Mondor Disease - An Underdiagnosed Pathology: Case Report and Review of Literature
Maria A. Ocampo1, Julian Chavarriaga2, Nayib Fakih2, Jose Miguel Silva3
2.Department of Urology, Pontificia Universidad Javeriana, Bogota, Colombia.
3.Department of Urology, Hospital Universitario San Ignacio, Assistant Professor Pontificia Universidad Javeriana, Bogota, Colombia.
Citation : Ocampo MA, Chavarriaga J, Fakih N, Silva, JM. Mondor Disease - An Undiagnosed Pathology: Case Report and Review of Literature. Clinic Res Urol 2019;2(1):1-3.
Mondor penile disease is the thrombophlebitis of the superficial dorsal penile vein. The incidence is 1.39% with a prevalence of 1.4%. The most common risk factor for this entity is mechanical trauma through sexual activity. Due to its low incidence, this entity is still unknown for many physicians including urologists. Our aim is to describe the case of a 22-year-old male with a clinical and ultrasonographic diagnosis of Mondor penile disease and review the initial evaluation, pathogenesis, risk factors, diagnosis, and treatment. A 22-year-old male, whose chief complaint was a 12-h duration of pain in the dorsal face of the penis after a robust sexual activity. At physical exam, it was evident the painful in the duration of the superficial dorsal penile vein pathway. A color Doppler ultrasound was performed with evidence of low venous flow and a hypoechogenic image in the superficial dorsal vein, confirming the diagnosis of Mondor disease. He received expectant treatment, with partial recanalization 6 weeks after the event, without any adverse effect on his sexual function. Mondor disease is an undiagnosed pathology due to the fear of the patient to consult, or the medical team is unaware of the condition. Is very important to be familiarized with this pathology, so an accurate diagnosis and treatment are provided, avoiding unnecessary procedures. Is important to give education to decrease the anxiety related to the diagnosis and avoid performance issues.
Mondor disease, Penile diseases, Penile induration, Penis, Thrombophlebitis, Thrombosis
INTRODUCTION
Mondor penile disease is a benign condition, characterized by thrombophlebitis of the superficial dorsal penile vein [1-3]. Its incidence is calculated in 1.39% and its prevalence around 1.4%, usually affecting sexually active men. The exact etiology of the disease is unknown, but there is a huge relationship with the mechanic trauma received during sexual intercourse [1,2]. This condition is usually undiagnosed due to fear or embarrassment; therefore, the patient does not seek medical help [2]. Our aim is to describe the case of a 22-year-old male diagnose with Mondor disease plus a review about the initial evaluation, pathogenesis, risk factors, diagnosis and treatment, so the urologist does not mislead the condition.
CASE REPORT
A 22-year-old male whose chief complaint was a 12-h duration of pain in the dorsal face of the penis, which starts 6 h after sexual intercourse; associated with heat and in duration in the base of the dorsal aspect of the penis. He has no medical history. Physical exam revealed a chordee-like painful lesion [Figures 1]. At palpation, the dorsal vein of the penis was indurated in the dorsal surface of the phallus and all the way through the balanopreputial sulcus. During this maneuver, an indurated plaque of 1 cm X 0.7 cm of diameter was identified at the base of the penis.

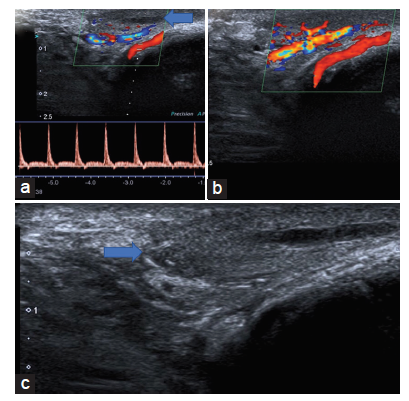
A penile Doppler ultrasound was performed with a transductor of 10 MHz. At the base of the dorsal surface, a hypoechogenic material, not compressible, and without blood flow was identified in the superficial dorsal vein [Figures 2]. These finding indicates the presence of a thrombus associated with an inflammatory reaction seen in the subcutaneous tissue. His blood count revealed leukocytosis as the only abnormal finding. The diagnosis of Mondor penile disease was made base on the physical examination findings and ultrasound results. Outpatient treatment was indicated with oral and topical nonsteroidal anti-inflammatory medication, topical corticosteroid, warm compresses, and abstinence from sexual activity for 6 weeks. 6 weeks later the patient had his medical control, with evidence of partial recanalization of the dorsal superficial vein of the penis; therefore, he was discharged from the urology service without complications.
DISCUSSION
Mondor penile disease is an uncommon benign medical condition, characterized by thrombophlebitis of the superficial dorsal penile vein [1-3]. The classic Mondor disease was first described as a superficial thrombosis of the thoracoepigastric veins in women during the year 1939 by Henri Mondor. In 1955 it was designated in the veins of the penis by Braun Falco and finally 3 years later was reported in the superficial dorsal vein of the penis by Helm and Hodge [3-5]. Mondor disease is often seen in men between 20 and 70 years old, with an incidence of 1.39% and a prevalence of 1.4% [1,2]. Its believed that many cases are undiagnosed because patients fear or are ashamed of their condition, thinking something bad happened to them, therefore, not seeking medical care [2,6]. On the other hand, physicians should get to know this entity so they can give an accurate diagnosis and provide the correct treatment. Ozkan et al. found in their study that 20% of their patients were misdiagnose when they looked for medical help in another institution [2]. The retroglandular plexus located behind the corona of the glans, rises small tributaries veins which finally drain in the superficial dorsal vein. This area is very susceptible to mechanical trauma during the sexual performance; therefore, an endothelial injury arises, leading to liberation of prothrombotic factors which will activate the coagulation cascade, ending in the formation of a thrombus; hence, the Virchow's triad has also been associated with the physiopathology of this entity. The superficial dorsal vein of the penis plays its role in the venous return of the subcutaneous tissue, buck's fascia, and the skin of the phallus. The pathway continues in the superficial external pudendal vein which finally carries the outflow to the long saphenous vein. Other etiologies can explain Mondor's disease such as surgical interventions in the inguinal canal leading to an abnormal pathway in the superficial external pudendal vein. Additional factors that can influence the outflow of the external pudendal vein is lower limb varices surgery and thrombosis of the saphenofemoral junction [2,3,6].
