A Case of Formalin Instillation Secondary to Refractory Gross Hematuria in a Patient with Radiation Cystitis
Kevin F. Carocci1, Jason Levy2, Dany Hanna2, Daniel Edwards2, Michael Nordsiek2, Brian McGreen2, Paulette Dreher2, Laurence Belkoff2
2.Department of Urology, Hahnemann University Hospital, Department of Urology, 230 North Broad Street, Philadelphia, PA 19102, USA.
Citation : Carocci KF, Levy J, Hanna D, Edwards D, Nordsiek M, McGreen B, Dreher P, Belkoff L. A Case of Formalin Instillation Secondary to Refractory Gross Hematuria in a Patient with Radiation Cystitis. Clinic Res Urol 2018;1(1):1-4.
Gross hematuria has several different etiologies, and as such, the process of working up a patient presenting with bleeding follows an outlined algorithm. The instillation of formalin, a caustic substance that hydrolyzes proteins and coagulates tissues, is a possible treatment option only when patients have failed previous preceding therapeutic steps. In our case, a 69-year-old African-American male presented with an acute episode of gross hematuria that did not resolve following several diagnostic and therapeutic steps. His hospital course was complicated by a steadily dropping hemoglobin, requiring many blood transfusions throughout his care. He was successfully treated with intravesical instillation of formalin following cystoscopy, transurethral resection of the prostate, and cystogram in the operating room. Thoughtful discussion regarding a treatment course in a patient with refractory gross hematuria deserves consideration.
Amicar, gross hematuria, hemorrhagic cystitis, intravesical formalin, percutaneous nephrostomy tube, radiation cystitis, superior vesical artery embolization.
INTRODUCTION
Patients presenting with gross hematuria can have a variety of etiologies. Treatment could be as simple as bladder irrigation or as extreme as a cystectomy. The American urological association recommends that a patient presenting with gross hematuria undergo cystoscopy, urine cytology, and upper urinary tract imaging (i.e., computerized tomography urogram) [1]. If an etiology is not identified and/or a patient continues to bleed, subsequent steps must be taken to achieve hemostasis.
Radiation cystitis describes the side effect of inflammation and subsequent destruction to the normal anatomy of the urinary bladder at the cellular level after the use of radiation in the treatment of multiple cancer types including, most commonly, pelvic cancers [2]. Patients can experience one or multiple lower urinary tract symptoms (i.e., frequency, urgency, and dysuria) as a side effect of pelvic radiation. However, this state of radiation-induced inflammation can also lead to microscopic and gross hematuria. Hemorrhagic cystitis is a condition of persistent bladder bleeding [3]. When a patient experiences intractable bleeding that does not respond to conservative approaches, one must consider one of several chemical bladder instillations. Intravesical formalin serves as the next best treatment option when a patient receives an instillation treatment with Amicar or alum without resolution of symptoms. One would possibly turn to formalin in a clinically stable patient who is still experiencing hematuria.
The use of formalin, however, has not been widely discussed in the literature. The first reported formalin treatment dates back to 1969, where it was used in the management of refractory bladder hemorrhage from inoperable cancer [4]. Donahue and Frank published an analysis review of 235 patients treated with intravesical formalin in 1989. They identified morbidity and mortality associated with differing concentrations of formalin as it applied to specific etiologies of hemorrhagic cystitis [5]. Since then, various case reports have discussed its use in refractory cases of gross hematuria. In a cohort study published more recently in 2017, Ziegelmann et al. echoes the scarcity of clinical data in support of intravesical formalin use. Their study looked at 104 patients who were hospitalized over a 10-year period for hemorrhagic cystitis. Of the 104 patients, eight patients were treated with intravesical formalin [4].
We report a case of formalin instillation in a patient with a history of radiation therapy following a previous diagnosis of prostatic adenocarcinoma.
CASE REPORT
A 69-year-old African-American male presented to our hospital emergency department with painless gross hematuria 3 h before arrival. While in the emergency department, an 18-French 3-way hematuria catheter was placed, and he received continuous bladder irrigation with resolution of the hematuria. He endorsed slight dysuria and incomplete bladder emptying and denied history of previous blood in his urine.
