Effect of Low-Dose Amitriptyline Treatment for Interstitial Cystitis/Bladder Pain Syndrome
Weiguo Chen1, Donghua Xie2, Guolu Liu1, Yifan Chen1, Zongqiang Cai1
2.Xie Urology LLC., Margate, FL 33063,Florida.
Citation : Chen W, Xie D, Liu G, Chen Y, Cai Z. Effect of Low-Dose Amitriptyline Treatment For Interstitial Cystitis/Bladder Pain Syndrome. Clin Res Urol 2018;1(1):1-5.
The primary purpose of this study is to evaluate the efficacy and safety of low-dose amitriptyline therapy on symptoms in patients with interstitial cystitis/bladder pain syndrome (IC/BPS).
Between September 2015 and December 2016, 102 patients with IC/BPS received low-dose amitriptyline therapy (25 mg/d, before bedtime) at a 12-week course. The outcome measures used were IC symptom index and IC problem index (ICSI/ICPI), 24-h frequency- volume chart, and visual analog scale (VAS), which were completed before and 4 and 12 weeks after amitriptyline treatment.
A total of 89 patients (mean age of 61.9 years) with IC/BPS were recruited in this low-dose amitriptyline therapy study. The response rate was 66.3% (89 patients). Compared with baseline, the various IC symptoms improved significantly. Comparing values before treatment and 4 and 12 weeks after treatment (baseline vs. 4 weeks-baseline vs. 12 weeks), the rates of improvement were as follows: ICSI - 38.42%-49.61%, ICPI - 45.04%-53.20%, 24-h frequency - 45.54%-50.83%, VAS - 41.18%-70.01%, and function bladder volume - +139 ml-+122 ml, which showed statistically significant differences (P < 0.05). However, comparing values at 4 and 12 weeks after treatment (4 weeks vs. 12 weeks), only VAS and urgency showed a statistically significant decrease (P < 0.05). Side effects occurred in 72 patients (80.90%), primarily including mouth dryness (66.30%) and drowsiness (49.44%).
Low-dose amitriptyline therapy is a feasible, effective, and safe treatment for the subgroup of patients with IC/BPS in a short term.
Amitriptyline, bladder pain syndrome, interstitial cystitis, low urinary tract symptom, treatment
Lower-dose amitriptyline therapy in IC/BPS showed a clear decrease in low urinary tract symptoms and pelvic pains for 12 weeks after treatment with tolerable side effects.
INTRODUCTION
The prevalence of interstitial cystitis/bladder pain syndrome (IC/BPS) varies greatly by nation, race, and diagnostic criteria, with an overall global prevalence of 0.1-2%, but women are more commonly affected than men by a ratio of 5:1 [1,2]. IC/BPS is still a disease of unknown etiology, characterized by pain and discomfort in the bladder area or lower pelvis that is frequently or typically relieved by voiding, along with lower urinary tract symptoms, for example, urgency or frequency of urination in the absence of urinary tract infections [3]. There is no curative treatment currently, so the treatment principle in the management of IC/BPS is to relieve symptoms and improve life quality [4]. The tricyclic antidepressant amitriptyline is the classic therapy for IC/BPS and has a demonstrated efficacy of 50-60%, with greater efficacy rates (up to 77%) at sustained higher doses (at least 50 mg daily) [5]. We now report the efficacy and safety of low-dose amitriptyline (25 mg) administration on symptoms in patients with IC/BPS.
PATIENTS AND METHODS
Between September 2015 and December 2016, 102 patients were diagnosed with IC/BPS. All patients met the criteria of the AUA guideline for IC/BPS through the O'Leary-Sant Symptom Index and cystoscopy under general anesthesia at only one institute (First Affiliated Hospital of Soochow University) [6]. They were recruited into an open-label study, which was approved by the Board of Ethics because of its minimal risk and non-invasiveness. All IC/BPS patients were treated with low-dose amitriptyline (25 mg, PO. before bedtime) for 12 weeks. Previous or current intake of nonsteroidal antiinflammatory drugs (NSAIDs), amitriptyline, gabapentin, and anticholinergic agents was considered an exclusion criterion for study enrollment.
