Comparison of the Hypazotemic Effects of Erythropoietin and U-74389G on Urea Levels
Constantinos Tsompos1, Constantinos Panoulis2, Konstantinos Toutouzas3, Aggeliki Triantafyllou4, George C. Zografos3, Apostolos Papalois5, Kalliopi Tsarea5, Maria Karamperi5
2.Department of Obstetrics & Gynecology, Aretaieion Hospital, Athens University, Athens, Attiki, Hellas,Greece.
3.Department of Surgery, Ippokrateion General Hospital, Athens University, Athens, Attiki, Hellas,Greece.
4.Department of Biologic Chemistry, Athens University, Athens, Attiki, Hellas, Greece.
5. Department of Experimental Research Centre, ELPEN Pharmaceuticals, S.A. Inc., Co., Pikermi, Attiki, Hellas, Greece.
Citation : Tsompos C, Panoulis C, Toutouzas K, Triantafyllou A, Zografos GC, Papalois A, Tsarea K, Karamperi M. Comparison of the Hypazotemic Effects of Erythropoietin and U-74389G on Urea Levels.Clinic Res Urol 2018;1(1):1-6.
This study calculated the hypazotemic capacities of two drugs as follows: The erythropoietin (Epo) and the antioxidant drug U-74389G. The calculation was based on the results of two preliminary studies, each one of which estimated the hypazotemic influence, after the respective drug usage in an induced hypoxia-reoxygenation animal experiment.
The two main experimental endpoints at which the blood urea levels were evaluated the 60th reoxygenation min (for the groups A, C, and E) and the 120th reoxygenation min (for the groups B, D, and F). Especially, the groups A and B were processed without drugs, groups C and D after Epo administration whereas groups E and F after U-74389G administration.
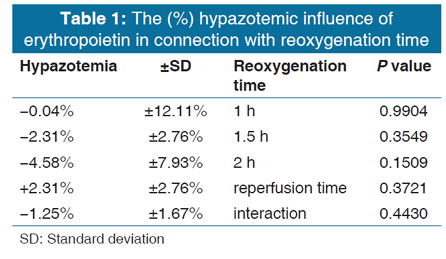
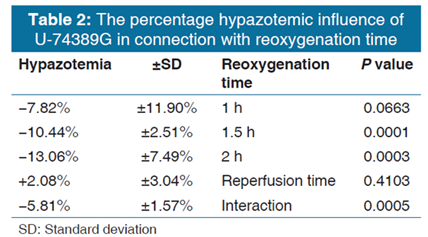
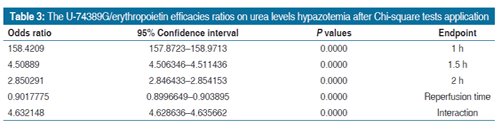
The first preliminary study of Epo presented a nonsignificant hypazotemic effect by 1.25% ± 1.67% (P = 0.4430). The second preliminary study of U-74389G presented a significant hypazotemic effect by 5.81% ± 1.57% (P = 0.0005). These two studies were co-evaluated since they came from the same experimental setting. The outcome of the co-evaluation was that U-74389G has 4.632148-fold more hypazotemic potency than Epo (P = 0.0000).
The antioxidant capacities of U-74389G enhance the acute hypazotemic properties presenting 4.632148-fold more intensive hypazotemia than Epo (P = 0.0000).
Erythropoietin, hypoxia, reoxygenation, U-74389G, urea levels
INTRODUCTION
U-74389G is not famous for its hypazotemic [1] capacity (P = 0.0005). U-74389G, as a novel antioxidant factor, implicates exactly only 256 published studies. The hypoxia-reoxygenation (HR) type of experiments was noted in 4.29% of these studies. A tissue-protective feature of U-74389G was obvious in these HR studies. The U-74389G chemically known as 21- [4-(2,6-di-1-pyrrolidinyl-4- pyrimidinyl)-1-piperazinyl]-pregna-1,4,9(11)-triene-3,20- dione maleate salt is an antioxidant complex, which prevents the lipid peroxidation either iron-dependent or arachidonic acid-induced one. Animal kidney, liver, brain microvascular endothelial cells monolayers, and heart models were protected by U-74389G after HR injury. U-74389G also attenuates the leukocytes, downregulates the proinflammatory gene, treats the endotoxin shock, produces cytokine, enhances the mononuclear immunity, protects the endothelium, and presents antishock property.
