Sizing it up: A Systematic Review of the Nosology of Muscle Dysmorphia
Douglas Blomeley1-3, Andrea Phillipou3-5,6, David J. Castle3,4,7
2.Department of Psychiatry, School of Medicine, Deakin University, Geelong, VIC, Australia.
3.Department of Psychiatry, St Vincent's Hospital, Melbourne, VIC, Australia.
4.Department of Psychiatry, the University of Melbourne, Melbourne, VIC, Australia.
5.Department of Mental Health, the Austin Hospital, Melbourne, VIC, Australia.
6.Centre for Mental Health, Swinburne University of Technology, Melbourne, VIC, Australia.
7.Faculty of Health Sciences, Australian Catholic University, Melbourne, VIC, Australia.
Citation : Blomeley D, Phillipou A, Castle DJ. Sizing it up: A Systematic Review of the Nosology of Muscle Dysmorphia. Clin Res Psychol 2018;1(1):1-10.
Muscle dysmorphia (MD), a condition in which the principal symptom is that of marked preoccupation with one's body being insufficiently muscular, has been the subject of considerable nosological debate in recent years.
The purpose of our systematic review is to examine the extant literature, with a focus on identifying the underlying psychopathology of MD, so as to allow accurate classification and determination of subsequent potential treatment implications. Electronic searches were performed within a date range of 2005-2015. We included only articles which employed assessments compatible with the criteria proposed by Pope et al.
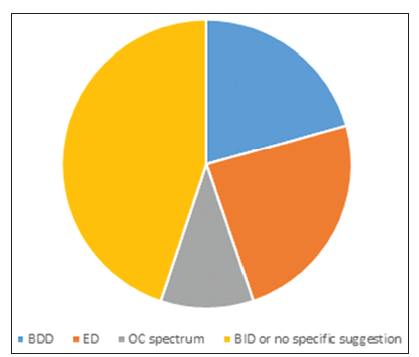
Our review encompassed a total of 29 papers, comprising cross-sectional or case report designs. Seven papers proposed MD be classified within the eating disorder spectrum, three papers favored an obsessive-compulsive spectrum classification, while six papers suggested classification within the body dysmorphic disorders. The remaining 13 papers either felt MD did not adequately fit within existing diagnostic categories or required creation of a new category of body image disorders (BID).
The centrality of body image disturbance in MD, in addition to its divergence from disorders within other diagnostic categories, suggests that creating a new category of BID would better reflect the psychopathology of MD, with additional potential benefits being increased validity of an MD diagnosis and subsequent development of targeted treatments.
Anorexia, bigorexia, body image, eating disorder, muscle dysmorphia, muscularity.
INTRODUCTION
A significant body of literature describes disorders characterized by a disturbance of body image, affecting both men and women to varying degrees. One such disorder, muscle dysmorphia (MD) has gained increasing recognition in recent years, both in the scientific literature and lay media. MD is a condition in which the principal symptom is that of marked preoccupation with one's body being insufficiently muscular, despite often being of above average muscularity and lean body mass. While certainly not a gender exclusive disorder, literature suggests that men are at significantly greater risk of developing MD than women. Originally conceptualized [1] as "reverse anorexia" due to the apparent behavioral and cognitive similarities with anorexia nervosa (AN), further research [2] resulted in the adoption of the term MD. The presence of pathological exercise behaviors aimed at increasing lean muscle mass was one of the features contributing to this conceptualization, with disordered eating being deemed a secondary characteristic.
From a nosological perspective, there has been increasing debate in the literature as to where MD best fits within current psychiatric classification systems. In the [3] Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5), it is currently classified as a subtype of body dysmorphic disorder (BDD). Various alternative suggestions have been put forward, including that MD may be best classified within existing categories of feeding and eating disorders (ED's), in view of MD's undeniable similarities with the ED's, particularly AN. Other suggestions have included placing MD within the grouping of obsessive-compulsive spectrum disorders. Indeed, some authors continue to question whether MD is a genuine disorder, despite it being a well-described entity.
