit within 30-45 days after 6 h of fasting for the collection of the second blood sample for the determination of SRC after supplementation.
Serum retinol was measured by high HPLC[27] with a model LC9 Shimadzu® (Japan) apparatus with a 25 cm X 0.46 cm C18 column (ODS), UV/Vis detector (SPD-6AV), SCL-6B controller, and C-R6A register calibrated for retinol measurement at 325 nm wavelength. The flow of the mobile phase was fixed at 2 ml/min. All- trans-retinol (Sigma® Chemical Co., St Louis, MO, USA) was used as an external standard. The detection limit of the method was 0.016 µmol/l. The +S30DR was calculated by the following formula (1): +S30DR = ([T1-T0]/T1) X100. Values ≥ 20% are indicative of low hepatic reserves of Vitamin A [16].
Serum CRP concentrations were determined by turbidimetry to assess the possible interference of inflammatory processes with SRC and values =0.5 mg/dL were considered abnormal [28-30].
An interview to obtain information about the family income, an ocular inspection was performed by a trained pediatrician for signs of xerophthalmia and anthropometric data were collected at the first visit. Z scores of body mass index were calculated to classify the nutritional status according to the criteria of the World Health Organization [31,32].
The difference in mean retinol values before and after supplementation was analyzed by the Student's t-test and Poisson models were adjusted to estimate the prevalence ratios of individuals with SRC ≤1.05 µmol/l before and after supplementation. A logistic regression model was used to analyze the influence of serum CRP on Vitamin A status. A second OR and 95% CI value were calculated with adjustment for CRP values. A linear regression model was adjustedto study theinfluenceof serum CRPconcentrationson pre-supplementation SRC. To determine the best sensitivity/ specificity ratio for the +S30DR of the study population and using the pre-supplementation SRC, a receiver operating characteristic (ROC) curve was constructed. The level of significance was set at 5%. The SAS software version 9.2 (SAS Institute Inc., 2008) was used.
The study was approved by the Research Ethics Committee of the University Hospital, Ribeirao Preto Medical School, University of Sao Paulo.
RESULTS
A total of 80 male adolescents participated in the study. 65.0% (52/80) were from families with monthly income up to US$ 285.00, with access to health and vaccination services, electricity, piped water, sewage system, and brick houses. 52 (65%) were classified as eutrophic, 14 (77.5%) as overweight, 10 (12.5%) as obese, and 4 (5%) as thin. 43.7% (35/80; 95% CI: 30.3-59.9%) had +S30DR tests indicative of low hepatic Vitamin A reserves. No adolescent had xerophthalmia and 2.5% (2/80) had pre-supplementation SRC ≤0.70 µmol/l. Regarding the post-supplementation SRC, only 1 (1.2%) adolescent had a value ≤0.70 µmol/l. In addition, 30.0% (24/80; 95% CI: 18.9-43.4%) of the adolescents had pre-supplementation SRC ≤1.05 µmol/l. Although 10.0% (8/80) of the adolescents still had SRC ≤1.05 µmol/l after supplementation, a significant reduction of this proportion was observed (prevalence ratio =3.0; 95% CI 1.54-5.82; P < 0.01).
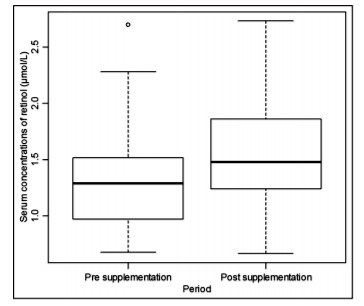
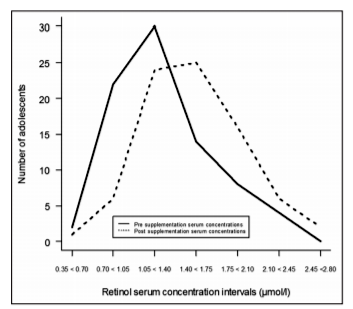
The mean pre- and post-supplementation SRC were 1.30 µmol/l (SD: 0.41) and 1.54 µmol/l (SD: 0.41; P < 0.01), respectively, and the median values were 1.29 µmol/l and 1.48 µmol/l, respectively [Figure 1]. Since only two adolescents had pre-supplementation SRC ≤0.70 µmol/l, the ≤1.05 µmol/l value was used as reference for the definition of inadequate Vitamin A concentrations for the construction of the ROC curve. The cutoff point of 20% for +S30DR showed 79% sensitivity and 69% specificity, being the most adequate for the study population. A "rightward shift" was observed for the curve of frequency distribution of SRC after supplementation [Figure 2].