Erythropoietin (Epo) even whether is not famous for its hypazotemic action (P = 0.4430), it can be used as a reference drug for comparison with U-74389G. Although Epo is met in over 30,022 published biomedical studies, only a 10.53% of them negotiate the known type of HR experiments. Nevertheless, Epo as a cytokine, it is worth being studied about urea levels too.
This experimental work tried to compare the hypazotemic effects of the above drugs on a rat-induced HR protocol. They were tested by calculating the serum urea levels declines.
MATERIALS AND METHODS
The Vet licenses between 3693/12-11-2010 and 14/10-1-2012 numbers, the granting company and the experiment location are mentioned in preliminary references [1,2]. The human animal care of albino female Wistar rats, the 7 days preexperimental ad libitum diet, the nonstop intraexperimental anesthesiologic techniques, the acidometry, the electrocardiogram and the oxygen supply, and postexperimental euthanasia are also described in preliminary references. Rats were 16-18 weeks old. They were randomly assigned to six groups consisted of N = 10. The stage of 45 min hypoxia was common for all six groups. Afterwards, reoxygenation of 60 min was followed in group A; reoxygenation of 120 min in group B; immediate Epo intravenous (IV) administration and reoxygenation of 60 min in group C, immediate Epo IV administration and reoxygenation of 120 min in group D, immediate U-74389G IV administration and reoxygenation of 60 min in group E, and immediate U-74389G IV administration and reoxygenation of 120 min in group F. The dose height assessment for both drugs is described at preliminary studies as 10 mg/kg body mass.
Hypoxia was caused by laparotomic clamping the inferior aorta over renal arteries with forceps for 45 min. The clamp removal was restoring the inferior aorta patency and reoxygenation. After exclusion of the blood flow, the protocol of HR was applied, as described above for each experimental group. The drugs were administered at the time of reperfusion through inferior vena cava catheter. The urea levels were determined at 60th min of reoxygenation (for A, C, and E groups) and at 120th min of reoxygenation (for B, D, and F groups). However, the predicted urea values were used since a very powerful relation was raised with animals' mass (P = 0.0111).
Table 1 presents the (%) hypazotemic influence of Epo regarding reoxygenation time. Furthermore, Table 2 presents the (%) hypazotemic influence of U-74389G regarding reoxygenation time. Chi-square tests were applied using the ratios which produced the (%) results per endpoint. The outcomes of Chi-square tests are depicted in Table 3. The statistical analysis was performed by Stata 6.0 software (Stata 6.0, StataCorp LP, Texas, USA).
RESULTS
The successive application of Chi-square tests revealed that U-74389G accentuated the hypazotemia by 158.4209- fold (157.8723-158.9713) than Epo at 1 h, by 4.50889-fold (4.506346-4.511436) at 1.5 h, by 2.850291-fold (2.846433- 2.854153) at 2 h, by 0.9017775-fold (0.8996649-0.903895) without drugs, and by 4.632148-fold (4.628636-4.635662) whether all variables have been considered (P = 0.0000).
DISCUSSION
The unique available study investigating the hypazotemic effect of U-74389G on urea levels was the preliminary one [1]. Although the most famous activities of neuroprotection and membrane-stabilization properties, it accumulates the cell membrane, protecting vascular endothelium from peroxidative damage but hardly penetrates the blood-brain barrier. It elicits a beneficial effect in ototoxicity and Duchenne muscular dystrophy. It increases γ-glutamyltransferase, superoxide dismutase (SOD), and glutathione levels in oxygen-exposed cells. It treats septic states and acts as an immunosuppressant in flap survival. It prevents the learning impairments, and it delays the early synaptic transmission decay during hypoxia improving the energetic state of neurons. It shows antiproliferative properties on brain cancer cells and is considered as a new promising anti-inflammatory drug for the treatment of reperfusion syndrome in IR injuries.
