Current Update in the Management of Post-operative Neuraxial Opioid-induced Pruritus
Borja Mugabure Bujedo1
Citation : Bujedo, BM. Current Update in the Management of Postoperative Neuraxial Opioid Induced Pruritus. J Clin Res Anesthesiol 2018;1(1):1-10.
Itching is an extremely bothersome side effect that frequently appears after the epidural and intrathecal administration of opioids. This common side effect can be severe enough to be considered by the patient to be as bad or worse than the pain itself. Both prevention and treatments remain a challenge in the clinical management of these patients. Many drugs have been used to either treat or prevent the condition with variable results.
This article's purpose is to review the clinical literature and summarize the current evidence of efficacy and efficiency of pharmacological treatments available to manage opioid-induced pruritus mediated by spinal opioids in the post-operative setting. An analysis of how the mechanism of action of the most common drugs affects in their clinic usefulness is presented. This comprehensive review is limited to published papers in English, found on PubMed, Medline, and Scopus until December 2017. The papers used in this review were systematized reviews, randomized controlled trials, and opinion articles by subject experts.
The most useful drugs are mu opioid antagonists, such as naloxone, and mixed opioids kappa agonists/mu antagonists, such as nalbuphine and butorphanol, the latter being capable of maintaining analgesia in addition to reduce itching. Some efficacy has also been observed, to a lesser extent, from 5-hydroxytryptamine 3 serotonin receptor antagonists, such as prophylactically administered ondansetron, and D2 dopaminergic receptor antagonists, such as droperidol. Moreover, propofol at subanesthetic doses, midazolam, and prophylaxis with mirtazapine and oral gabapentin have been used with efficacy. Finally, a clinical practical guide is suggested for general management of pruritus induced by spinal opioids in the perioperative setting.
Butorphanol, nalbuphine, naloxone, neuraxial opioids, ondansetron, postoperative complications, pruritus
INTRODUCTION
Neuraxial opioids (NO) are one of the most widely used methods for postpartum analgesia, for cesarean section analgesia and many other surgical procedures.The benefit of spinal opioid administration is to increase and prolong post-operative analgesia [1]. A wide range of side effects has been described after routine use, of which pruritus is one of the most common. Its frequency is currently understated, and it is severely undertreated. The itching induced by NO is an unpleasant, subjective, and irritating sensation that causes scratching response. The symptoms usually begin in the trunk, nose, and around the eyes. Itching in the face is located in areas of the skin innervated by the ophthalmic branch of the trigeminal nerve [2]. The spinal nucleus of the trigeminal nerve is rich in opioid receptors and structurally close to the gelatinous substance Lissauer tract C3-C4. The ophthalmic branch of the spinal sensory nucleus of the trigeminal nerve is at lower anatomical level. This fact is probably the underlying anatomical cause for pruritus after NO administration to occur most often in the upper part of the face [3].
The average incidence of pruritus is around 83% in obstetric patients and 69% in non-pregnant patients, including men and women. Pregnant women appear to be more susceptible to pruritus after the administration of NO than other populations. In contrast, after orthopedic surgery, the incidence of pruritus after NO ranged from 30% to 60%. This higher incidence in the obstetric population may be due to the interaction of estrogens with opioid receptors [4].
Pruritus begins shortly after analgesia, with a variable onset depending on the type, route, and dose of opioids used. Pruritus caused by highly lipophilic opioids such as fentanyl and sufentanil is short-lived, and the use of the minimal effective dose and addition of local anesthetics seems to decrease the prevalence and severity of itching. Pruritus caused by intrathecal morphine, which is much hydrophilic, is long lasting and more difficult to treat [5]. Intrathecal administration of opioids reaches peak concentrations in the cerebrospinal fluid (CSF) almost immediately after epidural administration. There is, however, a delay before the maximum concentration is achieved in the brain (10-20 min with fentanyl and 1-4 h with morphine). Epinephrine coadministration may have an influence on epidural opioids and its side effects, including pruritus. As a vasoconstriction agent, epinephrine decreases the vascular absorption of opioids from the epidural space and may increase concentrations in the CSF and, therefore, possibly the severity of side effects [6].
The objective of this paper is to review the current body of literature describing studies that support the inclusion of adequate pharmacological therapies for both opioid induced pruritus (OIP) treatment and prevention and to analyze them based on the current understanding of the pathophysiology and mechanisms of pruritus induced by spinal opioids. A practical clinical guide on this topic is also suggested by the author.
The exact mechanism of how opioids induce pruritus is not precise. Many mechanisms have been proposed as the possible origin of the condition since there seems to be no single mechanism that can explain this phenomenon in all cases. Mechanisms that appear to be involved include:
- The activation of the "itch center" in the central nervous system.
- The medullary modulation through dorsal horn activation and the antagonism of the inhibitory transmitters of the descending pathways.
- The wrong way on modulation of the central serotonergic pathway.
- A theory that links pain and pruritus, with a process of peripheral sensitization and another central one.
and binds specifically to specific receptors located at the nociceptive nerve endings. The signal is then transmitted through retrograde axonal transport to the dorsal root ganglia, where neuropeptide gene expression and receptor molecules, such as vanilloid receptors (TRPV1), are increased in number and density. Trophic factors can also initiate the sensitization of nerve fibers, and therefore, change the morphology of sensory neurons. Similar mechanisms may be functioning in chronic pruritus as a mechanism of peripheral and central sensitization [4].