The patient's history was significant for mechanical mitral and aortic valves secondary to rheumatic heart disease, embolic cerebrovascular accident with residual right-side deficits, and prostate cancer status post external beam radiation therapy in 2007. In addition, he has an extensive history of tobacco use. He denied a family history of genitourinary pathology. His home medications included aspirin 81 mg, terazosin 2 mg, and warfarin 5 mg. He was stable and afebrile with a hemoglobin of 11.8 g/dL. The urology service was consulted. His catheter was upsized to a 22-French 3-way hematuria catheter and his bladder was copiously irrigated to clear following 4 L of 0.9% sodium chloride solution.
Over the next 30 days, he underwent a series of therapeutic interventions for continued gross hematuria.
First, he underwent a cystoscopy with clot evacuation and fulguration, followed by continuous bladder irrigation. Imaging with a computed tomography abdomen and pelvis with and without contrast showed an empty bladder with non-specific wall thickening. He later went into acute urinary retention requiring subsequent Foley catheter placement, clot irrigation, and continuous bladder irrigation. On post-operative day #3 status post-cystoscopy, 1% intravesical alum was instilled. He experienced bladder pain following instillation, which was resolved with Ditropan and belladonna opium suppositories. Blood transfusions were continuously being administered per the primary care team, as his hemoglobin routinely dropped < 7 g/dL. Our patient eventually received a central venous catheter for hemodynamic support. A transfer to the medical intensive care unit ensued due to his downtrending hemoglobin and hypotension requiring the use of vasopressors. An abdominal ultrasound showed no evidence of hemorrhage.
Since the patient continued to have hematuria with a dropping hemoglobin following cystoscopy with clot evacuation and fulguration, continuous bladder irrigation, and alum instillation, the next step was intravesical instillation of Amicar. The patient continued to bleed, and therefore, a discussion to proceed with possible embolization of the bladder, formalin instillation, or nephrostomy diversion ensued. Interventional radiology embolized bilateral superior vesical arteries without complication. He continued to require blood transfusions. 2 days following the embolization procedure, he had bilateral percutaneous nephrostomy tubes placed to divert the urine from his bladder. The patient's hemoglobin continued to drop by approximately 1 g daily, leading to a discussion for more aggressive management in the form of formalin instillation versus simple cystectomy.
A decision was made to take the patient to the operating room to perform intravesical instillation of formalin. First, a cystoscopy with clot evacuation was performed. The bladder neck was severely contracted, limiting visualization with the resectoscope, leading to the transurethral resection of the bladder neck and prostate to allow for intravesical mobility of the resectoscope and completion of clot evacuation. A cystogram was performed with Cystografin contrast, and no extravasation or vesicoureteral reflux was noted under fluoroscopy imaging. 200 mL of 3% formalin was then instilled through a 22-French Foley catheter into the bladder and allowed to sit for 8 min. After conclusion of the formalin instillation, we drained the formalin and ran saline continuous bladder irrigation through the bladder for approximately 8 min. The bladder was then drained, and at the Foley catheter was removed as it would likely irritate the bladder lining and cause additional bleeding. He was transferred to the post-operative care unit in stable condition. The patient's percutaneous nephrostomy tubes remained in place as the primary source of urine drainage.
Following this procedure, the patient was hemodynamically stable and did not complain of bladder pain. His hemoglobin stabilized following formalin instillation. A Texas catheter was later placed as he began to void spontaneously. Bilateral percutaneous nephrostomy tubes continued to drain clear, yellow urine and were removed following successful voiding trials.
DISCUSSION
Gross hematuria can be associated with a wide range of differential diagnoses. It is, therefore, imperative to get an accurate and detailed history from someone with this presentation. This will help to direct management of care.
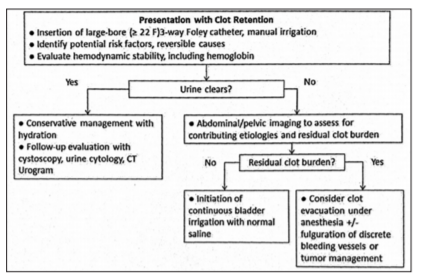
When our patient presented to the emergency department with gross hematuria, the team followed AUA guidelines with placement of a 3-way catheter and manual irrigation. This algorithm is outlined in Figure 1. By the time urology was consulted, he was hemodynamically stable with clear urine. The patient continued to bleed and required manual and continuous bladder irrigation, prompting a trip to the operating room for a cystoscopy with clot evacuation and fulguration to stop any active bleeding.
