Spironolactone-Induced Rash: A Case Report and Review
Abdulhalim Jamal Kinsara
Citation : Kinsara AJ. Spironolactone - Induced Rash: A Case Report and Review. J Clin Cardiol Diagn 2018;1(2):1-2.
Spironolactone is a commonly used drug with good safety profile. However, side effects, although infrequent, still occur. We are reporting on a rather rare side effect and reviewing the literature.
Rash, Side effect, Spironolactone
INTRODUCTION
Spironolactone is a potassium-sparing diuretic that is used to treat congestive heart failure, liver cirrhosis or nephrotic syndrome. In addition, it is used to diagnose or treat hyperaldosteronism and in the treatment or prevention of . The drug has been used for a long time in daily practice with noted side effects such as vomiting, diarrhoea, stomach pain, dry mouth, thirst, dizziness, gynecomastia, irregular periods and erectile dysfunction. In addition, in a few cases, rashes were an added side effect. Herein we describe a case and review the current available data.
CASE REPORT
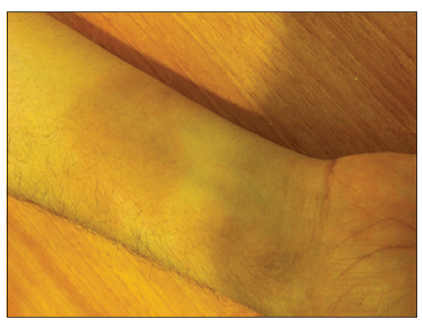
A 30-year-old male patient recently diagnosed with idiopathic cardiomyopathy, ejection fraction 30%, was started on ACEI and beta-blocker. When he visited the clinic for follow-up, he was started on spironolactone. On the 3rd day, he noted a macular rash on both arms [Figures 1-3], which was not itchy. The offending drug was stopped, and the rash started to fade out gradually and disappeared in 10 days.


Dermatological side effects are infrequent and usually would also have a more widespread effect:
- Uncommon (0.1%-1%): Rash, urticaria, erythema, chloasma, pruritus, and exanthema.
- Rare (< 0.1%): Eczema
- Very rare (< 0.01%): Alopecia, erythema annulare centrifugum, and hypertrichosis.
- Frequency not reported: Hirsutism, Stevens-Johnson syndrome, toxic epidermal necrolysis, drug rash with eosinophilia and systemic symptoms, maculopapular, or erythematous cutaneous eruptions [1].
Leukocytoclastic vasculitis or allergic form with red or purple skin rash that spreads and causes blistering and peeling, especially in the face or upper body had been reported.
The morphology and distribution of skin lesions resembling that of systemic lupus erythematosus had been described. Although the histologic changes in the skin biopsy specimen were consistent with SLE, there was, however, a negative serology [2].
Other reported skin manifestation was persisting pigment deposition with circumscribed spotty pigmentation of the skin after spironolactone allergy [3].
Topically applied spironolactone may be effective in the treatment of acne patients with high sebum secretion rates [4].
Spironolactone-induce rash, although infrequent, is a side effect worth considering.
REFERENCES
- Gupta AK, Knowles SR, Shear NH. Spironolactone-associated cutaneous effects: A case report and a review of the literature. Dermatology 1994;189:402-5.
- Uddin MS, Lynfield YL, Grosberg SJ, Stiefler R. Cutaneous reaction to spironolactone resembling lupus erythematosus. Cutis 1979;24:198-200.
- Luderschmidt C. Pigmented exanthema after spironolactone allergy in progressive systemic scleroderma. Dtsch Med Wochenschr 1983;108:1922-5.
- Yamamoto A, Ito M. Topical spironolactone reduces sebum secretion rates in young adults. J Dermatol 1996;23:243-6.