It is a scientific observation that the same population of sensory neurons transmits pain and pruritus. Non-myelinated small nerve fibers (C fibers) and the release of PGS (PGE1 and PGE2) are the primary mechanisms involved. All these tools improve the transmission of C fibers in the central nervous system, which can increase pruritus [7]. A high density of 5-hydroxytryptamine 3 (5-HT3) receptors (subtype 5-HT3) and opioid receptors are present on the superficial layers of the dorsal horn and in the nucleus of the spinal tract of the trigeminal nerve in the spinal cord. The trigeminal spinal nucleus located superficially in the medulla is an integrative center of sensory information of the face and contains an area known as the "itch center". The cephalic migration of NO to this center and the activation of 5-HT3 receptors by opioids may play a crucial role in the generation of neuraxial pruritus induced by opioids [4-9].
Opioids can also induce spinal pruritus by secondary neurons in dorsal plate horn and I Hawthorn-beam. The active broad range neurons of the dorsal horn inhibit these spinal neurons protecting us from itching. If mu spinal opioids weaken this inhibition, these neurons are activated and therefore causing itching without peripheral stimulation. It has been shown in experimental animal studies that medullar cord activation and pruritus production are observed in particular by the activation of mu opioid receptors (MOR) and that kappa opioid receptors (KOR) suppress the itching [10].
In this sense, two theories have been postulated which would support these affirmations:
- Molecular base: A recent study has somewhat revealed the molecular mechanism of pruritus induced by NO. Liu et al [11]. performed a series of elegant animal experiments, demonstrating the uncoupling of morphine-induced pruritus and the analgesia caused by this drug in the mouse spinal cord. They concluded that MOR in its MOR1D isoform is necessary for intrathecal morphine-induced pruritus and that gastrin-releasing peptide (GRPR receptor) in the spinal cord was also required. In particular, mu agonists induced itching and the scratching responses were almost abolished in "knock-out" GRPR mice, as well as by coadministration with a GRPR antagonist.
- The cellular base: The cellular mechanisms of pruritus induced by spinal opioids have been clarified in depth by the pharmacological studies in nonhuman primates. Ko et al., in an experimental setting, studied three types of opioid agonist receptors and their ability to elicit scratch responses across a wide range of analgesic doses. Interestingly, the results demonstrate that only mu agonists produce analgesic effects accompanied by pruritus and scratching in response. Other opioid receptor subtypes, such as KOR, delta (DOR), and nociceptin (NOR), did not mediate NO-induced pruritus [12].
MOST USEFUL DRUGS FOR EITHER OIP TREATMENT OR PREVENTION
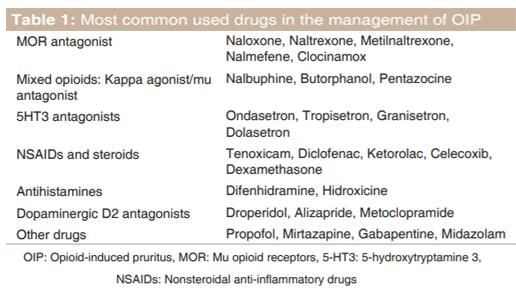
Both treatment and prevention of pruritus induced by NO are complicated, even after significant advances in knowledge in this field. However, at this moment, we have not been able to describe a definitive treatment for this irritable effect, but we believe that prevention is better than treat, so the use of minimal analgesic doses of neuraxial opiates has been recommended alone or in combination with a local anesthetic. This practice offers satisfactory analgesia with a very low incidence of pruritus. Several medications such as tenoxicam, diclofenac potassium, oral gabapentin before surgery, intravenous (IV) 5-HT3 antagonists, and sub-hypnotic propofol doses have shown positive but not consistent results for the prevention of spinal OIP and can be considered as a possible prophylactic and treatment therapy. These options are summarized in Table 1 [4].
The MOR is the primary receptor responsible for the modulation of pain and some side effects, especially pruritus and nausea or vomiting. Although naloxone is the most popular among anesthesiologist, other options are described below. Nalmefene, known initially as nalmetrene and developed in the mid-70s, is a MOR antagonist, which has been used primarily in the USA for the treatment of alcoholism and opioid overdose. This drug has also been investigated for the treatment of NO-induced pruritus in primates with excellent results. Ko et al. demonstrated how a single prophylactic dose of this drug (32 mcg/kg) could revert both effects, pruritus and intrathecal morphine-induced analgesia. This fact demonstrated for the authors, how the therapeutic window is indeed very close to the production of analgesia and pruritus, both effects mediated by mu receptors [13]. Pre-treatment with clocinamox, a mu selective antagonist, inhibits scratching induced by primate spinal opioids, but neither ?-opioid antagonism (binaltorfimine) nor delta (naltrindole) antagonists produce this effect. This fact would explain the essential antipruritic role of mu receptor antagonists [14]. It seems that a dose of 0.25-1 mcg/kg/h through IV route is the most effective without affecting analgesia. A systematic review in 2001 with 834 patients [15] concluded that IV naloxone was a useful drug in the treatment of pruritus induced by NO, without increasing the pain score. Moreover, naloxone doses >2 mcg/kg/h were more likely to lead to the reversal of analgesia and therefore are not advisable for clinical practice. Another recent meta-analysis [16] about the efficacy of IV naloxone, either as a continuous infusion or patient-controlled analgesia, revealed that naloxone was associated with a significant decrease in nausea or pruritus without any increase in pain scores.