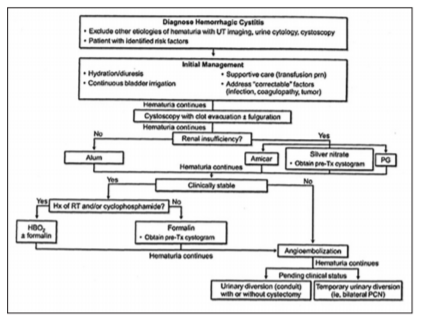
There is a strong correlation between bleeding due to hemorrhagic cystitis and previous history of radiation therapy. Our patient had a history of prostate cancer that was treated with external beam radiation in 2007. Radiation-induced damage to the bladder is typically a delayed process, with patients presenting at a median of 35 months after radiation treatment [1] When a patient fails conservative measures, management options including intravesical instillations are the next course of treatment. Figure 2 shows the algorithm proposed in Campbell-Walsh Urology consistent with the course of action and decisions made in the above case.
Our patient failed continuous bladder irrigation as well as cystoscopy with clot evacuation and fulguration. He was a candidate for alum instillation based on renal function. Alum is an initial management measure in a patient with hemorrhagic cystitis that does not resolve with continuous bladder irrigation. It causes protein precipitation on the urothelial lining, vasoconstriction, and decreased capillary permeability [6]. Amicar was also attempted with failure of symptom improvement.
Although it is further down in the algorithm, intravesical formalin continues to be an option through which hemostasis is achieved. Formalin, both historically and presently, has been successful in treating patients who have failed previous attempts at treatment. One study, from 1976, states that formalin treatment was effective in 14 of 16 patients in the present series and 79 of 90 cases reported in the literature [7]. In another review following 25 patients, 15 of which the patients had episodes of refractory bleeding due to history of pelvic radiation, 88% of patients achieved proper hemostasis after 4 months of follow-up. 10 patients had prior surgical intervention involving prior supravesical diversion, as in our patient [8].
In addition, even more recently, formalin continues to be a viable option in patients with refractory hematuria. Formalin is reserved for clinically stable patients who have failed initial management, cystoscopy with fulguration, and various instillations depending on renal function status. In a cohort study that followed eight patients managed with formalin for hemorrhagic cystitis from 2000 to 2014, they concluded that formalin remains an important tool for treating refractory hemorrhagic cystitis, with roughly 75.0% of patients requiring no additional therapy before hospital discharge [4].
CONCLUSION
Hemorrhagic cystitis can be a manifestation of previous exposure to pelvic radiation and can be treated with several methods. Intravesical instillations are an option once a patient has failed initial management. Formalin, while not the first- line treatment, can be one such route resulting in successful hemostasis in patients with hemorrhagic cystitis.
REFERENCES
- Linder BJ, Boorjian SA. Management of Emergency Bleeding, Recalcitrant Clots, and Hemorrhagic Cystitis. AUA Update Series. Maryland: American Urological Association Education and Research, Inc.; 2015. p. 34.
- Horan N, Cooper JS. Hyperbaric, Radiation Cystitis. In: Stat Pearls Treasure Island (FL): Stat Pearls Publishing; 2018. Available from: https://www.ncbi.nlm.nih.gov/books/ NBK470594. [Last accessed on 2017 Nov 27].
- Brian L, Linder BJ, Tarrell RF, Boorjian SA. Mp20-20 cystectomy for refractory hemorrhagic cystitis: Contemporary etiology, presentation and outcomes. J Urol 2015;193:2153.
- Ziegelmann MJ, Boorjian SA, Joyce DD, Montgomery BD, Linder BJ. Intravesical formalin for hemorrhagic cystitis: A contemporary cohort. Can Urol Assoc J 2017;11:E79-82.
- Donahue LA, Frank IN. Intravesical formalin for hemorrhagic cystitis: Analysis of therapy. J Urol 1989;141:809-12.
- Meredith FC, Wein AJ, Kavoussi LR. Campbell-Walsh Urology. 11th ed. Philadelphia, PA: Saunders Elsevier; 2016.
- Stanley HS, Donaldson MH, Duckett JW, Wein AJ. Formalin treatment for intractable hemorrhagic cystitis. A review of the literature with 16 additional cases. Cancer 1976;38:1785-9.
- Vicente J, Rios G, Caffaratti J. Intravesical formalin for the treatment of massive hemorrhagic cystitis: Retrospective review of 25 cases. Eur Urol 1990;18:204-6.