Audit of the Outcomes and Intraoperative Complications in the Single Incision and Retropubic Slings for Treating Stress Urinary Incontinence
Tristan Symonds, Sapna Dilgir, Ajay Rane, Venkat Vengaveti
Citation : Symonds T, Dilgir S, Rane A, Vengaveti V. Audit of the Outcomes and Intraoperative Complications in the Single Incision and Retropubic Slings for Treating Stress Urinary Incontinence. Clinic Res Urol 2018;1(2):1-4.
Stress urinary incontinence (SUI) is a common condition affecting woman. The Supris retropubic sling and Altis single-incision sling are two products used in surgical management of SUI. The Altis sling has been removed from the market by the Therapeutic Goods Administration as of 4/1/18. The aim of this audit was to compare the efficacy of a single-incision sling to traditional retropubic sling.
A retrospect audit was conducted at one site with a unit consisting of two surgeons. A total of 136 files were reviewed and included all patients who underwent suburethral sling surgery in 2017. Data were collected on baseline demographics, perioperative complications, and the objective and subjective outcomes.
Of the 136 patients who were treated for stress urinary incontinence (SUI), 104 (76.5%) underwent an Altis procedure and 32 (23.5%) underwent a Supris procedure. The intraoperative complication rate was 2% with the Altis and 12.5% with the Supris. Patients had a successful outcome 90.4% of the time with the Altis and 89.3% of the time with the Supris. The patients subjective outcome reported =7/10 or above on a Likert questionnaire 84.1% in the Altis group and 82.4% in the Supris group.
The data in this paper do not reach statistical significance in comparing the two slings. It does suggest that the Altis single-incision mini-sling has a low number of perioperative complications and the objective and subjective outcomes of the Altis and Supris sling are comparable in treating stress urinary incontinence.
Mini-sling, mid-urethral sling, single-incision mini-sling, standard mid-urethral slings, stress urinary incontinence.
BACKGROUND
Urinary incontinence has been shown to affect up to 10-40% of women [1,2]. Studies have shown that up to 80% of these women are affected by SUI [3]. SUI is the complaint of involuntary leakage of urine on effort or exertion, or on sneezing or coughing. The current treatment options for SUI include conservative therapies such as continence pessaries and physiotherapy. More invasive options include surgery. The most common and effective of the surgical options is a suburethral pubic sling composed of mesh.
Due to reports of complications after surgery for pelvic organ prolapse (POP), the Food and Drug Administration has changed the classification of surgical mesh for POP repairs from a moderate-risk device to a high-risk device. Only more recently the Therapeutic Goods Administration (TGA) in Australia proposed to remove the transvaginal mesh for pelvic prolapse and single-incision mini-slings from the Australian Register of Therapeutic Goods, deeming the devices too risky, with the changes taking effect from January 4, 2018. Research has shown that surgical mesh for transvaginal repair of POP can cause complications such as mesh erosion, pain, infection, bleeding, dyspareunia, and urinary problems. Treating SUI with mesh can also cause complications including mesh erosion, infection, and pain. However, complications are usually less severe; the erosion rate is 1-2% for SUI versus 11% with mesh for POP. Mesh complications associated with SUI rarely require repeat surgery [4].
The current public's concern with mesh has led to pharmaceutical companies removing surgical mesh for the treatment of SUI from the market. There are current concerns among urogynecologists that this will lead to a shortage of surgical treatment options in the future for women suffering from SUI. This is already resulting in some surgeons pursuing older procedures which are more complicated and less effective such as the Burch colposuspension.
Surgical treatment of SUI has changed considerably over the recent decades. Umsten et al. presented his minimally invasive midurethral sling (MUS) procedure under local anesthetic in 1996 [5]. In a MUS operation, a synthetic mesh or sling is placed underneath the urethra. When the women coughs or strains, the mesh compresses the urethra, thus providing the support necessary to prevent a leak.