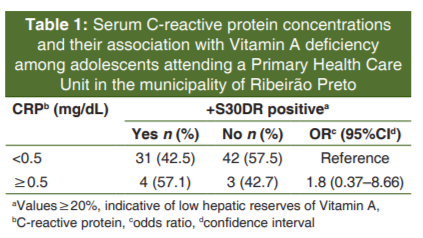
Serum CRP concentrations were high in 8.7% (7/80) of the adolescents, 4 of whom (11.4%-4/35) had low hepatic Vitamin A reserves by +S30DR test and 3 (6.7%-3/45) had not. However, elevated CRP concentrations did not prove to be a risk factor for low hepatic Vitamin A reserves by +S30DR test [Table 1]. In addition, there was no association between CRP values and pre-supplementation SRC (P = 0.21); thus, serum CRP concentrations did not interfere with the final value of the +S30DR.
It was observed that some adolescents with elevated pre- supplementation SRC (>0.70 µmol/l) still presented +S30DR results indicative of low reserves of Vitamin A.
DISCUSSION
Using the +S30DR test, it was observed a high prevalence (43.7%) of low hepatic reserves of Vitamin A. There was 2.5% (2/80) of the adolescents classified as having VAD (pre-supplementation SRC ≤0.70 µmol/l)[16,33] and 30.0% (24/80) with adequate levels (pre-supplementation SRC ≤1.05 µmol/l) [13-17]. A study conducted in a poor community of Rio de Janeiro (Brazil) revealed a 12.6% prevalence of SRC ≤1.05 µmol/l among adolescents of both sexes aged 10-17 years [12]. In another Brazilian study, Graebner et al [11]. observed a 31.6% prevalence of SRC ≤0.70 µmol/l among adolescents living in the rural area of Brazil. In Indonesia, a study detected an initial 41.4% prevalence of SRC ≤1.05 µmol/l among boys and a 45.1% among girls, with the proportions of serum retinol ≤0.70 µmol/l being 11.4% among boys and 7.7% among girls[34]. A study from Bangladesh on 381 adolescents from a privileged socioeconomic class detected 22% with SRC ≤1.05 µmol/l and 1.5% with concentrations ≤0.70 µmol/l [35]. Therefore, the higher prevalence detected by the +S30DR test in the present study suggests that tissue reserves of these adolescents were no longer adequate but not sufficiently depleted to influence the SRC, as also observed in a previous study on preschoolers from the same community [21]. However, the proportion of individuals with serum concentrations ≤1.05 µmol/l (30%) observed is close to those detected in the cited studies.
Despite the high sensitivity of the +S30DR, several factors support the observation that there could be a high prevalence of VAD among the adolescents studied before supplementation with retinyl palmitate. A significant reduction of the proportion of adolescents with SRC ≤1.05 µmol/l was observed 30-45 days after supplementation, even though only 2.5% (2/80) of the adolescents had initial SRC ≤0.70 µmol/l.