Several studies have evaluated the efficacy of naloxone, naltrexone, and methylnaltrexone in the prevention of pruritus, but variable results have been observed, especially for oral administration in both adult and pediatric populations. Based on existing data, a low dose, intravenously, or infused naloxone has the most significant evidence for the prevention of neuraxial opioid induced pruritus in adults. Continuous infusion produces less fluctuation of the concentrations of naloxone than bolus injections and compensates for the relatively short naloxone half-life [17]. On the other hand, a recent meta-analysis demonstrated the efficacy of naloxone in the prevention and treatment of adverse effects of opioid drugs. After a hard and selective selection, only six studies were included in which the authors examined the effects of naloxone on opioid-induced pruritus (OIP) (4 of them through spinal and two by systemic pathways). The analysis showed that there was significant heterogeneity among the included studies (I2 = 60.3 %, P = 0.027). Consequently, the meta-analysis was based on the random effects model. Their results indicated that the rate of incidence of OIP was significantly lower in the naloxone group versus the control group (relative risk [RR] = 0.252, 95% confidence interval [CI] = 0.137-0.464, P = 0.000) [18].
Under the results of a recent study, a single 12 mg dose of subcutaneous methylnaltrexone bromide failed to reduce the overall severity and incidence of pruritus among an obstetric population on receipt of fentanyl 15 mcg and 100 mcg of intrathecal morphine, during spinal anesthesia for cesarean section. Prophylactic treatment with a peripheral mu antagonist was ineffective against intrathecal morphine-induced pruritus in the peripartum, although a small clinical effect could not be excluded [19]. In this sense, the results were similar in a study in orthopedic surgery. Subcutaneous methylnaltrexone was not effective in decreasing post-operative urinary retention and pruritus, but it reduced the rate of nausea and vomiting, all the patients receiving 10 mg 0.5% hyperbaric bupivacaine plus 0.1 mg preservative-free morphine sulfate [20].
Mixed opioids, μ-antagonist/? -agonists such as nalbuphine, or MOR and KOR partial agonists such as butorphanol and pentazocine have a great potential to attenuate NO adverse effects and also to improve the analgesic effects on the KOR. Experimental studies have shown that both μ antagonists and ? agonists are effective in relieving intrathecal morphine-induced itching induced in primates [21]. The efficacy of nalbuphine, butorphanol, or pentazocine has been studied with positive results [22,23]. Tamdee et al [24]. conducted a randomized trial to investigate the efficacy of pentazocine for the treatment of pruritus associated with intrathecal injection of morphine. The authors concluded that pentazocine at a dose of 15 mg was superior to ondansetron 4 mg for the treatment of pruritus induced by intrathecal morphine.
In a systematic review recently published on nalbuphine in 2016, 10 studies with 1129 patients met all inclusion criteria, of which 9 were randomized controlled trials and 1 clinical case report [25]. The incidence of pruritus was higher among patients receiving NO than those with IV infusion. Nalbuphine provided higher efficacy in the treatment of OIP, as compared to placebo, or other pharmacological agents such as diphenhydramine, naloxone, and propofol. There was no attenuation of analgesia or increase in sedation with low doses
of nalbuphine treatment; 25-50% of the dose recommended to treat pain (2.5-5 mg vs. 10 mg). Furthermore, nalbuphine was associated with a reduction in nausea or vomiting and even the reversion of respiratory depression. Their findings were that nalbuphine was superior to treat OIP in patients who received NO for acute pain related to surgery or childbirth. Therefore, they recommended that nalbuphine should be used as a first-line treatment of OIP. Authors explained the lack of transfer of these conclusions to clinical practice due to the absence of an evidence-based clinical guide in this field. Other related facts were the counter-intuitive fact of treating the adverse effects of an opioid drug with another opioid, the off-label use of nalbuphine for the treatment of pruritus, and even the higher price compared to other drugs in the North American market. Moreover, this drug has not shown the same efficacy in children [26], although its lower passage to breast milk than other opioids makes it an attractive option in the obstetric population [25]. In a recent review, the author concluded that nalbuphine was a beneficial adjunct to intrathecal local anesthetics because of the excellent duration of analgesia, antipruritic, anti-shivering properties, minor respiratory depression, and nausea and vomiting so that its acceptance will become widespread [27].
A systematic review on the efficacy of butorphanol in OIP was published in 2013 [28]. The relevant results of 16 trials (n = 795 patients) were analyzed. Butorphanol, IV, and epidural reduced pruritus with a RR of 0.22 (95% CI: 0.10-0.45) and RR 0.24 (95% CI: 0.16-0.36), respectively. The use of epidural butorphanol reduced the number of patients who requested rescue therapy for pruritus (RR 0.57, 95% CI 0.41-0.81). Butorphanol decreased the intensity of post-operative pain at 4, 8, and 12 h. Differences in visual analog scale scores were -0.29 (95% CI: -0.52 to -0.05), -0.30 (95% CI: -0.56 to -0.04), and -0.23 (95% CI: -0.46 to -0.01), respectively. However, epidural but not intravenous butorphanol reduced the overall incidence of post-operative nausea and vomiting (PONV) (RR: 0.35; 95% CI: 0.19- 0.66) . Butorphanol did not increase respiratory depression (RR: 0.71, 95% CI 0.31-1.63) or dizziness (RR: 2.45, 95% CI: 0.35-17.14) or drowsiness (RR: 0.71, 95% CI: 0.22- 2.37). Butorphanol administered with morphine may be an effective strategy to prevent itching and also decrease the intensity of pain and PONV without increasing other side effects. Therefore, the authors concluded that it might be recommended to prevent NO-induced pruritus during the perioperative period.