The same authors confirmed [2] the short-term hypazotemic effect of Epo preparations in noniron-deficient individuals. Zeng et al. [3] noticed that blood urea nitrogen (BUN) was decreased by cyclic helical B-peptide derived from Epo in a dose-dependent fashion maybe through reducing caspase-3 activation, apoptosis, and inflammation in a mice model. Ma et al. levels showed [4] small but significant improvement of BUN than control treatment after the delivery of human Epo cDNA to salivary glands. Tajbakhsh et al. found [5] the postdialysis means of malondialdehyde, BUN, advanced glycation end product (AGE), and ox-low-density lipoprotein plasma level significantly decreased than predialysis level in chronic hemodialysis end-stage renal disease patients on maintenance treatment with Epo therapy. Saraji et al. found no significant relation between restless leg syndrome and dialysis adequacy, serum intact parathyroid hormone, and urea; whereas, Epo dosage and serum hemoglobin level were [6] lower. Koriem et al. found [7] significant increases in serum Epo and urea levels in 4-tert-octylphenol toxicity - an endocrine-disrupting chemical in rats. Yamazaki et al. found [8] no significant differences regarding the dose of darbepoetin and BUN between transplant and no transplant chronic kidney disease (CKD) dialysis recipients. Huang et al. found high blood lead level (BLL) 0.318-fold rarely in the group [9] with Epo than in the group without Epo. Clearance of urea was positively associated with log BLL in maintenance hemodialysis patients. Tahamtan et al. [10] could not reverse the increased level of BUN by Epo 24 h after reperfusion, but counteracted 7 days after bilateral renal ischemia in Wistar rats. Hertzberg-Bigelman et al. [11] reflected the elevated BUN, presence of anemia, and molecular changes in the Epo/ Epo-R axis in a severe renal failure rat model. Schaalan et al. found [12] a significant positive correlation between antimicrobial β-defensin-like role of hepcidin (HEPC) levels and BUN by 1.8- fold and decreased Epo levels by 77.8% in septic acute kidney injury (AKI) patients before and after treatment. Maduell et al.
significantly decreased blood urea nitrogen values increasing [13] the dialysis dose; whereas, there was a 50.4% of reduction in darbepoetin dose at 24 months and a significant decrease in the Epo resistance index in online hemodia filtration. Antwi- Bafour et al. [14] observed a significantly increased fasting blood urea by 1.45-fold and Epo levels also high as 54.0% in the cases than controls in renal insufficiency patients with poorly controlled diabetes. Xu et al. found no obvious changes of BUN [15] and Epo in either groups after sodium ferrous chlorophyll treatment of hemodialysis patients; whereas, Epo dosage was decreased more significantly than in the control group (P < 0.05). Vega et al. found the mean equivalent renal urea clearance at [16] 15.6 ± 4.2 mL/min and the Epo resistance index at 3.7 ± 2.1 IU/kg/week/g/dL in patients who received home hemodialysis. Ibrahim et al. [17] exhibited reduced serum levels of Epo and increases in the kidney function markers (urea and creatinine) in male Wistar rats of induced diabetes mellitus than control ones. Xue et al. showed [18] a significantly increasing similar trend (P < 0.05) for both Epo levels and BUN postoperatively in a rat model of chronic allograft nephropathy. Elshiekh et al. decreased [19] urea contents in the IR kidney after treatment with Epo or ischemic preconditioning (IPC). Liu et al. significantly decreased [20] serum expression levels of BUN markedly induced by renal ischemia-reperfusion injury after pretreatment with Epo and sodium selenite. Hirata et al. alleviated [21] the increasing urinary total protein excretion and plasma urea nitrogen, in a rat model of chronic progressive glomerulonephritis (GN), thereby delaying end-stage kidney disease after a single dose of epoetin beta pegol (continuous Epo receptor activator [CERA] given on day 1). Cakiroglu et al. improved [22] statistically nonsignificantly the serum urea particularly after daily Epo application in AKI rats. Phillips et al. suggested inefficient erythropoiesis in the presence of elevated Epo that is correlated [23] with plasma urea concentration in Lewis polycystic kidney CKD rodent model. Zhao et al. [24] calculated BUN levels less severe after administration of Epo at a dose of 3000 IU/kg once a week than the placebo group at day 21 (P < 0.01) in rats model of