The purpose of this paper is to present a systematic review of the extant, contemporary literature on MD, with a focus on interrogating the nosology, based on the features of the underlying psychopathology. We present a discussion on both treatment implications and future research directions and go on to suggest that MD may be best classified under a new category of body image disorders (BID).
METHODS
Electronic searches were performed in PubMed, PsycINFO, EMBASE, and The Cochrane Library. While descriptions of MD date back to as early as 1993, to maintain the contemporary nature of the investigation and discussion, the above databases were searched within a date range of 2005-2015, using the terms MD, bigorexia, reverse anorexia, and muscularity. Searching included all languages. Finally, reference lists of included studies were checked to identify as yet undiscovered publications which could then be assessed for suitability.
To examine the best available contemporary evidence on MD nosology, we included only articles which employed assessments compatible with the criteria proposed [2]. These encompassed the MD symptom questionnaire, MD disorder inventory, MD inventory, drive for muscularity scale, modified MD scale, and the MD questionnaire.
Articles which did not justify or explain the method of MD assessment/diagnosis were excluded, as were articles consisting of primarily of viewpoints/commentaries, reviews, and articles which were not deemed to be primarily related or applicable to MD.
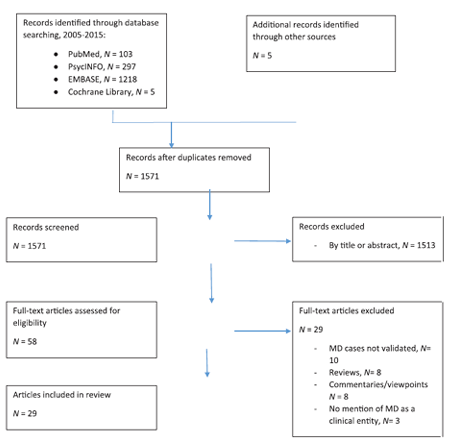
Titles and abstracts were initially read by the first author, whom also decided on inclusion and exclusion of papers based on the above-mentioned criteria. Some papers which did not meet criteria for the review were, however, considered to be rich in content and contributed to elements of the discussion (see below). First authors of the included papers were contacted as required to clarify methodology. From a total of 1576 records, 54 articles were fully assessed for eligibility, with 29 papers included in this review. Reasons for exclusion are shown in Figure 1.
Included studies were assessed for quality according to the National Health and Medical Research Council (NHMRC) recommendations, with included papers representing level IV evidence [4] due to being cross-sectional or case-report designs. No evidence of language bias was found, as searching was not limited to English.
RESULTS
Figure 1 shows the Preferred Reporting Items for Systematic reviews and Meta-analysis flowchart of the article searching and selection for this review. A total of 29 articles were included, with dates ranging from 2005 to 2015. A total of 29 full-text articles were excluded following full review for suitability. Many articles were excluded due to being commentary articles, reviews, or failing to specify the method of diagnosing MD. Finally, additional articles were excluded due to MD not being discussed at all throughout the paper.
The majority of studies compromised relatively small, non-clinical samples through a cross-sectional design. Six case reports were also included. In view of the absence of experimental or epidemiological study designs, the included articles represent Grade IV evidence according to the NHMRC guidelines [Table 1 (Table in PDF)].
Throughout our review, the highest reported prevalence of MD was 44%, found in a sample of 51 male weightlifters,[5] with the lowest reported prevalence in weightlifters being 13.6% [6]. This replicated the prevalence rates found by Alves dos Santos Filho et al.[7] in their 2016 review, reflecting the relatively scarce availability of prevalence data. Notably Bo et al.,[8] found in a sample of 440 college students that males were at a significantly greater risk than females of developing MD, with students of exercise and sports sciences courses at a 5-fold risk above baseline. Of the included studies, three included females [5,9,10]
The similarities between AN and MD have been extensively documented,[11-14] with a number of clear similarities evident from etiological, psychological, behavioral, and comorbidity perspectives, with this concept dating back to [1] original description of MD as "reverse anorexia." Seven papers (24.1%) in our review proposed MD be classified with the ED's.[9,15-19] In addition, from a psychological and behavioral perspective, a number of authors have previously described MD compulsions as being experienced as egosyntonic, again similarly to AN [20,21]. Further to this Kanayama and Pope,[22] suggest there may be a shared biological vulnerability between MD and AN. This has been further discussed by Benninghoven et al.[23] and Raevuori et al.,[24] through demonstration in twin studies, whereby cotwins of AN sufferers expressed significant MD symptomatology in addition to mood and anxiety symptoms. Given these extensive similarities, it is unsurprising that suggestions for classifying MD as an ED remain prominent.