Regarding the ROC curve, the cutoff point of 20% for +S30DR showed 79% sensitivity and 69% specificity, being the most adequate for the study population. In a study from the same community studied here, Ferraz et al [21]. suggested a cutoff point of 45% for the +S30DR at preschoolers. In both the study by Ferraz et al [21] and in the present study, the prevalence of low liver reserves detected with the +S30DR was closer to the proportions of serum concentrations ≤1.05 µmol/l than to those presented by the cutoff point of 0.70 µmol/l. In view of the above considerations, these observations support the argument of some authors who propose a value of >1.05 µmol/l as being the most appropriate for SRC considered to be adequate [3,13,36,37].
The mean SRC after supplementation was significantly higher than the pre-supplementation concentration (1.54 µmol/l and 1.30 µmol/l, respectively). A similar phenomenon was detected in Indonesia in a study in which male adolescents were found to have a significant increase in their initial SRC after weekly oral supplementation with 10,000 IU Vitamin A for 3 months [34]. In the present study, we also observed a "rightward shift" of the frequency distribution curve of the SRC after supplementation [Figure 2]. The same was also observed in preschoolers from the same community who had received an oral dose of retinyl palmitate equivalent to the one administered here [21].
Differently of some author's observations,[10,38-40] in the present study, there was no correlation between serum CRP and pre- supplementation SRC and high CRP values did not prove to be a risk factor for VAD. Similar findings were observed in two other studies conducted in the same community [22,23].
Individuals were studied into a convenience sample and might not have represented the community of adolescents in the municipality of Ribeirao Preto. In addition, the relatively small number of individuals investigated may have limited the power of the study. Finally, performing the RDR, whose laboratorial logistic proceedings are difficult due to the age group, could have given more accurate information. However, by observing adolescents with pre-supplementation SRC ≤1.05 µmol/l very close to VAD prevalence detected by the +S30DR, we inferred that the latter may be helpful for adolescents. Moreover, the +S30DR can be therapeutic and can minimize the interpretation errors caused by isolated analysis of serum retinol, which can be influenced by various physiological and pathological situations.
CONCLUSION
A high prevalence of low reserves of Vitamin A was observed in a population of healthy adolescents. In addition, a dose of 200,000 IU retinyl palmitate caused a favorable change in Vitamin A status. The +S30DR proved to be a useful tool for the detection of VAD subclinical in male adolescents.
ACKNOWLEDGMENTS
We thank Coordenacao de Aperfeicoamento de Pessoal de Nivel Superior (CAPES) and Fundacao de Apoio ao Ensino, Pesquisa e Assistencia do Hospital das Clinicas, Faculdade de Medicina de Ribeirao Preto, Universidade de Sao Paulo (FAEPA) for financial support, Davi Aragon for statistical support, the nursing team of Centro Medico Social Comunitario Vila Lobato, and Marina Mendonca Dias and Paula Ovidio (Laboratory of Nutrology, Ribeirao Preto Medical School -USP).
REFERENCES
- Ramakrishnan U, Darnton-Hill I. Assessment and control of Vitamin Adeficiency disorders. J Nutr 2002;132:2947S-2953S.
- WHO. Global Prevalence of Vitamin A Deficiency in Populations at Risk, 1995-2005: WHO Global Database on Vitamin A Deficiency. Geneva (Switzerland): WHO; 2009.
- Chehab ET, Anya BM, Onyango AW, Tevi-Benissan MC, Okeibunor J, Mkanda P, et al. Experience of integrating Vitamin A supplementation into polio campaigns in the African region. Vaccine 2016;34:5199-202.
- Adelekan DA, Northrop-Clewes CA, Owa JA, Oyedeji AO, Owoeye AA, Thurnham DI, et al. Use of biomarkers of sub- clinical infection, nutrition and neonatal maturity to interpret plasma retinol in Nigerian neonates. Br J Nutr 2003;90:353-61.
- Arlappa N, Laxmaiah A, Balakrishna N, Harikumar R, Kodavanti MR, Gal Reddy CH, et al. Micronutrient deficiency disorders among the rural children of West Bengal, India. Ann Hum Biol 2011;38:281-9.