induced renal interstitial fibrosis. Banks conducted [25] isothermal urea denaturation experiments at numerous temperatures in the absence and presence of sodium chloride and indicated that salt stabilizes Epo primarily by increasing the difference in enthalpy between the native and unfolded sates. This result, and the finding that the salt induced increases in Epo, melting temperatures were independent of the identity of the salt cation, and anion indicates that salt likely increases the conformational stability of Epo at neutral pH by nonspecific shielding of unfavorable electrostatic interaction(s) in the native state. Attia et al. related high predialysis levels of BUN [26] with uremic pruritus, a common treatment of which includes also Epo in dialysis patients with chronic kidney disease. Bueno et al. noticed [27] increase in median Epo levels (P < 0.001) and urea (P = 0.039) in the evaluated period in chronic kidney disease patients. Yang et al. found [28] that nandrolone decanoate plus Epo may increase HCT by 2.54%; whereas, no evidence was found to indicate that decreased BUN than Epo alone. Reddy et al. documented [29] Epo dosage and urea reduction rate in maintenance hemodialysis patients per week. Dardashti et al. found [30] statistically no significant differences in p-urea and IV administration of a single high-dose (400 IU/ kg) Epo, without renal protective effect in patients with reduced kidney function undergoing coronary artery bypass surgery. Aydin et al. positively correlated prohepcidin with urea (P = 0.002) levels; whereas, HEPC generation [31] is also dependent on Epo levels in chronic kidney disease. Zhang et al.[32] maintained for < 1 week, the declines in Hb and BUN following the end of the treatment with chitosan-tripolyphosphate-Epo nanoparticles in an immunoglobulin A nephropathy (IgAN) rat model. Aizawa et al. suppressed [33] increased urea nitrogen after epoetin beta pegol (CERA) in Thy-1-GN rats. Arend et al. [34] considered the dose-dependent adverse effects of high darbepoetin treatment as elevated serum urea in nephrectomized apo E knockout mice. Ahmadiasl et al. significantly decreased [35] blood SOD, GPx, and urea levels and increased TAC level after treatment with Epo and MEL in renal IR injury of male rats. Nasri found [36] that Epo was able to prevent the increase in serum BUN. Thus, Epo is a promising kidney protective agent to prevent, ameliorate, or attenuate tubular damage induced by nephrotoxic agents in a study of male rats. Siribamrungwong et al. improved the nutritional status since BUN was increased [37] by 1.09% and Epo dosage requirement was decreased by 25%/week in peritoneal dialysis patients. Chrysikos DT et al. found serum urea not to differ [38] between the two groups of a swine model of pancreatic IR encompassing IPC and U-74389G effect. Alhan et al. inhibited [39] the significant increase in serum urea after the use of U-74389G in induced acute necrotizing pancreatitis in rats.
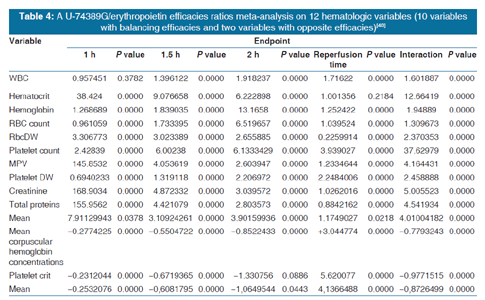
According to above, Table 3 shows that U-74389G accentuated by 4.632148-fold (4.628636- 4.635662) the hypazotemic potency than Epo (P = 0.0000); a trend attenuated along time, in Epo nondeficient rats. A meta-analysis of these ratios from the same experiment, for 12 other seric variables, provides comparable results [40] [Table 4].
CONCLUSION
The antioxidant agent U-74389G proved also more hypazotemic by 4.632148-fold (4.628636-4.635662) than Epo (P = 0.0000) in rats. However, this trend is attenuated along the short-term time frame of the experiment. A biochemical investigation is needed for the elucidation of this metabolic pathway.
ACKNOWLEDGMENT
This study was funded by Scholarship by the Experimental Research Center ELPEN Pharmaceuticals (E.R.C.E), Athens,Greece. The research facilities for this project were provided by the aforementioned institution.
REFERENCES
- Tsompos C, Panoulis C, Toutouzas K, Triantafyllou A, Zografos G, Papalois A. The effect of the antioxidant drug U-74389G on urea levels during ischemia reperfusion injury in rats. Ital J Med 2017;11:305-9.
- ?sompos C, Panoulis C, ??utouzas K, ?ografos G, Papalois A. The effect of erythropoietin on urea levels during ischemia reperfusion injury in rats. Lit J Pharm Drug Delivery Technol 2015;1:61-4.
- Zeng Y, Zheng L, Yang Z, Yang C, Zhang Y, Li J, et al. Protective effects of cyclic helix B peptide on aristolochic acid induced acute kidney injury. Biomed Pharmacother 2017;94:1167-75.
