Bladder Adenocarcinoma Easily Mistaken for a Urachal Carcinoma: A Case Report
J. P. Omana Wembonyama, Tenkorang Somuah, Ahsaini Mustapha, Mellas Soufiane, El Ammari Jalal Eddine, Tazi Mohammed Fadl, El Fassi Mohammed Jamal, Farih Moulay Hassanr
Citation : Wembonyama JPO, Somuah T, Mustapha A, Soufiane M, Eddine EAJ, Fadl TM, Jamal EFM, Hassan FM. Bladder Adenocarcinoma Easily Mistaken for a Urachal Carcinoma: A Case Report. Clin Res Urol 2018;1(1):1-3.
Primary adenocarcinoma (ADK) of the bladder is a rare and aggressive form of bladder tumors. This affection represents < 2% of all tumors of the bladder. This tumor which has not been well studied can present features similar to that of urachal carcinoma and that can possibly be unidentified on the computed tomography (CT) scan. Its clinical latency renders its prognosis pejorative. The objective of this case report is to analyze the epidemiological, clinical, radiological, and therapeutic characteristics of this affection. This is a 54-year-old Moroccan male patient with no significant pathological history. This patient complained of a terminal hematuria that had only occurred once. The bladder ultrasound objectified a hyperechoic mass localized on the anterior wall of the bladder. The CT scan performed showed a tissue mass lesion with endo- and exo-luminal development arising from the anterior bladder wall measuring 33 mm * 30 mm suggesting a urachal neoplasia. The management of this affection consisted of a partial cystectomy with en bloc resection of the urachal ligament involving the bladder dome and the umbilicus with lymph node dissection. The anatomopathological analysis of the surgical specimen found a moderately differentiated ADK of the bladder staged T3N0M0. This tumor is known to be resistant to radiochemotherapy. However, a remedial approach by performing a radical cystoprostatectomy was proposed to our patient. Primary ADK of the bladder is a rare and an aggressive form of all bladder tumors. This tumor has a pejorative prognosis. It can be present itself as a urachal carcinoma and can easily be mistaken during imaging investigations such on the CT scan. The management of this affection demands surgery and consists of a radical cystectomy since the tumor is radio-chemo resistant.
Adenocarcinoma, bladder, computed tomography, urachus,Urology
INTRODUCTION
Primary adenocarcinoma (ADK) of the bladder is a rare tumor that occurs in < 2% of bladder cancers and accounts for 10-20% of all bladder ADKs. This tumor rapidly invades adjacent organs and remains very aggressive. If not diagnosed early, this tumor evolves very fast with a pejorative prognosis. Radical surgical treatment at a localized stage remains the only possibility for a better patient survival rate.
PRESENTATION DE CAS
A 54-year-old Moroccan male patient, who is married with no children, presented with a 1st time terminal hematuria associated with bladder irritative symptoms notably urinary frequency and painful urination. The patient had no significant medical history.
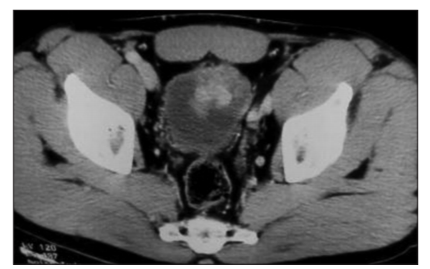
The patient had already performed a bladder ultrasound which objectified a hyperechoic mass localized on the anterior wall of the bladder. We performed a computed tomography thoraco-abdomino-pelvic (CT TAP) scan which showed a tissue mass lesion arising from the anterior wall of the bladder with an endo- and exo-luminal development measuring 33 mm * 30 mm in diameter suggestive of a neoplasia of the urachus with no signs of locoregional and distant invasion [Figures 1 and 2]. No other tumors notably that of the gastrointestinal tract or that of the lungs were objectified. Laboratory tests including urinalysis were all within their normal ranges. The urine culture was negative.

We programmed the surgery beginning with cystoscopy under general anesthesia to map out the lesion as well as any abnormal zones in the bladder. The patient finally underwent a partial cystectomy with en bloc resection of the urachal ligament involving the bladder dome and the umbilicus with lymph node dissection.