Since the introduction of the standard MUS (SMUS), this method has been modified through the introduction of the transobturator approach. The objective of this approach was to eliminate the risk of damage to bladder by passing "blind" through the retropubic route [6]. However, several studies have shown that the transobturator procedure is associated with post-operative groin pain and increased bleeding [6].
The single-incision mini-sling (SIMS) was assumed to solve some of these complications. By inserting into the obturator membrane, it avoided passing through the retropubic region and the groin adductor muscles. A Cochrane database systematic review found that there was not enough evidence on other SIMS compared to retropubic and transobturator slings to allow reliable comparison. The study concluded that SIMS may be more cost-effective than SMUS based on 1-year follow-up; however, trials with longer term follow-up were required [7]. Despite the benefits of shorter operation time, less blood loss and fewer complications some studies concluded that there was a significantly higher 3-year failure rate for SIMS versus SMUS [8,9]. However, more recent data have demonstrated that they may be equally as effective.
The Altis SIMS and Supris SMUS are a new third-generation synthetic mesh used in the surgical treatment of SUI. The Supris is a "retropubic" sling which means it is inserted behind the pubic bone. The Altis is a SIMS and is anchored into the obturator membrane.
Although TGA has removed the Altis SIMS from the Australian market, as of January 4, 2018, the sling is available elsewhere in the world. The aim of the audit is to publish data around the efficacy of these two types of MUS (single incision and retropubic). The audit was carried out by retrospectively reviewing patient's charts from the private practice of an urogynecologist.
METHODS
A retrospective audit was conducted at the Mater Hospital Pimlico in North Queensland, Australia. The units consist of a trainee and an advanced pelvic floor fellow. All procedures were performed by the urogynecologists or under direct supervision. Patients in the audit included those who were operated on between January 1st 2017 and December 31st 2017. A total of 136 files were reviewed. Data were collected on baseline demographics, perioperative complications, and objective and subjective outcomes. A positive stress leak at urodynamics was objective treatment failure and a Likert questionnaire on satisfaction was used as a subjective measure.
RESULTS
The audit included 136 cases. There were a total of 104 (76.5%) Altis single-incision slings performed and 32 (23.5%) Supris midurethral slings. This was predominantly because at this unit, SIMS was used as the first-line treatment when maximal urethral closing pressure was >10 cm H(2)O. Of the 32 Supris slings, 7 (21.8%) were performed after a previously failed Altis sling. The median age of the women was 68.5, the youngest was 36, and the oldest was 91. All patients underwent urodynamic studies to confirm SUI.
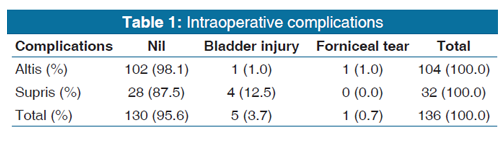
The breakdown of intraoperative complications can be viewed in Table 1. There were two intraoperative complications with the use of the Altis (2%) and four with the Supris sling (12.5%). Cystotomy occurred in 1% of the operations involving the Altis sling and in 12.5% of the operations involving the Supris sling. All patients were discharged on the same day and there were no sequelae as a result of the perforations.
The outcomes of post-operative trial of void can be viewed in Table 2. Data were collected on 119 of the 136 procedures. Patients with an initial failed trial of void were assessed as failed and continued with a trial of void protocol.
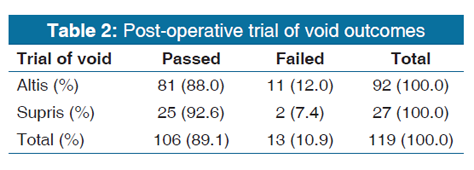
Patients who underwent an Altis procedure failed an initial trial of void 12% of the time compared to patients who underwent a Supris procedure that failed an initial trial of void 7.4% of the time. There was no statistical significance between the two groups (P = 0.73). Of these patients that failed a post-operative void six were admitted overnight with urinary retention this included: Five Altis and one Supris patient. One patient developed urinary retention and required discharge with a catheter from the Altis group.