- Ma C, Fan Z, Gao Z, Wang S, Shan Z. Delivery of human erythropoietin gene with an adeno-associated virus vector through parotid glands to treat renal anaemia in a swine model. Gene Ther 2017;24:692-8.
- Tajbakhsh R, Qorbani M, Mehrpour G, Rahimzadeh M, Azimzadeh MM, Mirmiranpour H, et al. Effect of hemodialysis on oxidants and antioxidant factors in chronic renal failure. Saudi J Kidney Dis Transpl 2017;28:507-16.
- Saraji NZ, Hami M, Boostani R, Mojahedi MJ. Restless leg syndrome in chronic hemodialysis patients in Mashhad hemodialysis centers. J Renal Inj Prev 2016;6:137-41.
- Koriem KMM, Arbid MSS, Gomaa NE. The role of chlorogenic acid supplementation in anemia and mineral disturbances induced by 4-tert-octylphenol toxicity. J Diet Suppl 2018;15:55-71.
- Yamazaki K, Sakai K, Ohashi Y, Nihei H, Itabashi T, Muramatsu M, et al. Similar anemic control between chronic kidney diseases in patients with and without transplantation on entry to dialysis. Transplant Proc 2017;49:57-60.
- Huang WH, Hsu CW, Weng CH, Lin-Tan DT, Yen TH. Negative relationship between erythropoietin dose and blood lead level in patients undergoing maintenance hemodialysis. Sci Rep 2016;6:34313.
- Tahamtan M, Moosavi SM, Sheibani V, Nayebpour M, Esmaeili-Mahani S, Shabani M, et al. Erythropoietin attenuates motor impairments induced by bilateral renal ischemia/ reperfusion in rats. Fundam Clin Pharmacol 2016;30:502-10.
- Hertzberg-Bigelman E, Barashi R, Levy R, Cohen L, Ben- Shoshan J, Keren G, et al. Down-regulation of cardiac erythropoietin receptor and its downstream activated signal transducer phospho-STAT-5 in a rat model of chronic kidney disease. Isr Med Assoc J 2016;18:326-30.
- Schaalan MF, Mohamed WA. Determinants of hepcidin levels in sepsis-associated acute kidney injury: Impact on pAKT/ PTEN pathways? J Immunotoxicol 2016;13:751-7.
- Maduell F, Ojeda R, Arias-Guillen M, Rossi F, Fontsere N, Vera M, et al. Eight-year experience with nocturnal, every-otherday, online haemodiafiltration. Nephron 2016;133:98-110.
- Antwi-Bafour S, Hammond S, Adjei JK, Kyeremeh R, Martin- Odoom A, Ekem I. A case-control study of prevalence of anemia among patients with Type 2 diabetes. J Med Case Rep 2016;10:110.
- Xu XF, Hu JP, Cheng X, Yu GJ, Luo F, Zhang GS, et al. Effects of sodium ferrous chlorophyll treatment on anemia of hemodialysis patients and relevant biochemical parameters. J Biol Regul Homeost Agents 2016;30:135-40.
- Vega A, Sequi MJ, Abad S, Yuste C, Santos A, Macias N, et al. Daily home hemodialysis is an available option for renal replacement therapy in Spain. Ther Apher Dial 2016;20:408-12.
- Ibrahim ZS, Alkafafy ME, Ahmed MM, Soliman MM. Renoprotective effect of curcumin against the combined oxidative stress of diabetes and nicotine in rats. Mol Med Rep 2016;13:3017-26.
- Xue D, Zhou C, Shi Y, Lu H, He X. Hepcidin as a biomarker of impaired renal function in rat models for chronic allograft nephropathy. Med Sci Monit 2016;22:608-16.
- Elshiekh M, Kadkhodaee M, Seifi B, Ranjbaran M, Ahghari P. Ameliorative effect of recombinant human erythropoietin and ischemic preconditioning on renal ischemia reperfusion injury in rats. Nephrourol Mon 2015;7:e31152.
- Liu L, Liu C, Hou L, Lv J, Wu F, Yang X, et al. Protection against ischemia/reperfusioninduced renal injury by cotreatment with erythropoietin and sodium selenite. Mol Med Rep 2015;12:7933-40.
- Hirata M, Tashiro Y, Aizawa K, Kawasaki R, Shimonaka Y, Endo K. Epoetin beta pegol alleviates oxidative stress and exacerbation of renal damage from iron deposition, thereby delaying CKD progression in progressive glomerulonephritis rats. Physiol Rep 2015;3:pii: e12637.