The main conclusion of this section is that mixed opioids and μ-antagonist/?-agonists can prevent and are useful in the treatment of NO-induced pruritus. These drugs do not induce an increase in basal pain, but at the expense of an increase in adverse effects such as drowsiness, they should only be used at doses lower than those recommended to achieve clinical analgesia.
The exact mechanism of ondansetron that relieves pruritus is unknown. Although 5-HT 3 receptors can be identified in the spinal cord of rodents and primates, there is no anatomical evidence for colocalization of 5-HT3 receptors with MOR in the spinal cord or functional tests to corroborate the interaction between the 5-HT3 receptor and MOR in any of the animal models studied previously. Unpublished data from Kolab showed that intrathecal morphine administration (32 μg) resulted in a broad scratching sensation (~600 scratches at 15 min/sampling time) in Rhesus Monkeys (n = 8). IV ondansetron (0.1-3.2 mg/kg) was administered approximately 2 h after the subjects received intrathecal morphine study dose. Within these doses evaluated in the present study, ondansetron was ineffective in attenuating pruritus induced by intrathecal morphine. A higher dose of ondansetron (10 mg/kg) caused extrapyramidal reactions in the monkeys (involuntary contractures, stiffness in both legs, and spasm of the extensor muscles) leading to the completion of the experiments. In consequence, this author does not support the routine use of these drugs in humans [12].
Otherwise, 5-HT3 receptors are very plenty in the dorsal horn of the spinal cord and the spinal tract of the trigeminal nerve. Therefore, the interaction between opioids and 5-HT3 receptors may play a decisive role in the generation of OIP. 5-HT3 antagonists, such as ondansetron, dolasetron, and granisetron, have been studied prophylactically to prevent OIP. A systematic review (n = 1337) of 15 randomized controlled trials [29] indicated that prophylactic treatment with IV bolus of 5-HT3 receptor antagonists might provide a significant decrease in incidence and itching intensity score after NO administration, particularly when intrathecal morphine and non-lipophilic opioids are used. Authors also found a substantial reduction in the use of rescue drugs for the treatment of pruritus. The dosages for ondansetron used were 4 mg and 8 mg or 0.1 mg/kg. Other 5-HT3 receptor antagonist studies that gave good results were tropisetron (5 mg), granisetron (3 mg), and dolasetron (12.5 mg).
In another recent meta -analysis in 2016, the most commonly used 5-HT3-receptor antagonist in clinical practice did not reduce the incidence of pruritus following injection of lipophilic opioids such as fentanyl or sufentanil. IV 8 mg ondansetron prophylaxis did not decrease the incidence of pruritus but may minimize the need for rescue medication in specific subgroups, especially those including non-obstetric surgery and in patients who received the drug before the administration of spinal opioids [30]. One of the postulated mechanisms is that morphine being less lipophilic and slower at the beginning of analgesia results in a higher concentration of residual opioid in the CSF and greater cephalic migration. As the peak concentration of ondansetron occurs about
15 min, 5-HT3 antagonists can reach 5-HT3 receptors in the spinal cord before morphine but not after lipophilic drugs [31]. Studying specifically pregnant women submitted to the cesarean section under spinal anesthesia with intrathecal morphine, a systematic review with meta-analysis [32], verified that the prophylactic treatment with 5-HT3 receptor antagonists was ineffective in reducing the incidence of pruritus. Moreover, these drugs significantly reduced the severity and the need for treatment of this adverse effect, the frequency of nausea, as well as the need for rescue antiemetic drugs. The drugs were also effective for the treatment of established pruritus. However, in a recent traditional meta-analysis [33], the results demonstrated that prophylactic ondansetron did not show the preventive efficacy of OIP in obstetric patients (7 trials, RR = 0.84, 95% CI: 0.69-1.03, P= 0.10) with apparent heterogeneity (I2 = 82%). Otherwise, it could significantly reduce the incidence of neuraxial morphine-induced pruritus (NMIP) in non-obstetric patients (3 trials, RR = 0.63, 95% CI: 0.45-0.89, P = 0.008) with modest heterogeneity (I2 = 47%). However, the subsequent trial analysis demonstrated the need of more high-quality randomized controlled trials to confirm the preventive efficacy of ondansetron on NMIP in non-obstetric populations and to study whether it prevents NMIP in obstetric patients. In conclusion, prophylactic ondansetron can significantly reduce the incidence of NMIP in non-obstetric patients, but this fact could be not right in obstetric patients. Finally, better-designed trials are still required to test the reliability of these results.
NSAIDs have a well-recognized role in post-operative pain relief. They inhibit cyclooxygenase (COX) and decrease the formation of PGs involved in the peripheral tissue inflammatory process. It has been shown that tenoxicam IV [34] and diclofenac rectal [35] have certain antipruritic effects in patients receiving spinal opioids. However, Gulhas et al [7]. found no decrease in pruritus with the use of lornoxicam after intrathecal fentanyl administration. Celecoxib, a COX-2 selective NSAID, has shown variable results in studies of antipruritic effects. Lee et al [36]. found no pruritus reduction with oral celecoxib after intrathecal administration of morphine. Their study showed no significant antipruritic or analgesic effect in a single dose of 200 mg (administered after delivery) within the first 24 h after a cesarean section. However, Samimi et al. [37], using 400 mg celecoxib orally 1 h before surgery, demonstrated efficacy in reducing the incidence of intrathecal morphine-induced pruritus in this subgroup of patients undergoing cesarean section.