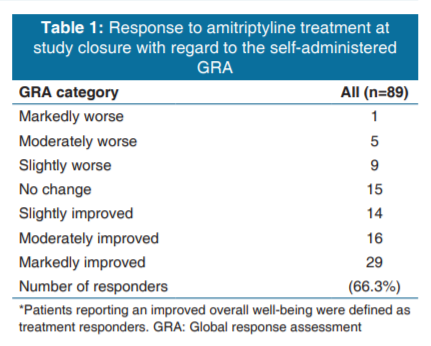
A patient-reported global response assessment (GRA) was used at study closure relative to overall baseline symptoms before amitriptyline therapy to identify treatment responders. The GRA is a 7-point centered scale rating the overall well-being. The 7 points included markedly worse, moderately worse, slightly worse, no change, slightly improved, moderately improved, and markedly improved. Patients who reported any of the last 3 categories were defined as treatment responders. Further efficacy measures included patient-reported symptoms of pain and urgency (100 mm visual analog scale [VAS]) and changes in functional bladder capacity and frequency (24-h frequency- volume chart, 3 days). An additional outcome measure was a change from baseline in the O'Leary-Sant IC symptom index (ICSI) and problem index (ICPI). All these treatment- based changes in IC/BPS-related symptoms were evaluated before treatment and 4 and 12 weeks after amitriptyline therapy.
Different statistical methods including Wilcoxon signed- rank test and Kruskal-Wallis test were used (SPSS ver. 13.0, SPSS Inc., Chicago, IL, USA) for analyses of the outcome. P ≤ 0.05 was considered statistically significant.
RESULTS
The data of 89 patients were available for evaluation 12 weeks after amitriptyline treatment. Thirteen patients were excluded from this study due to increasing amitriptyline dosage (over 25 mg/d) needed to relieve symptoms (10 cases) or withdrawal from this study because of fear of drug adverse effects (3 cases). The included patients consisted of 8 men and 81 women. Their age ranges from 25 to 83 years, and the mean age is 61.9 years. All patients experienced IC/BPS- related symptoms with a mean duration of 51.8 months before they visited the Urology Clinic at the First Affiliated Hospital of Soochow University. Overall response to amitriptyline treatment at a low dose (25 mg) was observed in 66.3% of patients [n = 59, Table 1].
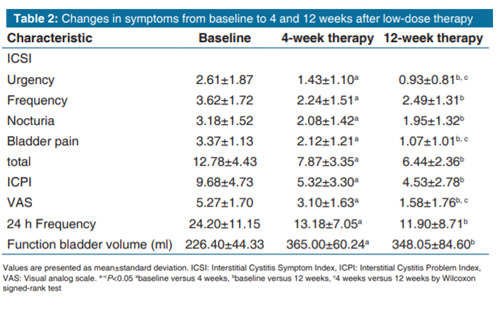
The ICSI, ICPI, 24-h frequency, and VAS conducted before treatment showed high scores of 12.78, 9.68, 24.20, and 5.27, respectively [Table 2]. Comparing values before treatment and 4 and 12 weeks after treatment (baseline vs. 4 weeks and baseline vs. 12 weeks), the rates of improvement were as follows: ICSI - 38.42%-49.61%, ICPI - 45.04%-53.20%; 24-h frequency - 45.54%-50.83%, VAS - 41.18%-70.01%, and function bladder volume - +138.6 ml-+121.65 ml, with all parameters which showed statistically significant differences (P < 0.05). However, comparing values at 4 and 12 weeks after treatment (4 weeks vs. 12 weeks), only the scores of VAS showed a statistically significant decrease (P < 0.05). The ICSI, ICPI, 24-frequency, and function bladder volume did not show statistically significant difference (P > 0.05) [Table 2].
Scores of urgency, urgency incontinence, frequency, nocturia, and bladder pain, which are components of the ICSI, were compared before and after treatment. As for the ICSI, a comparison of the results before treatment and 4 and 12 weeks after treatment revealed a statistically significant improvement in urgency, urgency incontinence, frequency, nocturia, and bladder pain (P < 0.05). When results at 4 and 12 weeks after treatment were compared, only scores of urgency and bladder pain showed a statistically significant improvement [Table 2].
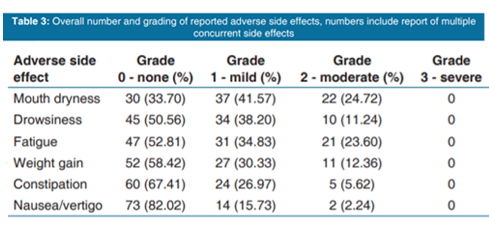
The majority of the patients (72 of 89 or 80.90%) showed at least one side effect but in mild or moderate manner. Mouth dryness was the most frequent side effect reported in the amitriptyline group (66.30%). No adverse side effects of grade 3 or higher were reported. There were no adverse events severe enough to stop the treatment [Table 3].