Four papers favored an OC spectrum classification for MD,[8,9,25,31] representing 10.3% of literature included in our review. One of these studies, however,[8] suggested that females at risk of MD may show psychological profiles more closely resembling profiles seen in the ED's, whereas men may present with more obsessive-compulsive symptoms. In addition, a key finding by Tucker et al.[10] was the relationship between pressures to attain a sociocultural physique ideal and the development of MD, which may suggest a primary body image pathology.
Six papers suggested MD be placed with BDD, as it is at present,[5,26-30] one of these studies [29] found that in a sample of 95 men with BDD (25 of whom had MD), men with MD experienced poorer quality of life, had higher lifetime prevalence of substance use disorder (86% vs. 51%) and were significantly more likely to have attempted suicide (51% vs. 16%). Similarly Cafri et al.,[5] described greater functional impairment, more severe body dissatisfaction and body checking, and higher rates of mood and anxiety disorders in MD sufferers when compared to controls [26]. Furthermore, highlighted that variations of MD may present with a pathological pursuit of leanness, as opposed to muscularity, albeit while retaining as much lean muscle tissue as possible.
Thirteen papers [5,6,32-40] either suggested MD may be best classified as a BID or were unable to identify an appropriate nosology based on existent criteria.
A number of these studies found prominent body image dissatisfaction to be a core feature of MD - specifically Danilova et al.,[32] found that the perceived gap between the actual and ideal self when shown pictures of various physiques were significantly greater in men with high MD symptoms in comparison to men with low MD symptoms. These findings are also supported by Maida and Armstrong [25] who found symptoms of body distortion/dysmorphia to be stronger predictors of MD behaviors than were ED or obsessive-compulsive symptoms, despite the authors favoring an OC spectrum classification. Similarly Martin and Govender,[36] demonstrated that adherence to the masculine ideal was associated with significantly increased body image discrepancy and drive for muscularity.
Grieve et al.[33] found that men with higher levels of social physique anxiety (SPA) undertook exercise more for reasons of self-presentation and perceived image (muscularity) enhancement, as opposed to being motivated by physical fitness or recreational reasons. Further to this, men with higher levels of SPA also expressed higher levels of MD symptoms. It is important to note, however, that this was a correlational study; therefore, causality could not be determined, and it may be that the development of MD contributed to greater SPA. A number of additional correlates of SPA were also described in this study, including low self-esteem, low rates of participation in public exercise or social events, body image dissatisfaction, increased disordered eating, and prominent fear of negative evaluation of one's physique by others [11]. It was also noted that men with higher measures of self-objectification demonstrated greater drive for muscularity and expressed more MD symptomatology. Similar findings were evident in another study,[6] and while unable to suggest a classification, those authors found that subjects with MD showed high SPA and physique protection behaviors, in addition to a greater drive for muscularity and bulimic symptoms. Many of these findings were further replicated by Walker et al.,[39] who demonstrated a relationship between increased body checking behaviors (such as regularly checking one's reflection, feeling muscles for size, and tone and seeking reassurance from others about muscularity) and greater MD symptoms, in addition to higher rates of appearance and performance enhancing drug (APED) use.