Another experimental study (unpublished Kolab data) compared the effects of ketorolac and nalmefene on Rhesus Monkeys (n = 5). Any of the two drugs, nalmefene (32 μg/ kg) or ketorolac (10 mg/kg) was administered intravenously 2 h after the subjects received intrathecal morphine (32 μg). In this experimental setting, IV nalmefene, but not ketorolac, significantly reduced the scratch response to pruritus. Based on these results, NSAIDs cannot be used for treating neuraxial OIP. According to Ko [12], it seems unlikely that PGs play an important role as mediators of itching associated with NO.
Besides, another drug with an apparent protective effect against PONV such as dexamethasone has been shown to be ineffective in preventing OIP. In a systematic review with meta-analysis in patients undergoing cesarean section or hysterectomy under regional anesthesia with intrathecal morphine, pre-operative administration of 5-10 mg IV dexamethasone significantly reduced PONV but not the incidence of pruritus versus placebo [38].
Although morphine may trigger histamine release from mast cells, clinical studies have indicated that antihistamines are not effective in relieving OIP [39]. Pharmacological studies in non-human primates also found that an antihistamine such as diphenhydramine, over a wide range of doses, could not attenuate intrathecal morphine-induced pruritus [14]. Besides, other MOP agonists such as fentanyl and alfentanil do not stimulate the release of histamine, however they evoke pruritus or scratching in humans and non-human primates [40]. As tachyphylaxis develops rapidly in the local response to histamine, its role is minimal in the central processes of OIP. H1 blockers, therefore, have little or no effect on opioid central pruritus. However, first-generation H1 receptor antagonists such as hydroxyzine or diphenhydramine may produce a sedative effect, which could sometimes be useful in patients with pruritus. The proposed mechanism would be an interruption of the entire itching-scratching cycle, providing a better quality of sleep, which is necessary, but they are not very effective in reducing the severity of itching [4,12].
Since recent years, propofol has been used for the treatment and prevention of pruritus. Its antipruriginous action is exerted through the inhibition of the posterior horn of the spinal cord. Many studies have been conducted with subhypnotic doses of propofol, ranging from 10 mg bolus to 30 mg for 24 h infusion, but the results were contradictory [4,12,39].
A prospective double-blinded randomized trial aimed at comparing the effects of propofol, midazolam, and a combination of both drugs on the prevention of pruritus induced by intrathecal sufentanil. Eighty-four patients undergoing spinal anesthesia with 3 mL hyperbaric bupivacaine 0.5% and 5 μg sufentanil (1 mL) were randomly allocated to one of the three study groups: Group 1, who were administered 20 mg IV propofol bolus, then 50 μg/kg/min IV infusion; Group 2, who were administered 0.03 mg/kg IV midazolam bolus, then 0.02 mg/kg/h IV infusion; and Group 3, who were administered 10 mg IV propofol and 0.015 mg/ kg IV midazolam bolus, then 25 μg/kg/min propofol and 0.01 mg/kg/h midazolam IV infusion. The incidence rates and severity of pruritus were assessed intraoperatively and postoperatively for 24 hours. Overall results were as follows: 17 patients in the propofol group (60.7%), eight patients in the midazolam group (28.6%), and nine patients in the propofol-midazolam group (32.1%) developed pruritus (P = 0.027). Intraoperative pruritus was observed in seven patients in the propofol group (25%), two patients in the midazolam group (7.1%), and five patients in the midazolam-propofol group (17.9%) (P = 0.196). Post-operative pruritus developed in 12 patients in the propofol group (42.9%), six patients in the midazolam group (21.4%), and four patients in the midazolam-propofol group (14.3%) (P = 0.041). There was no significant difference between the groups with respect to the severity of pruritus (P > 0.05). Author's conclusions showed that, the administration of 0.03 mg/kg IV midazolam bolus followed by 0.02 mg/kg/h could be more effective than propofol in the prevention of intrathecal sufentanil-induced pruritus without increasing sedation and other side effects [41].
Droperidol and alizapride have also been used for the treatment of OIP. Both are potent antagonists of dopamine D2 receptors. Droperidol also has weak anti-5-HT3 activity. In the Horta et al. study, on 300 women undergoing a cesarean section with 0,2 mg intrathecal morphine, the subgroup receiving IV droperidol showed the lower prevalence of pruritus compared to placebo and also compared to propofol, alizapride, and promethazine. The droperidol, propofol and alizapride groups had significantly lower incidences of pruritus compared with the control and promethazine groups, while the incidence of pruritus was similar among the patients assigned to the promethazine and control groups. As for the prevention of moderate and severe pruritus, droperidol had the lowest NNT (3.52; 95% CI: 3.37-3.67), followed by propofol (4.61; 95% CI: 4.45-4.77) and alizapride (5.43; 95% CI: 5.27-5.59). As for untoward effects, droperidol and promethazine increased the incidence of somnolence, which seemed more severe with promethazine. Metoclopramide, another dopamine D2 receptor antagonist, has been shown to be ineffective in this regard [39].
Mirtazapine is a new antidepressant that selectively blocks 5-HT2 and 5-HT3 receptors. This drug has a unique pharmacological profile, since apart from increasing noradrenergic and serotonergic neurotransmitters, mirtazapine can exert its antidepressive and anti-nociceptive action through the ?-opioid-dependent system. Its antipruritic activity was first described by Davis et al [42]. who studied its ability to reduce intrathecal morphine-induced pruritus. Sheen et al [43]. conducted a study on the strength of mirtazapine to prevent pruritus induced by intrathecal morphine and concluded that pre-operative oral administration of 30 mg decreased the incidence, delayed onset time, decreased severity, and shortened the duration of pruritus. Mirtazapine may act on the cerebral cortex to reduce the perception of pruritus, and it presents a high antihistamine effect. The most frequent adverse effects were drowsiness, dizziness, and dry mouth that appeared in 50% of patients. From the pharmacokinetic point of view, this drug has another advantage over the first-generation 5-HT3 receptor antagonists; The peak concentration of mirtazapine is reached 2 h after a single dose, and the elimination half-life ranges from 20 h to 40 h, allowing the drug to cover the entire duration of pruritus in the post-operative period [44].