- Bekele A, Asres G, Wondimkun Y, Assefa Y, Reissig D. Conjunctival impression cytology and detection of Vitamin A deficiency in pregnant women, Gondar, Northwest Ethiopia. Ethiop Med J 2012;50:23-30.
- Kheir AE, Dirar TO, Elhassan HO, Elshikh MA, Ahmed MB, Abbass MA, et al. Xerophthalmia in a traditional quran boarding school in Sudan. Middle East Afr J Ophthalmol 2012;19:190-3.
- Sachdeva S, Alam S, Beig FK, Khan Z, Khalique N. Determinants of Vitamin A deficiency amongst children in Aligarh District, Uttar Pradesh. Indian Pediatr 2011;48:861-6.
- Demissie T, Ali A, Mekonen Y, Haider J, Umeta M. Magnitude and distribution of Vitamin A deficiency in Ethiopia. Food Nutr Bull 2010;31:234-41.
- Hotz C, Chileshe J, Siamusantu W, Palaniappan U, Kafwembe E. Vitamin A intake and infection are associated with plasma retinol among pre-school children in rural Zambia. Public Health Nutr 2012;15:1688-96.
- Graebner IT, Saito CH, de Souza EM. Biochemical assessment of Vitamin A in school children from a rural community. J Pediatr (Rio J) 2007;83:247-52.
- de Souza Valente da Silva L, Valeria da Veiga G, Ramalho RA. Association of serum concentrations of retinol and carotenoids with overweight in children and adolescents. Nutrition 2007;23:392-7.
- WHO. Indicators for Assessing Vitamin A Deficiency and their Application in Monitoring and Evaluating Intervention Programmes: Report of a Joint. WHO/UNICEF. [Micronutrient series]. Geneva (Switzerland): WHO; 1996.
- Tanumihardjo SA, Russell RM, Stephensen CB, Gannon BM, Craft NE, Haskell MJ, et al. Biomarkers of nutrition for development (BOND)-Vitamin A review. J Nutr 2016;146:1816S-48S.
- Tanumihardjo SA. Biomakers of Vitamin A status: What do they mean? In: World Health Organization. Report: Priorities in the Assessment of Vitamin A and Iron Status in Populations, Panama City, Panama,15-17 September2010. Geneva: World Health Organization; 2012.
- Flores H, Campos F, Araujo RC, Underwood BA. Assessment of marginal Vitamin A deficiency in Brazilian children using the relative dose response procedure. Am J Clin Nutr 1984;40:1281-9.
- Weinman AR, Jorge SM, Martins AR, de Assis MD, Martinez FE, Camelo JS Jr., et al. Assessment of Vitamin A nutritional status in newborn preterm infants. Nutrition 2007;23:454-60.
- Ferraz IS, Daneluzzi JC, Vannucchi H. Vitamin A deficiency in children aged 6-24 months in Sao Paulo state, Brazil. Nutr Res 2000;20:757-68.
- Ferraz IS, Daneluzzi JC, Vannucchi H, Jordao AA, Ricco RG, Del Ciampo LA, et al. Prevalence of iron deficiency and its association with Vitamin A deficiency in preschool children. J Pediatr (Rio J) 2005;81:169-74.
- Verhoef H, West CE. Validity of the relative-dose-response test and the modified-relative-dose-response test as indicators of Vitamin A stores in liver. Am J Clin Nutr 2005;81:835-9.
- Ferraz IS, Daneluzzi JC, Vannucchi H, Jordao AA Jr., Ricco RG, Del Ciampo LA, et al. Detection of Vitamin A deficiency in Brazilian preschool children using the serum 30-day dose-response test. Eur J Clin Nutr 2004;58:1372-7.
- Custodio VI, Daneluzzi JC, Custodio RJ, Del Ciampo LA, Ferraz IS, Martinelli CE Jr., et al. Vitamin A deficiency among Brazilian school-aged children in a healthy child service. Eur J Clin Nutr 2009;63:485-90.