Anatomopathology analysis of the surgical specimen found an ADK of the bladder staged pT3N0M0. We decided and discussed with the patient to perform cystoprostatectomy as primary bladder ADK is known not to respond very well to radiotherapy and chemotherapy.
2-month post-operative follow-up cystoscopy revealed a tumor recurrence arising from the anterior wall of the bladder. CT TAP objectified the same tissue mass lesion on the anterior wall of the bladder. However, we could not perform the proposed cystoprostatectomy during surgery as the tumor had locally invaded adjacent organs. We, therefore, performed a Bricker ileal conduit urinary diversion as a palliative procedure. The patient was referred to the department of oncology for complementary care.
DISCUSSION
Primary bladder ADK accounts for 0.5-2% of malignant bladder tumors[1,2]. 2/3 of these tumors are located on the dome of the bladder and develop from the urothelial mucosa, secondarily to a phenomenon of metaplasia; the remaining third derives from the urachus[3]. This pathology has a very high incidence in populations exposed to schistosomiasis, where it was evaluated at 9.9% of malignant tumors of the bladder[4,5].
Macroscopic hematuria is present in 65-87% of cases. Irritative bladder symptoms are more common (45%) in primary bladder ADKs than in tumors of the urachus. Irritations and chronic infections contribute to the development of metaplasia which degenerates into ADK[3,6]. This is similar to our patient's case.
Abdominopelvic CT scan was essential to discuss the diagnosis and to evaluate tumor extension in the bladder, the lymph nodes, and distant metastasis. However, the CT scan can be misleading based on the localization and the endo and exo-luminal evolution of the tumor as this occurred in our case. Anatomopathological analysis of the specimen after a partial cystectomy concluded the diagnosis of the moderately differentiated primary ADK of the bladder but not that of the urachus. Anatomopathological classification of primary bladder ADK has been proposed being either[7]:
1. Glandular carcinoma.
2. Colloid carcinoma.
3. Papillary ADK.
Signet-ring cell carcinoma. Immunohistochemical analysis is important to differentiate between primary and secondary ADK of the bladder (most often, invasion by colorectal tumor)[7]. Wang has shown that dysregulation of Wnt/β-catenin allows this differentiation: Its nuclear expression is positive in colorectal tumors invading the bladder and negative in primary bladder ADKs[8].
From the therapeutic point of view, total cystoprostatectomy is the most widely used treatment in the literature with variable 5-year survival rate ranging from 0 to 80%, with an average value of 35% at all pathological stages[2,10-17]. Hatch reported the case of a patient, with local recurrence of ADK after two partial cystectomies, who had with no recurrence after chemotherapy using 5-fluorouracil (5-FU).
These results show the interest of chemotherapy for the treatment of primary bladder ADK, but its combination with other treatments, in particular, total cystectomy, has not been evaluated.
Partial cystectomy is proposed when the tumor is located on the mobile part of the bladder. Post-operative results are most often very bad, even if the number of reported cases is low and the decline is short[1,3,18]. Paradoxically, Anderstrom reported a 5- year survival of 54% in 15 patients treated with partial cystectomy[2]. However, this author also reports a survival of 21% in seven patients treated with neoadjuvant irradiation and partial cystectomy.
Primary bladder ADK is classically considered radiation resistant, and it is not surprising that patients treated with radiotherapy had a bad result.
Thomas and Anderstrom reported 5-year survival being < 20% in patients treated with radiotherapy alone[2,14]. For Gill, mean survival was 13 months after this treatment[19]. The use of systemic chemotherapy is very limited in the literature. From the results obtained for colon ADK, 5-FU-based chemotherapy has been proposed in all publications.
Nevin treated four patients with intra-arterial chemotherapy: Two full responses were obtained with a follow-up of 30 and 40 months (without further treatment), a partial response, and a lack of response[20]. Logothetis treated eight T4 tumors patients through intravenous or intra-arterial chemotherapy using 5-FU. Only one complete response was obtained with 11-month survival[9].