Gabapentin is an anticonvulsant, a structural analog of ?-aminobutyric acid. Some studies have shown how gabapentin to be effective under varied conditions of chronic itching. Sheen et al [45]. studied the role of gabapentin in the treatment of intrathecal pruritus induced by morphine. They concluded that gabapentin 1200 mg pre-operative, decreased incidence, delayed onset time, decreased severity, and shortened duration of pruritus due to intrathecal morphine. They observed that this effect might be due to the multimodal antipruritic action of gabapentin that includes the reduction at the central level of the perception of itching. It may also exhibit a modulatory effect on neurotransmitter release, which reduces the excitability of spinal and supraspinal neurons during the transmission of itching and inhibition of the supraspinal cord through serotonergic circuits. Chiravanich et al [46]. underwent a controlled clinical trial in a single dose of gabapentin as prevention of intrathecal morphine-induced pruritus in orthopedic surgery. They concluded that gabapentin 600 mg preoperatively did not significantly reduce post-operative intrathecal pruritus induced by morphine. Therefore, the anti-pruriginous efficacy, dosage, and pharmacological mechanisms of gabapentin in this field need further studies.
Within traditional Chinese medicine, acupuncture has been used for many purposes including improving the side effects of opioids. In a study of 60 patients undergoing transurethral resection of the prostate under regional anesthesia with intrathecal morphine and subsequent postoperative epidural analgesia, the side effects of opioids were found to be lower than the placebo group. Based on this study, acupuncture may decrease the incidence of morphine-related side effects (nausea and vomiting, pruritus, and gastrointestinal disorders) when the function of the spinal cord is intact. However, there was a decrease in the incidence of pruritus but not for gastrointestinal dysfunction when the spinal cord was blocked under the effect of regional anesthesia [47]
CLINICAL PRACTICE GUIDE (CPG)
In the development of a CPG, the concepts of quality, level of evidence, and degree of recommendation are at the heart of the definition of evidence-based CPG, since they are the instruments that attempt to standardize and provide clinicians with solid rules for valuing. Published research determines its validity and summarizes its usefulness in clinical practice. Different institutions and scientific societies have also contemplated many differences in the appreciation of the quality of the evidence and have been developing various classification systems to evaluate and structure the evidence and establish the degrees of recommendation. There are currently more than 100 rating systems for assessing evidence. The best-known and used classifications in our environment are as follows:
- Canadian Task Force on Preventive Health Care (CTFPHC).
- US Preventive Services Task Force (USPSTF) (Currently integrated into Agency for Healthcare Research and Quality-AHRQ)
- US Agency for Health Care Policy and Research (AHRQ)
- Center for Evidence-Based Medicine, Oxford (OCEBM)
- Scottish Intercollegiate Guidelines Network (SIGN)
- National Institute for Clinical Excellence (NICE)
- Grading of Recommendations Assessment, Development and Evaluation Working Group (GRADE)
Evidence-Based Health Care: Practice guideline levels of evidence and grades of recommendations used by the National Guideline Clearinghouse.
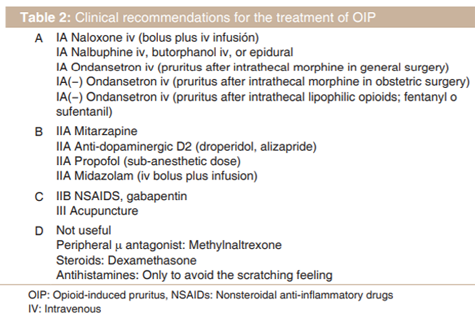
IA: Evidence from meta-analysis of randomized controlled trials
IB:Evidence from at least one randomized controlled trial IIA:Evidence from at least one controlled study without randomization
IIB:Evidence from at least one other type of quasi-experimental study
III:Evidence from non-experimental descriptive studies, such as comparative studies, correlation studies, and case- control studies
IV:Evidence from expert committee reports or opinions or clinical experience of respected authorities, or both
A:Directly based on Level I evidence
B:Directly based on Level II evidence or extrapolated recommendations from Level I evidence
C:Directly based on Level III evidence or extrapolated recommendations from Level I or II evidence
D:Directly based on Level IV evidence or extrapolated recommendations from Level I, II, or III evidence
CONCLUSIONS
The incidence of pruritus following intrathecal administration of opioids varies between 30 and 100% without significant differences depending on the opioid involved, being higher in the pregnant woman and the mixtures with adrenaline. It usually presents in face and trunk and is mediated by an unknown mechanism although the modulation of the serotoninergic system seems to play an important role. Histamine release does not appear to be involved and a central mechanism must exist since the use of antagonists such as naltrexone and naloxone reverses the condition. Antihistamines are only useful to reduce scratching. Serotoninergic receptor antagonists 5HT-3 as ondansetron (4-8 mg iv) have shown some effectiveness in preventing and treating this symptom. However, it could be ineffective after intrathecal morphine in obstetric patients and after intrathecal fentanyl or sufentanil. Propofol in subhypnotic doses (10 mg IV bolus without or with 30 mg infusion for 24 h) and prophylactic oral mirtazapine (30 mg) have also been shown to be effective.