DISCUSSION
It has been three decades since the first study of treating IC patients with the tricyclic antidepressant amitriptyline was reported[7]. So far, amitriptyline has become the most frequently prescribed oral drug for IC within the patient population of the IC database [8,9]. Current guidelines also recommend oral amitriptyline as a second-line treatment option that may provide benefit in a subset of patients [10]. Amitriptyline acts through the blockade of acetylcholine receptors, inhibition of reuptake of released serotonin and norepinephrine, and blockade of histamine H1 receptors [11]. Several studies have documented the beneficial effects of amitriptyline in the treatment of IC/BPS. A double-blind, placebo-controlled study showed that, in the subset of patients achieving a dose of at least 50 mg daily, a significantly higher response rate was observed in the amitriptyline group (66% vs. 47% with placebo; P = 0.01) [12]. van Ophoven et al. reported that amitriptyline therapy for 4 months was safe and effective for treating IC, and they conducted a prospective placebo-controlled study and found that amitriptyline significantly improved the mean symptom score, pain and urgency intensity, whereas frequency and functional bladder capacity improved but not significantly [13]. In our study, amitriptyline demonstrated the overall response rate of 66.3% at a low dose (25 mg/d) in the management of IC/BPS, which was higher compared to other studies at such a low dosage; perhaps, it was due to vesical dilatation during cystoscopic examination under general anesthesia, which we performed for all the studied patients before their intake of amitriptyline.
IC/BPS is a syndrome consisting of severe refractory bladder symptoms, i.e., pain, urgency, and frequency in the absence of a specific underlying identifiable cause [3,14,15]. It is well-known that normal bladder can store a sufficient amount of urine followed by a painless urge to void and finally almost complete emptying. This complex ability, which is severely impaired in patients with IC, is based on activation and maintenance of sophisticated reflex mechanism involving sympathetic, parasympathetic, and somatic control of the lower urinary tract [16]. The spinal and supraspinal neuronal pathways involved are modulated by activation and/or inhibition of neurons in the periphery, at spinal levels, and at supraspinal regulatory sites. Serotonergic (5-hydroxytryptamine [5-HT]) pathways and receptor mechanisms have a crucial role within this neuronal network [17]. The mechanism of action of serotonergic drugs, such as the well-known 5-HT reuptake inhibitor amitriptyline, is to modulate this neuronal network, resulting in an ameliorating impact on the impaired bladder function of patients with IC/BPS [18]. The mechanism of analgesic action of amitriptyline in general and, particularly, for IC is not fully understood [19,20]. Collectively, current data from functional studies and clinical observations indicate that 5-HT receptor activation induced by amitriptyline appears to act as a pharmacological neuromodulation of afferent and efferent neuronal pathways that signal and regulate pain and urgency sensations from the bladder [9]. According to our findings, significant improvements in urgency intensity, functional bladder capacity, daytime frequency, and nocturia were noted after 4-week treatment at a daily dose of 25 mg amitriptyline, and the therapeutic efficacy maintained until 12 week after the end of the treatment. A number of other studies have also documented the beneficial effects of amitriptyline in daytime frequency, urgency, dyspareunia, and other bladder storage dysfunction syndromes [12,21]. However, we did not observe significant improvement in the GRA response rate in subjects who maintained higher doses (over 25 mg daily, data not shown).
Although there are some reports on the usefulness of gabapentin, amitriptyline, and NSAIDs, there are limitations to use a single drug to control and treat a patient's pain effectively [22]. Tricyclic antidepressants are used to treat various pain syndromes and cause effects such as increased pain tolerance, recovery of normal sleep, and decrease in depression symptoms [20] They can be effective against chronic pain by directly suppressing the nervous mechanisms underlying pain or by alleviating depression symptoms caused by the inability to accept pain or experience pain. They control the activation and suppression of peripheral neurons or modulate the neuronal inhibitory or stimulatory pathways in the spine or supraspinal segments. Such mechanisms alleviate pain symptoms by suppressing acetylcholine, histamine, and the H1 receptor and by inhibiting the reuptake of released serotonin and norepinephrine [23]. In our study, when values before treatment and 4 and 12 weeks after treatment were compared, those of the ICSI, ICPI, frequency, and VAS showed statistically significant improvement. However, when values at 4 and 12 weeks after low-dose therapy were compared, only VAS score showed significant improvement after the longer duration of therapy.
Reduction in the ICSI and ICPI score was significantly greater in the low-dose amitriptyline treatment, with mouth dryness (66.30%) being the most frequent side effect in our study. As the side effects were primarily mild to moderate, all patients were able to achieve and maintain a dose of at 25 mg per day through the whole amitriptyline treatment period. Antidepressant side effects, such as drowsiness (49.44%) and fatigue (47.19%), were also bearable.
In conclusion, low-dose amitriptyline therapy in IC/BPS showed a clear decrease in bladder pain and bladder storage symptoms after 4 weeks and 12 weeks after treatment, with additional benefit seen on pain management for the treatment of 12 weeks. The side effects were well tolerated.
REFERENCES
- Davis NF, Gnanappiragasam S, Thornhill JA. Interstitial cystitis/painful bladder syndrome: The influence of modern diagnostic criteria on epidemiology and on internet search activity by the public. Transl Androl Urol 2015;4:506-11.