- Cakiroglu F, Enders-Comberg SM, Pagel H, Rohwedel J, Lehnert H, Kramer J, et al. Erythropoietin-enhanced endothelial progenitor cell recruitment in peripheral blood and renal vessels during experimental acute kidney injury in rats. Cell Biol Int 2016;40:298-307.
- Phillips JK, Boyd R, Krockenberger MB, Burgio G. Progression of anemia and its relationship with renal function, blood pressure, and erythropoietin in rats with chronic kidney disease. Vet Clin Pathol 2015;44:342-54.
- Zhao XF, Liu YH, Han ZM, Xu YU. Effect of erythropoietin on the expression of dynamin-related protein-1 in rat renal interstitial fibrosis. Exp Ther Med 2015;9:2065-71.
- Banks DD. Nonspecific shielding of unfavorable electrostatic intramolecular interactions in the erythropoietin nativestate increase conformational stability and limit non-native aggregation. Protein Sci 2015;24:803-11.
- Attia EA, Hassan AA. Uremic pruritus pathogenesis, revisited. Arab J Nephrol Transplant 2014;7:91-6.
- Bueno CS, Frizzo MN. Anemia in chronic kidney disease in a hospital in the Northwest region to the State of Rio Grande do Sul. J Bras Nefrol 2014;36:304-14.
- Yang Q, Abudou M, Xie XS, Wu T. Androgens for the anaemia of chronic kidney disease in adults. Cochrane Database Syst Rev 2014;10:CD006881.
- Reddy YN, Abraham G, Reddy YN, Nagarajan P, Matthew M, Jayaseelan T, et al. Mineral bone disease in maintenance hemodialysis patients: Association with morbidity and mortality. Indian J Nephrol 2014;24:302-7.
- Dardashti A, Ederoth P, Algotsson L, Bronden B, Grins E, Larsson M, et al. Erythropoietin and protection of renal function in cardiac surgery (the EPRICS Trial). Anesthesiology 2014;121:582-90.
- Aydin Z, Gursu M, Karadag S, Uzun S, Sumnu A, Doventas Y, et al. The relationship of Prohepcidin levels with anemia and inflammatory markers in non-diabetic uremic patients: A controlled study. Ren Fail 2014;36:1253-7.
- Zhang X, Wu Y, Sun K, Tan J. Effect of erythropoietin loading chitosan-tripolyphosphate nanoparticles on an igA nephropathy rat model. Exp Ther Med 2014;7:1659-62.
- Aizawa K, Tashiro Y, Hirata M, Takeda S, Kawasaki R, Endo K, et al. Renoprotective effect of epoetin beta pegol by the prevention of M2 macrophage recruitment in thy-1 rats. J Nephrol 2014;27:395-401.
- Arend N, Hilgers KF, Campean V, Karpe B, Cordasic N, Klanke B, et al. Darbepoetin alpha reduces oxidative stress and chronic inflammation in atherosclerotic lesions of apo E deficient mice in experimental renal failure. PLoS One 2014;9:e88601.
- Ahmadiasl N, Banaei S, Alihemati A, Baradaran B, Azimian E. Effect of a combined treatment with erythropoietin and melatonin on renal ischemia reperfusion injury in male rats. Clin Exp Nephrol 2014;18:855-64.
- Nasri H. Renal cell protection of erythropoietin beyond correcting the anemia in chronic kidney disease patients. Cell J 2014;15:378-80.
- Siribamrungwong M, Yothasamutr K, Puangpanngam K. Periodontal treatment reduces chronic systemic inflammation in peritoneal dialysis patients. Ther Apher Dial 2014;18:305-8.
- Chrysikos DT, Sergentanis TN, Zagouri F, Psaltopoulou T, Theodoropoulos G, Flessas I, et al. Lazaroid U-74389G administration in pancreatic ischemia-reperfusion injury: A swine model encompassing ischemic preconditioning. JOP 2015;16:176-84.
- Alhan E, Turkyilmaz S, Ercin C, Kural BV. Effects of lazaroid U-74389G on acute necrotizing pancreatitis in rats. Eur Surg Res 2006;38:70-5.
- Tsompos C, Panoulis C, ??utouzas K, Triantafyllou A, Zografos CG, Papalois A. Comparison of the hypoproteinemic capacities of erythropoietin and U-74389G. J Genes Proteins 2018;1:1.