- Martins TM, Ferraz IS, Daneluzzi JC, Martinelli CE Jr., Del Ciampo LA, Ricco RG, et al. Impact of maternal Vitamin A supplementation on the mother-infant pair in Brazil. Eur J Clin Nutr 2010;64:1302-7.
- Duerbeck NB, Dowling DD. Vitamin A: Too much of a good thing? Obstet Gynecol Surv 2012;67:122-8.
- WHO/Micronutrient Initiative. Safe Vitamin A Dosage during Pregnancy and Lactation. Recommendations and and Report of a Consultation. Geneva (Switzerland): WHO; 1998.
- Guillonneau M, Jacqz-Aigrain E. Teratogenic effects of Vitamin A and its derivates. Arch Pediatr 1997;4:867-74.
- Arnaud J, Fortis I, Blachier S, Kia D, Favier A. Simultaneous determination of retinol, alpha-tocopherol and beta-carotene in serum by isocratic high-performance liquid chromatography.J Chromatogr 1991;572:103-16.
- Winkles J, Lunec J, Deverill I. Enhanced-latex-agglutination assay for C-reactive protein in serum, with use of a centrifugal analyzer. Clin Chem 1987;33:685-9.
- Ledue TB, Poulin SE, Leavitt LF, Johnson AM. Evaluation of a particle-enhanced immunoassay for quantifying C-reactive protein. Clin Chem 1989;35:2001-2.
- Macy EM, Hayes TE, Tracy RP. Variability in the measurement of C-reactive protein in healthy subjects: Implications for reference intervals and epidemiological applications. Clin Chem 1997;43:52-8.
- de Onis M, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J, et al. Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Organ 2007;85:660-7.
- WHO. WHO Child Growth Standards: Length/Height-for- Age, Weight-for-Age and Body Mass Index-for-Age. Methods and Development. Geneva (Switzerland): WHO; 2006.
- Bresnahan KA, Tanumihardjo SA. Under nutrition, the acute phase response to infection, and its effects on micronutrient status indicators. Adv Nutr 2014;5:702-11.
- Soekarjo DD, Pee Sd Sd, Kusin JA, Schreurs WH, Schultink W, Muhilal, et al. Effectiveness of weekly Vitamin A (10,000 IU) and iron (60 mg) supplementation for adolescent boys and girls through schools in rural and urban East java, Indonesia. Eur J Clin Nutr 2004;58:927-37.
- Ahmed F, Rahman A, Noor AN, Akhtaruzzaman M, Hughes R. Anaemia and Vitamin A status among adolescent schoolboys in Dhaka city, Bangladesh. Public Health Nutr 2006;9:345-50.
- de Pee S, Dary O. Biochemical indicators of Vitamin A deficiency: Serum retinol and serum retinol binding protein. J Nutr 2002;132:2895S-901S.
- Vitolo MR, Gama CM, Queiroz SS, Lopez FA, Colugnati FA. Retinol blood levels in high school students of Sao Paulo, Brazil. Rev Nutr 2004;17:291-9.
- Baeten JM, Richardson BA, Bankson DD, Wener MH, Kreiss JK, Lavreys L, et al. Use of serum retinol-binding protein for prediction of Vitamin A deficiency: Effects of HIV-1 infection, protein malnutrition, and the acute phase response. Am J Clin Nutr 2004;79:218-25.
- Donnen P, Dramaix M, Brasseur D, Bitwe R, Bisimwa G, Hennart P, et al. The molar ratio of serum retinol-binding protein (RBP) to transthyretin (TTR) is not useful to assess Vitamin A status during infection in hospitalised children. Eur J Clin Nutr 2001;55:1043-7.
- Filteau SM, Morris SS, Abbott RA, Tomkins AM, Kirkwood BR, Arthur P, et al. Influence of morbidity on serum retinol of children in a community-based study in Northern Ghana. Am J Clin Nutr 1993;58:192-7.