CONCLUSION
L'Adenocarcinome primitif de la vessie est une forme rare, agressive et ne represente que 2% de l'ensemble des tumeurs de vessie dont l'evolution est pejorative pretant confusion avec l'ADK de l'ouraque a l'imagerie medicale au moment de diagnostic dont (TDM trompeuse).
Le traitement est chirurgical et consiste a une cystectomie partielle, vu que la tumeur est radio-chimio resistante. Toute fois, une chimiotherapie adjuvante a base de 5-FU peut etre proposee.
REFERENCES
- Bennett JK, Wheatley JK, Walton KN. 10-year experience with adenocarcinoma of the bladder. J Urol 1984;131:262-5.
- Thomas DG, Ward AM, Williams JL. A study of 52 cases of adenocarcinoma of the bladder. Br J Urol 1971;43:4-15.
- Grignon DJ, Ro JY, Ayala AG, Johnson DE, Ordonez NG. Primary adenocarcinoma of the urinary bladder. A clinicopathologic analysis of 72 cases. Cancer 1991;67:2165-72.
- el-Boulkany MN, Ghoneim MA, Mansour MA. Carcinoma of the bilharzial bladder in Egypt. Clinical and pathological features. Br J Urol 1972;44:561-70.
- EL-Sebai L. Cancer of the bladder in Egypt. Kasr El-Aini J Surg 1961;2:183-241.
- Mostofi FK. Potentialities of bladder epithelium. J Urol 1954;71:705-14.
- Fiter L, Gimeno F, Martin L, Gomez-Tejeda L. Signet-ring cell adenocarcinoma of bladder. Urology 1993;41:30-3.
- Wang HL, Lu DW, Yeriam LM, Alsikafi N, Steinberg G, Hart J, Yang XJ. Immunohistochemical distinction between primary adenocarcinoma of the bladder and secondary colorectal adenocarcinoma. Am J Surg Pathol 2001;25:1380-7.
- Logothetis CJ, Samuels MI, Ogden S. Chemotherapy for adenocarcinomas of bladder and urachal origin: 5-Fluorouracil, doxorubicin and mitomycin-C. Urology 1985;26:252-5.
- Hatch TR, Fuchs EF. Intra-arterial infusion of 5-fluorouracil for recurrent adenocarcinoma of bladder. Urology 1989;33:311-2.
- Abenoza P, Monivel C, Fraley E. Primary adenocarcinoma of the urinary bladder. A clinico-pathologic study of 16 cases. Urology 1987;31:9-14.
- Anderstrom C, Johansson SL, von Schultz L. Primary adenocarcinoma of the urinary bladder. A clinicopathologic and prognostic study. Cancer 1983;52:1273-80.
- Dandekar NP, Dalal AV, Tongaonkar HB, Kamat MR. Adenocarcinoma of bladder. Eur J Surg Oncol 1997;23:157-60.
- EL-Mekresh MM, EL-Baz MA, Abol-enein H, Ghoneim MA. Primary adenocarcinoma of the urinary bladder: A report of185 cases. Br J Urol 1998;82:206-12.
- Kramer S, Bredael J, Croker B, Paulson D, Glenn J. Primary non-urachal adenocarcinom a of the bladder. J Urol 1979;121:278-81.
- Malek RS, Rosen J, O'dea M. Adenocarcinoma of the bladder. Urology 1983;21:357-9.
- Nocks B, Heney N, Daly J. Primary adenocarcinoma of urinary bladder. Br J Urol 1983;64:138142.
- Gill HS, Dhillon HK, Woodhouse CR. Adenocarcinoma of the urinary bladder. Br J Urol 1989;64:138-42.
- Nevin JE, Elnick IM, Rly JT, Easley CA, Landes R. Advanced carcinoma of the bladder: Treatment using hypogastric artery infusion with 5-fluorouracil, either as a single agent or in combination with bleomycin or adriamycin and super voltage radiation. J Urol 1974;112:752-8.
- Soulie M, Mouly P, Plante P, Escourrou G, Pontonnier F. Adenocarcinome vesical primitif a cellules enbague a chaton. A propos de 1 cas. Revue de la litterature. Prog Urol 1993;3:677-82.