- Offiah I, Didangelos A, Dawes J, Cartwright R, Khullar V, Bradbury EJ, et al. The expression of inflammatory mediators in bladder pain syndrome. Eur Urol 2016;70:283-90.
- Jhang JF, Kuo HC. Pathomechanism of interstitial cystitis/ bladder pain syndrome and mapping the heterogeneity of disease. Int Neurourol J 2016;20:S95-104.
- Wang J, Wang Q, Wu Q, Chen Y, Wu P. Intravesical botulinum toxin a injections for bladder pain syndrome/interstitial cystitis: A systematic review and meta-analysis of controlled studies. Med Sci Monit 2016;22:3257-67.
- Generali JA, Cada DJ. Amitriptyline: Interstitial cystitis (painful bladder syndrome). Hosp Pharm 2014;49:809-10.
- Hanno PM, Erickson D, Moldwin R, Faraday MM, American Urological Association. Diagnosis and treatment of interstitial cystitis/bladder pain syndrome: AUA guideline amendment. J Urol 2015;193:1545-53.
- Hanno PM, Wein AJ. Medical treatment of interstitial cystitis (other than rimso-50/elmiron). Urology 1987;29:22-6.
- Riedl C, Engelhardt P, Schwarz B. Treatment costs of bladder pain syndrome/interstitial cystitis in Austria: A pharmacoeconomic approach following current guidelines. Clin Drug Investig 2013;33:737-42.
- van Ophoven A, Pokupic S, Heinecke A, Hertle L. A prospective, randomized, placebo controlled, double-blind study of amitriptyline for the treatment of interstitial cystitis. J Urol 2004;172:533-6.
- Hanno PM, Burks DA, Clemens JQ, Dmochowski RR, Erickson D, Fitzgerald MP, et al. AUA guideline for the diagnosis and treatment of interstitial cystitis/bladder pain syndrome. J Urol 2011;185:2162-70.
- Fall M, Oberpenning F, Peeker R. Treatment of bladder pain syndrome/interstitial cystitis 2008: Can we make evidence- based decisions? Eur Urol 2008;54:65-75.
- Foster HE Jr., Hanno PM, Nickel JC, Payne CK, Mayer RD, Burks DA, et al. Effect of amitriptyline on symptoms in treatment naive patients with interstitial cystitis/painful bladder syndrome. J Urol 2010;183:1853-8.
- Sun Y, Fang Z, Ding Q, Zheng J. Effect of amitriptyline in treatment interstitial cystitis or bladder pain syndrome according to two criteria: Does ESSIC criteria change the response rate? Neurourol Urodyn 2014;33:341-4.
- Kim HJ. Update on the pathology and diagnosis of interstitial cystitis/bladder pain syndrome: A review. Int Neurourol J 2016;20:13-7.
- Pang R, Ali A. The Chinese approach to complementary and alternative medicine treatment for interstitial cystitis/bladder pain syndrome. Transl Androl Urol 2015;4:653-61.
- Patnaik SS, Lagana AS, Vitale SG, Buttice S, Noventa M, Gizzo S, et al. Etiology, pathophysiology and biomarkers of interstitial cystitis/painful bladder syndrome. Arch Gynecol Obstet 2017;295:1341-59.
- Sanford MT, Rodriguez LV. The role of environmental stress on lower urinary tract symptoms. Curr Opin Urol 2017;27:268-73.
- Zhu HJ, Appel DI, Grundemann D, Richelson E, Markowitz JS. Evaluation of organic cation transporter 3 (SLC22A3) inhibition as a potential mechanism of antidepressant action. Pharmacol Res 2012;65:491-6.
- Kremer M, Salvat E, Muller A, Yalcin I, Barrot M. Antidepressants and gabapentinoids in neuropathic pain: Mechanistic insights. Neuroscience 2016;338:183-206.
- Papandreou C, Skapinakis P, Giannakis D, Sofikitis N, Mavreas V. Antidepressant drugs for chronic urological pelvic pain: An evidence-based review. Adv Urol 2009;2009:797031.
- Yang W, Propert KJ, Landis JR. Estimating the efficacy of an interstitial cystitis/painful bladder syndrome medication in a randomized trial with both non-adherence and loss to follow-up. Stat Med 2014;33:3547-55.
- Lee JW, Han DY, Jeong HJ. Bladder pain syndrome treated with triple therapy with gabapentin, amitriptyline, and a non-steroidal anti-inflammatory drug. Int Neurourol J 2010;14:256-60.
- Sawynok J, Esser MJ, Reid AR. Antidepressants as analgesics: An overview of central and peripheral mechanisms of action. J Psychiatry Neurosci 2001;26:21-9.