The most common risk factor for Mondors disease is prolonged or robust sexual activity [1-3,6]. As was the case of our patient, whose only risk factor was sexual activity, as well as being the most common trigger of Mondor disease. Other risk factors have been reported such as long periods of sexual abstinence, vein compression due to pelvic tumors or vesical distension, scar tissue from a circumcision, irritation secondary to menstrual blood, behcet syndrome, and infections such as sexually transmitted diseases, enteroviruses or tuberculosis, and two cases of extensive trips by plane or car have been reported in literature [2,3,7]. When none of these risk factors are present, the disease becomes idiopathic, and studies for coagulation deficiency factors such as Antithrombin III, protein C, and S should be made [6,7].
Mondor disease has three stages. The acute phase which starts 24-48 h after sexual intercourse, it is characterized by the induration and painful chordee-like appearance in the venous pathway in the dorsal surface of the phallus. In this phase, patients might also experience palpitations, continuous, or intermittent pain which is worsen with erections and may also have fever. The sub-acute phase presents itself 1 week after trauma, the intensity of this pain is less, and they can experience some irritative urinary symptoms. The last phase occurs 9 weeks later and is characterized by the recanalization of the vein, and normal outflow is reestablished [1-3].
The diagnosis of this disease is made by a complete medical history and an excellent physical examination. When the diagnosis is not well-defined, color Doppler ultrasound can help exclude the differential diagnoses and help build one. The findings in the ultrasound are absence or low venous return, the presence of a thrombus (hypoechogenic material) which leads to a not compressible vessel, low peak systolic velocity, and an increase resistant index in the cavernous artery [2,5,6,8].
This undiagnosed entity has two main differential diagnosis, sclerosis lymphangitis and Peyronie disease. Sclerosis lymphangitis is characterized by big and dilated lymphatic vessels which can be seen on color Doppler ultrasound with the preserved venous flow, whereas, Peyronie disease is portrayed by an abnormal curvature of the penis which is evident during a physical examination. Palpation reveals fibrotic plaques in the dorsal surface of the phallus and the ultrasound is with no evidence of thrombus[2,5,8].
Mondor disease is a self-resolving process; therefore, treatment should be expectant management, achieving restauration of blood flow within 6 weeks in >90% of the cases. During the first two stages of the disease, treatment should be sexual abstinence for 6 weeks, oral, and/or topical nonsteroidal anti-inflammatory drugs, heparin unguents or topical corticosteroids. Antibiotics should only be used when there is infection associated [1,2,5]. Our patient received expectant management, with a resolution of his symptoms by the 6th week. However, surgical management (thrombectomy or superficial dorsal vein removal) should be consider in patients with recurrence or refractory pathology, defined as the persistence of symptoms or absence of venous flow after 6 weeks of initial treatment [5,8]. Nowadays is important that patients are able to receive education about this disease sincethe anxiety the it can generate is huge and can affect their sexual performance, leading to erectile disfunction and decrease in the International Index of Erectile Function, thus, is very important to ensure is a benign, self-resolving condition [1,2,5].
CONCLUSION
Mondor disease is an undiagnosed entity, either patients do not seek for medical help or the physician is not familiarized with the disease. Throughout a complete medical history and a good physical exam, the diagnosis can be established, though, color Doppler ultrasound is a useful tool to confirm the diagnosis but not mandatory. Its crucial that the urologist is well informed about the disease to provide adequate treatment and instruct other doctors involved in the case, avoiding over treatments, and unnecessary tests. Finally, the physician should be able to educate the patient, emphasizing the benign and self-resolving course of the disease, avoiding the anxiety related to the diagnosis.
REFERENCES
- Kumar B, Narang T, Radotra BD, Gupta S. Mondor's disease of penis: A forgotten disease. Sex Transm Infect 2005;81:480-2.
- Ozkan B, Coskuner ER, Turk A, Akkus E, Yalcin V. Penile mondor disease and its effect on erectile function: Results of 30 patients. Urology 2015;85:113-7.
- Sasso F, Gulino G, Basar M, Carbone A, Torricelli P, Alcini E, et al. Penile mondors' disease: An underestimated pathology. Br J Urol 1996;77:729-32.
- Pittaka M, Fotiou E, Dionysiou M, Polyviou P, Eracleous E, Andreopoulos D, et al. Penile mondor's disease in a patient treated with radical chemoradiation for anal cancer. Oxf Med Case Reports 2017;2017:omx036.
- Haslam S, Ikpeama C, Wilkerson M. Penile mondor's disease: Two rare cases. Skin 2017;1:25-34.
- Conkbayir I, Yanik B, Keyik B, Hekimoglu B. Superficial dorsal penile vein thrombosis (mondor disease of the penis) involving the superficial external pudendal vein: Color doppler sonographic findings. J Ultrasound Med 2010;29:1243-5.
- Al-Mwalad M, Loertzer H, Wicht A, Fornara P. Subcutaneous penile vein thrombosis (Penile mondor's disease): Pathogenesis, diagnosis, and therapy. Urology 2006;67:586-8.
- Ozturk H. Penile mondor's disease. Basic Clin Androl 2014;24:5.