Martin and Govender [36] found that adherence to masculine ideals was associated with increased body image discrepancy, and significantly increased drive for muscularity. Similarly Kuennen and Waldron,[35] found a significant relationship between muscularity and self-esteem. Interestingly, one study [27] described a number of male body image disturbance phenotypes with varying behaviors and presentations, although noted a drive for both muscularity and leanness to be at the core of all variations. However, these authors again favored a BDD classification for MD.
The use of the term "APED,"[27] also described as "body image drugs," [14,40] highlights that anabolic-androgenic steroids (AAS), and other illicit compounds are not simply used to enhance strength and performance but are used extensively by those with MD to attain muscularity and leanness. A number of authors have described AAS use in MD, [11,38,41,42] with estimates of >50% of sufferers having current or lifetime use of AAS [41]. Behar and Molinari, (2010), found AAS use in 42% of weightlifters with MD, and a general APED usage of 67% [27]. Highlighted the high rate of utilization of over the counter and illicit thermogenic compounds in MD. It seems logical that APED use in MD parallels the use of similar agents in AN, with their use in both disorders aimed at expediting the process of attaining an unrealistic appearance ideal, or compensating for a variation from the rigidly planned nutrition and/or exercise regimen.
DISCUSSION
This systematic review investigated the contemporary suggestions on the nosology of MD, in studies in which MD cases were appropriately validated. A number of studies assessed comorbidities and factors associated with the development of MD. Overall, the majority of papers reviewed either did not conclude that MD fits appropriately within any current DSM-5 category (despite its current classification), or did not suggest a classification see Figure 2, with many describing MD as a disorder of body image.
While a number of papers described body image disturbance as being at the core of MD psychopathology, it is important to note the absence of neurobiological research pertaining specifically to MD, with evidence coming from subjective surveys and experiments, such as participants selecting
representation of their true and ideal self, based on photos of varying physiques Phillipou et al.,[43] in their recent systematic review of neurobiological changes reported in individuals with AN, described many structural and functional brain differences such as alternations in neurotransmitter function, regional cerebral blood flow, glucose metabolism, volumetrics, and the blood oxygen level dependent response. In view of the clear similarities between AN and MD, it seems plausible that similar neurobiological correlates may be evident in subjects with MD. In addition to this, there are a number of clear links between MD, the ED's (particularly AN), and BDD, with many etiological, psychological, and behavioral similarities.
Despite the clear links and similarities with BDD and AN, MD seems to demonstrate unique elements in its presentation and behaviors that suggest it may represent a discrete entity. The increased presence of compulsive exercise and lower scores on measures of eating pathology (compared to men with AN);[13] provides an example of MD's divergence from the currently recognized ED's. In addition to this, MD demonstrates a clear pursuit of muscularity and leanness, as opposed to thinness. In terms of divergence from BDD, BDD presentations rarely include such significant disturbance in dietary and exercise behavior as that seen in MD, and indeed BDD diagnostic criteria suggest that at present, clinicians should determine whether a BDD presentation is better explained by an ED, with MD also showing greater comorbidity and functional impairment than "non-MD" BDD patients [29].
Treatments for MD currently focus on serotonergic antidepressants and cognitive behavioral therapy,[21,44] again notably similar to the ED's and BDD [18,22]. At present, there is a distinct lack of published data on specific MD treatments. Previous publications have described the difficulties in treating MD, including reluctance of sufferers to seek treatment due to the egosyntonic nature of beliefs and behaviors,[45] and their outward appearance often being that of a "healthy" individual [46].
Griffiths et al.[46] have previously suggested that placing MD within the ED category may result in males becoming even less likely to seek treatment, for fear of being labeled with a disorder which society continues to view as a primarily "female problem." Stigma against those with ED's is a recognized problem, with the male experience of ED pathology being no exception. Griffiths et al. suggested that some MD sufferers may internalize the experience of not having a "real illness," and maybe thus reluctant to seek treatment. In addition Menees et al.,[37] found that boys who were exposed to critical comments about their physiques from fathers and sports coaches were at increased risk for developing MD, thus paving the way for interventions at a population level, through delivery of education on, and awareness of MD, particularly to higher risk groups [47].