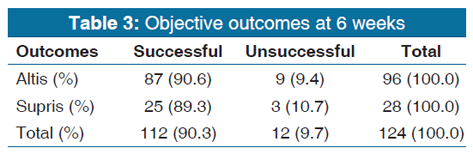
The objective outcomes of the slings can be viewed in Table 3. These were assessed through a positive or negative cough test with patients who were followed up at urodynamics postoperatively at the 6-week mark. For the Altis sling, 9.4% of patients still experienced a positive cough test at the 6-week mark compared to 10.7% for the Supris sling. There was no statistical significance between the groups.
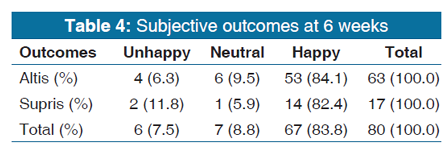
The subjective outcomes of patients at 6 weeks postoperatively can be viewed in Table 4. Patients filled out a Likert scale between 1 and 10 to indicate their level of satisfaction with the improvement in their urinary stress incontinence. For simplification patients who rated [1-3] were unhappy,[4-6] were neutral, and [7-10] were happy with the outcome. 80 patients had filled out a questionnaire. Patients in the Altis group reported being happy 84.1%, neutral 9.5%, and unhappy 6.3% of the time. Patients who underwent a Supris procedure reported being happy 82.4%, neutral 5.9%, and unhappy 11.8% of the time.
DISCUSSION
Treating SUI through SMUS or SIMS gives majority of patients a good outcome and high level of satisfaction. Severe complications are rare although the number of cases reviewed is low.
The most common intraoperative complication in retropubic slings is bladder injury. The reported complication rate ranges between 3.5% and 6.6% [10-14]. In this audit, the number of bladder injuries was higher at 12.5%. None of these were complete perforations of the bladder wall and all women were discharged same day without sequelae. There are two potential explanations for the higher rate of bladder injuries in this audit. The first is that the number of Supris procedures was quite low, and therefore, every complication has the potential to dramatically increase the perceived rate of injury. However, it is known that retropubic slings will result in increased rate of cystotomy due to the trocar placed adjacent to the bladder. Second, all four of the bladder injuries occurred by the advanced trainee highlighting the more difficult learning curve and higher potential for injury with passing through a "blind" route with the retropubic sling. This suggests that SIMS may be an easier technique to teach trainees.
Post-operative voiding dysfunction was seen in a total of 10.9% of the patients. There was a higher percentage in the Altis group (12.0%) compared to the Supris group (7.4%); however, there was no statistical significance between the groups (P = 0.703). One patient (0.96%) from the Altis group was discharged with a catheter and was voiding normally at 6 weeks. The reported rates of voiding dysfunction vary from 19.7% to 47% of cases, depending on the definition and diagnostic criteria used [12,13]. In our practice, incomplete bladder emptying was defined as failed trial of void. We did not look at other factors that may have contributed to voiding dysfunction, such as pain. No patients required a sling release and all were voiding normal at 6 weeks.
The two outcomes assessed: Objective and subjective are comparable between the Altis and the Supris groups. Objectively, there was a success rate of 90.6% for patients having an Altis and 89.3% for patients having a Supris. Of the 32 patients undergoing a Supris procedure, seven patients had failed a previous SIMS treatment for SUI. The failure rates for those SIMS ranged from 3 months to 6 years. All seven of these patients had negative cough tests at urodynamics at the 6-week mark. The subjective outcome was similar between the two groups 84.1% for Altis and 82.4% for Supris rated a ≥ 7/10 in a Likert scale on a questionnaire at their follow-up.
These results are similar to a 2014 systematic review and meta-analysis by Mostafa et al. who assessed SIMS versus SMUS in the surgical management of SUI [15]. Their meta-analysis found no RCTs evaluating the Altis sling at the time of publication but grouped its efficacy and safety with other SIMS such as the Ajust and TFS. Their analysis concluded that there was no evidence of significant difference in subjective or objective cure between SIMS and SMUS.