In summary, accumulated pharmacological evidence supports MOR antagonists such as naloxone and mixed partial agonists KOR/MOR as the most effective treatment options for spinal OIP. The remaining therapeutic options in the management of non-opioid ligands, such as 5-HT3 antagonists, antihistamines, and NSAIDs, have not shown sufficient efficacy to be considered as the first line of treatment in this field. On the other hand, IV nalbuphine (4 mg) seems to demonstrate the greater effectiveness and should be considered as the first line of treatment of OIP[49].
DISCLOSURES
Part of this article has been previously published in Journal of Anesthesia and Critical Care: Open Access. Volume 6 Issue 2 - 2016, and The Open Pain Journal, 2017, 10, 14-21. The author (Borja Mugabure Bujedo, MD) of these open access articles retains the copyright, so the text can be used if properly cited. References no 6, 49.
References
- Ballantyne JC, Loach AB, Carr DB. Itching after epidural and spinal opiates. Pain 1988;33:149-60.
- Szarvas S, Harmon D, Murphy D. Neuraxial opioid-induced pruritus: A review. J Clin Anesth 2003;15:234-9.
- Kam PC, Tan KH. Pruritus: Itching for a cause and relief? Anaesthesia 1996;51:1133-8.
- Kumar K, Singh SI. Neuraxial opioid-induced pruritus: An update. J Anaesthesiol Clin Pharmacol 2013;29:303-7.
- Reich A, Szepietowski JC. Opioid-induced pruritus: An update. Clin Exp Dermatol 2010;35:2-6.
- Bujedo BM. An update on neuraxial opioid-induced Pruritus prevention. J Anesth Crit Care Open Access 2016;6:226.
- Gulhas N, Erdil FA, Sagir O, Gedik E, Togal T, Begec Z, et al. Lornoxicam and ondansetron for the prevention of intrathecal fentanyl-induced pruritus. J Anesth 2007;21:159-63.
- Ganesh A, Maxwell LG. Pathophysiology and management of opioid-induced pruritus. Drugs 2007;67:2323-33.
- Schmelz M. Opioid-induced pruritus. Mechanisms and treatment regimens. Anaesthesist 2009;58:61-5.
- Andrew D, Craig AD. Spinothalamic lamina I neurons selectively sensitive to histamine: A central neural pathway for itch. Nat Neurosci 2001;4:72-7.
- Liu XY, Liu ZC, Sun YG, Ross M, Kim S, Tsai FF, et al. Unidirectional cross-activation of GRPR by MOR1D uncouples itch and analgesia induced by opioids. Cell 2011;147:447-58.
- Ko MC. Neuraxial opioid-induced itch and its pharmacological antagonism. Handb Exp Pharmacol 2015;226:315-35.
- Ko MC, Naughton NN. An experimental itch model in monkeys: Characterization of intrathecal morphine-induced scratching and antinociception. Anesthesiology 2000;92:795-805.
- Ko MC, Song MS, Edwards T, Lee H, Naughton NN. The role of central mu opioid receptors in opioid-induced itch in primates. J Pharmacol Exp Ther 2004;310:169-76.
- Kjellberg F, Tramer MR. Pharmacological control of opioid-induced pruritus: A quantitative systematic review of randomized trials. Eur J Anaesthesiol 2001;18:346-57.
- Murphy JD, Gelfand HJ, Bicket MC, Ouanes JP, Kumar KK, Isaac GR, et al. Analgesic efficacy of intravenous naloxone for the treatment of postoperative pruritus: A meta-analysis. J Opioid Manag 2011;7:321-7.
- Miller JL, Hagemann TM. Use of pure opioid antagonists for management of opioid-induced pruritus. Am J Health Syst Pharm 2011;68:1419-25.
- He F1, Jiang Y, Li L, The effect of naloxone treatment on opioid-induced side effects: A meta-analysis of randomized and controlled trails. Medicine (Baltimore) 2016;95:e4729.
- Paech M, Sng B, Ng L, Nathan E, Sia A, Carvalho B. Methylnaltrexone to prevent intrathecal morphine-induced pruritus after caesarean delivery: A multicentre, randomized clinical trial. Br J Anaesth 2015;114:469-76.
- Zand F, Amini A, Asadi S, Farbood A. The effect of methylnaltrexone on the side effects of intrathecal morphine after orthopedic surgery under spinal anesthesia. Pain Pract 2015;15:348-54.
- Ko MC, Lee H, Song MS, Sobczyk-Kojiro K, Mosberg HI, Kishioka S, et al. Activation of kappa opioid receptors inhibits pruritus evoked by subcutaneous or intrathecal administration of morphine in monkeys. J Pharmacol Exp Ther 2003;305:173-9.
- Lawhorn CD, McNitt JD, Fibuch EE, Joyce JT, Leadley RJ Jr. Epidural morphine with butorphanol for postoperative analgesia after cesarean delivery. Anesth Analg 1991;72:53-7.
- Charuluxananan S, Kyokong O, Somboonviboon W, Lertmaharit S, Ngamprasertwong P, Nimcharoendee K. Nalbuphine versus propofol for treatment of intrathecal morphine-induced pruritus after cesarean delivery. Anesth Analg 2001;93:162-5.
- Tamdee D, Charuluxananan S, Punjasawadwong Y, Tawichasri C, Patumanond J, Sriprajittichai P. A randomized controlled trial of pentazocine versus ondansetron for the treatment of intrathecal morphineinduced pruritus in patients undergoing cesarean delivery. Anesth Analg 2009;109:1606-11.