Enhancing the validity of an MD diagnosis through appropriate classification may assist in the development of more targeted treatments, both in severe and subclinical cases, as well as improving rates of treatment seeking, particularly by males. It is apparent that a vast number of subclinical cases of MD exist,[48] and while many of these cases would benefit from treatment, individuals may only be correctly diagnosed during assessment and treatment of another primary disorder or comorbidity, such anxiety or depressive disorder [21]. In addition, the aforementioned APED use adds a further layer of complexity to MD, and it is important that this is recognized and responded to within treatment approaches [49]. We suggest that placing MD within a diagnostic category which reflects its underlying pathology of body image disturbance (BID) may encourage further investigation into the underlying neurobiological processes evident in body image disturbance, and the subsequent development of targeted treatments.
This review has a number of limitations. First, despite relatively large numbers of empirical articles being available, the number of articles suitable based on our inclusion criteria is relatively small. Limiting the search range to 2005 onward may have contributed to this relatively small number; however, this strategy was chosen to allow interrogation of the contemporary literature and debates. In addition, the majority of included articles employed a cross-sectional design, with a small number of case reports included. Regardless, level of evidence for the included literature was level IV, representing the lowest level of the NHMRC evidence hierarchy. A minority of studies (three) included female subjects, with many studies also enrolling in non-clinical subjects. Selection and response bias may have been an additional factor in some samples, as many subjects were recruited from flyers and advertisements at universities and gymnasiums. Prevalence data for the general population were particularly scarce. Samples were generally from Western countries, with the majority from North America and Australia. In addition, many of the rating scales used in the reviewed articles (particularly in assessing eating pathology) were developed and validated in female ED samples - their utility in male subjects is questionable [50].
CONCLUSION
It is clear there is a significant need to further our understanding of the experience of muscularity oriented body image pathology, with our review further demonstrating the continuing uncertainty regarding the most fitting classification for MD. In view of the majority of reviewed studies describing MD either as a disorder of body image (currently a non-existent category in the DSM-5), or failing to suggest appropriate classification, when combined with the available evidence suggesting body image disturbance lays at the core of this disorder, we suggest MD would be best classified under a new category of "BID." MD's striking similarities with the ED's, particularly AN, would suggest this classification could also logically encompass the ED's, and indeed BDD and its variants, thereby better reflecting the shared underlying psychopathology of body image distortion. Future research on MD will need to utilize a variety of sample characteristics and validated symptom measures to determine who may be at risk for MD, in addition to bodybuilders and weightlifters. Further to this, we reiterate that exploring the underlying neurobiology of MD is crucial. In closing, we suggest this review allows us to extrapolate that disturbance of body image lays at the core of MD pathology, with other behavioral manifestations occurring secondary to this, and therefore we suggest it should be classified as such under the new heading of BID.
REFERENCES
- Pope HG Jr, Katz DL, Hudson JI. Anorexia nervosa and "reverse anorexia" among 108 male bodybuilders. Compr Psychiatry 1993;34:406-9.
- Pope HG Jr, Gruber AJ, Choi P, Olivardia R, Phillips KA. Muscle dysmorphia. An underrecognized form of body dysmorphic disorder. Psychosomatics 1997;38:548-57.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders V. Washington, DC: American Psychiatric Association; 2013.
- National Health and Medical Research Council. NHMRC Additional Levels of Evidence and Grades for Recommendations-Stage 2 Consultation. NHMRC; 2008. Available from:
http://www.nhmrc.gov.au/_files_nhmrc/file/ guidelines/stage_2_consultation_levels_and_grades.pdf. [Last accessed on 2018 Sep 06]. - Cafri G, Olivardia R, Thompson JK. Symptom characteristics and psychiatric comorbidity among males with muscle dysmorphia. Compr Psychiatry 2008;49:374-9.
- Hildebrandt T, Schlundt D, Langenbucher J, Chung T. Presence of muscle dysmorphia symptomology among male weightlifters. Compr Psychiatry 2006;47:127-35.