Some limitations should be noted in this audit. First, the number of cases across both the Altis and the Supris slings is low. This makes trends difficult to identify and none of the comparison data was statistically significant. The reason the Supris sling numbers are low is because at this unit it is used as a second-line treatment. This is evident by the fact that 7 of the 32 women (21.8%) undergoing a Supris procedure had a previously failed Altis procedure.
Our study suggests that SIMS may be as effective as retropubic slings with lower complications. In addition, it may be easier to teach trainees.
REFERENCES
- Hunskaar S, Burgio K, Diokno A, Herzog AR, Hjalmas K, Lapitan MC, et al. Epidemiology and natural history of urinary incontinence in women. Urology 2003;62:16-23.
- Milsom I AD, Lapitan MC, Nelson R, Sillen U. Epidemiology of Urinary (UI) and Faecal (FI) Incontinence, Pelvic Organ Prolapse (POP). Incontinence: 4 International Consultation on Incontinence; 2009.
- Hampel C, Wienhold D, Benken N, Eggersmann C, Thuroff JW. Definition of overactive bladder and epidemiology of urinary incontinence. Urology 1997;50:4-14.
- Shah HN, Badlani GH. Mesh complications in female pelvic floor reconstructive surgery and their management: A systematic review. Indian J Urol 2012;28:129-53.
- Ulmsten U, Henriksson L, Johnson P, Varhos G. An ambulatory surgical procedure under local anesthesia for treatment of female urinary incontinence. Int Urogynecol J Pelvic Floor Dysfunct 1996;7:81-5.
- Ford AA, Rogerson L, Cody JD, Aluko P, Ogah JA. Mid-urethral sling operations for stress urinary incontinence in women. Cochrane Database Syst Rev 2017;7:CD006375.
- Nambiar A, Cody JD, Jeffery ST, Aluko P. Single-incision sling operations for urinary incontinence in women. Cochrane Database Syst Rev 2017;7:CD008709.
- Basu M, Duckett J. Three-year results from a randomised trial of a retropubic mid-urethral sling versus the miniarc single incision sling for stress urinary incontinence. Int Urogynecol J 2013;24:2059-64.
- Rudnicki M, von Bothmer-Ostling K, Holstad A, Magnusson C, Majida M, Merkel C, et al. Adjustable mini-sling compared with conventional mid-urethral slings in women with urinary incontinence. A randomized controlled trial. Acta Obstet Gynecol Scand 2017;96:1347-56.
- Jha S, Hillard T, Monga A, Duckett J. National BSUG audit of stress urinary incontinence surgery in England. Int Urogynecol J 2018. Doi: 10.1007/s00192-018-3705-4.
- Gold RS, Groutz A, Pauzner D, Lessing J, Gordon D. Bladder perforation during tension-free vaginal tape surgery: Does it matter? J Reprod Med 2007;52:616-8.
- Kristensen I, Eldoma M, Williamson T, Wood S, Mainprize T, Ross S. Complication of the tension-free vaginal tape procedure for stress urinary incontinence. Int Urogynecology J 2010;21:1353-7.
- Abouassaly R, Steinberg JR, Lemieux M, Marois C, Gilchrist LI, Bourque JL, et al. Complications of tension-free vaginal tape surgery: A multi-institutional review. BJU Int 2004;94:110-3.
- Dyrkorn OA, Kulseng-Hanssen S, Sandvik L. TVT compared with TVT-O and TOT: Results from the Norwegian national incontinence registry. Int Urogynecol J 2010;21:1321-6.
- Mostafa A, Lim CP, Hopper L, Madhuvrata P, Abdel-Fattah M. Single-incision mini-slings versus standard midurethral slings in surgical management of female stress urinary incontinence: An updated systematic review and meta-analysis of effectiveness and complications. Eur Urol 2014;65:402-27.