- Jannuzzi RG. Nalbuphine for treatment of opioid-induced pruritus: A systematic review of literature. Clin J Pain 2016;32:87-93.
- Nakatsuka N, Minogue SC, Lim J, Montgomery CJ, Court CA, Malherbe S, et al. Intravenous nalbuphine 50 microg x kg (-1) is ineffective for opioid-induced pruritus in pediatrics. Can J Anaesth 2006;53:1103-10.
- Raghuraman MS. Intrathecal nalbuphine. Will it gain wider acceptance? A narrative review. Egypt J Anaesth 2017;33:289-93.
- Du BX, Song ZM, Wang K, Zhang H, Xu FY, Zou Z, et al. Butorphanol prevents morphine-induced pruritus without increasing pain and other side effects: A systematic review of randomized controlled trials. Can J Anaesth 2013;60:907-17.
- Bonnet MP, Marret E, Josserand J, Mercier FJ. Effect of prophylactic 5-HT3 receptor antagonists on pruritus induced by neuraxial opioids: A quantitative systematic review. Br J Anaesth 2008;101:311-9.
- Prin M, Guglielminotti J, Moitra V, Li G. Prophylactic ondansetron for the prevention of intrathecal fentanyl- or sufentanil-mediated pruritus: A meta-analysis of randomized trials. Anesth Analg 2016;122:402-9.
- Pernia A, Calderon E, Pla EC, Torres LM. Ondansetron in the treatment of the pruritus associated with the spinal infusion of opiates. Rev Esp Anestesiol Reanim 2000;47:425-6.
- George RB, Allen TK, Habib AS. Serotonin receptor antagonists for the prevention and treatment of pruritus, nausea, and vomiting in women undergoing cesarean delivery with intrathecal morphine: A systematic review and meta-analysis. Anesth Analg 2009;109:174-82.
- Wang W, Zhou L, Sun L. Ondansetron for neuraxial morphine-induced pruritus: A meta-analysis of randomized controlled trials. J Clin Pharm Ther 2017;42(4):383-393.
- Colbert S, O'Hanlon DM, Chambers F, Moriarty DC. The effect of intravenous tenoxicam on pruritus in patients receiving epidural fentanyl. Anaesthesia 1999;54:76-80.
- Colbert S, O'Hanlon DM, Galvin S, Chambers F, Moriarty DC. The effect of rectal diclofenac on pruritus in patients receiving intrathecal morphine. Anaesthesia 1999;54:948-52.
- Lee LH, Irwin MG, Lim J, Wong CK. The effect of celecoxib on intrathecal morphine-induced pruritus in patients undergoing caesarean section. Anaesthesia 2004;59:876-80.
- Samimi S, Tanha FD, Malekian M. A blinded study using celecoxib for prevention of morphine induced pruritus in patients undergoing cesarean section. J Fam Reprod Health 2011;2:35-9.
- Allen TK, Jones CA, Habib AS. Dexamethasone for the prophylaxis of postoperative nausea and vomiting associated with neuraxial morphine administration: A systematic review and meta-analysis. Anesth Analg 2012;114:813-22.
- Horta ML, Morejon LC, da Cruz AW, Santos GR, Welling LC, Terhorst L, et al. Study of the prophylactic effect of droperidol, alizapride, propofol and promethazine on spinal morphine-induced pruritus. Br J Anaesth 2006;96:796-800.
- Ellis DJ, Millar WL, Reisner LS. A randomized double-blind comparison of epidural versus intravenous fentanyl infusion for analgesia after cesarean section. Anesthesiology 1990;72:981-6.
- Makarem J, Mireskandari SM, Jafarzadeh A, Nikoukar LR, Aghaii S. Intravenous midazolam as more effective than propofol for preventing pruritus after intrathecal sufentanil in surgical patients: A randomized blinded trial. Anesth Pain Med 2016;7:e37535.
- Davis MP, Frandsen JL, Walsh D, Andresen S, Taylor S. Mirtazapine for pruritus. J Pain Symptom Manage 2003;25:288-91.
- Sheen MJ, Ho ST, Lee CH, Tsung YC, Chang FL, Huang ST. Prophylactic mirtazapine reduces intrathecal morphine-induced pruritus. Br J Anaesth 2008;101:711-5.
- Timmer CJ, Sitsen JM, Delbressine LP. Clinical pharmacokinetics of mirtazapine. Clin Pharmacokinet 2000;38:461-74.
- Sheen MJ, Ho ST, Lee CH, Tsung YC, Chang FL. Preoperative gabapentin prevents intrathecal morphine-induced pruritus after orthopedic surgery. Anesth Analg 2008;106:1868-72.
- Chiravanich W, Oofuvong M, Kovitwanawong N. Single dose of gabapentin for prophylaxis intrathecal morphine-induced pruritus in orthopedic surgery: A randomized controlled trial. J Med Assoc Thai 2012;95:186-90.
- Jiang YH, Jiang W, Jiang LM, Lin GX, Yang H, Tan Y, et al. Clinical efficacy of acupuncture on the morphine-related side effects in patients undergoing spinal-epidural anesthesia and analgesia. Chin J Integr Med 2010;16:71-4.
- Shekelle PG, Woolf SH, Eccles M, Grimshaw J. Developing clinical guidelines. West J Med 1999;170:348-51.
- Bujedo BM. Why do pain physicians not routinely use mixed opioids for the prevention of neuraxial opioid-induced pruritus? Open Pain J 2017;10:14-21.