- Santos Filho CA, Tirico PP, Stefano SC, Touyz SW, Claudino AM. Systematic review of the diagnostic category muscle dysmorphia. Aust N Z J Psychiatry 2016;50:322-33.
- Bo S, Zoccali R, Ponzo V, Soldati L, De Carli L, Benso A, et al. University courses, eating problems and muscle dysmorphia: Are there any associations? J Transl Med 2014;12:221.
- Lamanna J, Grieve FG, Derryberry WP, Hakman M, McClure A. Antecedents of eating disorders and muscle dysmorphia in a non-clinical sample. Eat Weight Disord 2010;15:e23-33.
- Tucker R, Watkins PL, Cardinal BJ. Muscle dysmorphia, gender role stress, and sociocultural influences: An exploratory study. Res Q Exerc Sport 2011;82:310-9.
- Grieve R, Helmick A. The influence of men's self-objectification on the drive for muscularity: Self-esteem, body satisfaction and muscle dysmorphia. Int J Men's Health 2008;7:288-98.
- Hay PJ. What is an eating disorder? Implications for current and future diagnostic criteria. Aust N Z J Psychiatry 2012;47:208-11.
- Murray SB, Rieger E, Hildebrandt T, Karlov L, Russell J, Boon E, et al. A comparison of eating, exercise, shape, and weight related symptomatology in males with muscle dysmorphia and anorexia nervosa. Body Image 2012;9:193-200.
- Rohman L. The relationship between anabolic androgenic steroids use and muscle dysmorphia: A review. Eat Disord 2009;17:187-99.
- Mosley PE. Bigorexia: Bodybuilding and muscle dysmorphia. Eur Eat Disord Rev 2009;17:191-8.
- Murray SB, Griffiths S. Adolescent muscle dysmorphia and family-based treatment: A case report. Clin Child Psychol Psychiatry 2014;20:324-30.
- Murray SB, Maguire S, Russell J, Touyz SW. The emotional regulatory features of bulimic episodes and compulsive exercise in muscle dysmorphia: A case report. Eur Eat Disord Rev 2012;20:68-73.
- Murray SB, Rieger E, Karlov L, Touyz SW. An investigation of the transdiagnostic model of eating disorders in the context of muscle dysmorphia. Eur Eat Disord Rev 2013;21:160-4.
- Murray SB, Rieger E, Touyz SW. Muscle dysmorphia symptomatology during a period of religious fasting: A case report. Eur Eat Disord Rev 2011;19:162-8.
- Grieve FG. A conceptual model of factors contributing to the development of muscle dysmorphia. Eat Disord 2007;15:63-80.
- Grieve FG, Truba N, Bowersox S. Etiology, assessment and treatment of muscle dysmorphia. J Cogn Psychother: Int Quarterly 2009;23:306-14.
- Kanayama G, Pope HG Jr. Gods, men, and muscle dysmorphia. Harv Rev Psychiatry 2011;19:95-8.
- Benninghoven D, Tetsch N, Jantschek G. Patients with eating disorders and their siblings - an investigation of body image perceptions. Eur Child Adolesc Psychiatry. 2008;17:118-26.
- Raevuori A, Keski-Rahkonen A, Hoek HW, Sihvola E, Rissanen A, Kaprio J, et al. Lifetime anorexia nervosa in young men in the community: Five cases and their co-twins. Int J Eat Disord 2008;41:458-63.
- Maida DM, Armstrong L. The classification of muscle dysmorphia. Int J Men's Health 2005;4:73-91.
- Cafri G, Blevins N, Thompson JK. The drive for muscle leanness: A complex case with features of muscle dysmorphia and eating disorder not otherwise specified. Eat Weight Disord 2006;11:e117-8.
- Hildebrandt T, Alfano L, Langenbucher JW. Body image disturbance in 1000 male appearance and performance enhancing drug users. J Psychiatr Res 2010;44:841-6.
- Leone JE, Sedory EJ, Gray KA. Recognition and treatment of muscle dysmorphia and related body image disorders. J Athl Train 2005;40:352-9.
- Pope CG, Pope HG, Menard W, Fay C, Olivardia R, Phillips KA, et al. Clinical features of muscle dysmorphia among males with body dysmorphic disorder. Body Image 2005;2:395-400.
- Wolke D, Sapouna M. Big men feeling small: Childhood bullying experience, muscle dysmorphia and other mental health problems in bodybuilders. Psychol Sport Exerc 2008;9:595-604.
- Chandler CG, Grieve FG, Derryberry WP, Pegg PO. Are anxiety and obsessive-compulsive symptoms related to muscle dysmorphia? Int J Men's Health 2009;8:143-54.
- Danilova D, Diekhoff GM, Vandehey MA. A multidimensional scaling analysis of male body perception in men with muscle dysmorphia: The adonis complex. Int J Men's Health 2013;12:83-105.
- Grieve FG, Jackson L, Reece T, Marklin L, Delaney A. Correlates of social physique anxiety in men. J Sport Behav 2008;31:329-37.
- Grieve FG, Shacklette MD. Brief report on men's bodies and mood: Correlates between depressive symptoms and muscle dysmorphia symptoms. N Am J Psychol 2012;14:563-8.
- Kuennen MR, Waldron JJ. Relationships between specific personality traits, fat free mass indices, and the muscle dysmorphia inventory. J Sport Behav 2007;30:453-70.
- Martin J, Govender K. Making muscle junkies: Investigating traditional masculine ideology, body image discrepancy, and the pursuit of muscularity in adolescent males. Int Journal Men's Health 2011;10:220-39.
- Menees L, Grieve FG, Mienaltowski A, Pope J. Critical comments about the body and muscle dysmorphia symptoms in collegiate men. Int J Men's Health 2013;12:17-28.
- Thomas LS, Tod DA, Lavallee DE. Variability in muscle dysmorphia symptoms: The influence of weight training.J Strength Cond Res 2011;25:846-51.
- Walker DC, Anderson DA, Hildebrandt T. Body checking behaviors in men. Body Image 2009;6:164-70.
- Cafri G, van den Berg P, Thompson JK. Pursuit of muscularity in adolescent boys: Relations among biopsychosocial variables and clinical outcomes. J Child Adolesc Psychol 2006b;25:283-291.
- Contesini N, Adami F, Blake Md, Monteiro CB, Abreu LC, Valenti VE, et al. Nutritional strategies of physically active subjects with muscle dysmorphia. Int Arch Med 2013;6:25.
- Giardino JC, Procidano ME. Muscle dysmorphia symptomatology: A cross-cultural study in Mexico and the United States. Int J Men's Health 2012;11:83-103.
- Phillipou A, Rossell SL, Castle DJ. The neurobiology of anorexia nervosa: A systematic review. Aust N Z J Psychiatry 2014;48:128-52.
- Leone JE, Sedory EJ, Gray KA. Recognition and treatment of muscle dysmorphia and related body image disorders. J Athlet Train 2005;40:352-9.
- Phillipou A, Blomeley D, Castle DJ. Muscling in on body image disorders: What is the nosological status of muscle dysmorphia?Aust N Z J Psychiatry 2016;50:380-1.
- Griffiths S, Mond JM, Murray SB, Touyz S. Young peoples' stigmatizing attitudes and beliefs about anorexia nervosa and muscle dysmorphia. Int J Eat Disord 2014;47:189-95.
- Murray SB, Touyz SW. Masculinity, femininity and male body image: A recipe for future research. Int J Men's Health 2012c;11:227-39.
- Davey CM, Bishop JB. Muscle dysmorphia among college men: An emerging gender-related counselling concern. J Coll Counsell 2006;9:171-81.
- Russell J. Commentary on: Muscle dysmorphia: Towards a diagnostic consensus. Aust N Z J Psychiatry 2013;47:284-5.
- Hildebrandt T, Walker DC, Alfano L, Delinsky S, Bannon K. Development and validation of a male specific body checking questionnaire. Int J Eat Disord 2010;43:77-87.