Transfusion and Postoperative Outcome in Pediatric Abdominal Surgery
Claudine Kumba1, S. Querciagrossa1, T. Blanc2, J. M. Treluyer3
2. Department of Pediatric Digestive and Urologic Surgery, Necker Enfants Malades University Hospital, France
3. Department of Clinical Research and Pharmacology, Necker Enfants Malades and Cochin University Hospitals, Assistance Publique Hopitaux de Paris, Paris Descartes University, France
Citation: Kumba C, Querciagrossa S, Blanc T, Treluyer JM. Transfusion and Postoperative Outcome in Pediatric Abdominal Surgery. J Clin Res Anesthesiol 2018;1(1):1-8.
Intraoperative and post-operative morbimortality factors are multiple in pediatric patients. Studies in pediatric cardiac surgery and intensive care patients have identified transfusion as one independent factor among others. This study was undertaken to investigate whether transfusion was an independent factor of morbimortality in pediatric abdominal surgical patients.
The objective of the study is to identify morbimortality risk factors in intraoperatively transfused and not transfused pediatric abdominal surgical patients.
This was a retrospective observational descriptive pediatric cohort study.
Monocentric pediatric tertiary center, Necker-Enfants Malades University Hospital, Paris, from January 1, 2014, to May 17, 2017.
193 patients with a median age of 27.5 months (1.0-100.5) were included in the study. Inclusion criteria were the presence or the absence of transfusion in the intraoperative period in abdominal surgery patients. Exclusion criterion was transfusion in the post-operative period until discharge from hospital and non-abdominal surgical patients.
Primary outcome was mortality and secondary outcome was morbidity in transfused and non-transfused patients. Mortality was assessed by deaths occurring intraoperatively or post-operatively during the entire hospitalization. Morbidity was assessed by intraoperative, post-operative complications, repeat surgery, length of stay in the intensive care unit (LOSICU), in the hospitalization ward, total length of stay in hospital and length of mechanical ventilation (LMV).
Transfusion was the independent predictive risk factor for post-operative complications (odds ratio 1.14; P 0.02) and an independent predictive risk factor for repeat surgery (odds ratio 1.11; P 0.01). Emergency surgery was an independent predictive risk factor for repeat surgery (odds ratio 5.63; P = 0.01). Transfusion, age, emergency surgery, and American Society of Anesthesiologists score status were independent predictive risk factors for LOSICU, total length of hospital stay, and LMV (P < 0.01).
Transfusion was identified as an independent morbidity risk factor among others in this pediatric population. Identifying these factors to implement improvement measures can upgrade patient post-operative outcome. One of these measures is to implement transfusion protocols in which blood-product administration is guided by point of care devices such as viscoelastic methods which can contribute to reduce transfusion intraoperatively in potential hemorrhagic surgical interventions.
, postoperative outcome, pediatric abdominal surgery
INTRODUCTION
In pediatric patients admitted for surgery under anesthesia, morbimortality is related to multiple factors. Several morbimortality risk factors have been identified of which transfusion is one of the independent risk factors in studies concerning pediatric cardiac surgery and critical care patients [1]-[3]. This study was undertaken to determine whether transfusion is an independent morbimortality risk factor in abdominal surgical pediatric patients. The primary endpoint was to identify factors related to mortality and the secondary endpoint was to identify factors related to morbidity in this pediatric population. Mortality (primary outcome) was assessed by deaths occurring intraoperatively or post-operatively until discharge from hospital. Morbidity (secondary outcome) was assessed by intraoperative and post-operative complications, repeat surgery, length of stay in the intensive care unit (LOSICU), length of stay in hospital (LOSHOSP), total LOSHOSP (intensive care and standard hospitalization ward, TLOSHOSP), and length of mechanical ventilation (LMV).
METHODS
After approval from the Ethics Committee of Necker- Enfants Malades University Hospital, Paris, France, under the registration number 2017-CK-5-R1 on March 21, 2017 (Chairperson Professor Mariane de Montalembert) and after declaration of this study to the National Commission of Liberties and Computer Science, Paris, France (CNIL, Commission Nationale des Libertes et de l'Informatique) under the registration number 2028257 v0 on February 21, 2017 (Chairperson Mrs Isabelle Falque-Pierrotin), 193 patients with a median age of 27.5 months (1.0-100.5) (first quartile-third quartile interval) were included in this study from our Hospital, Necker-Enfants Malades, Paris.
Inclusion criteria consisted of patients admitted for abdominal surgery and who received blood products (packed red blood cells [PRBCs] and/or fresh frozen plasma [FFP] and/or concentrated platelet units [CPUs]) in the intraoperative period (transfusion group,) and patients admitted for the same surgical specialty and who did not receive any blood transfusion during surgery or in the post-operative period.
We first included the transfused patients and then patients who did not receive blood components, to include patients with the same surgical operations whenever possible. The local Transfusion Department (EFS, Etablissement Francais de Sang, Hopital Universitaire Necker Enfants Malades) provided a list of patients who had been transfused in the operation theater from January 1, 2014, to December 31, 2016. There were 1500 transfused patients identified of which only 94 were finally retained for the study because of complete data and also to have the same number of patients with equivalent surgical operations as in the no transfusion group.
We used the operation theater programmation system to identify patients who did not receive blood products intraoperatively and post-operatively. We included 99 patients from 1 January 2014, to 17 May 2017 in the no transfusion group. Whenever possible, patients scheduled for similar interventions as in the transfused group were included. Medical records were analyzed using the computer medical report system (Orbis, Mediweb and Cristalnet).
Data collected consisted of intraoperative and post-operative mortality occurring during hospitalization regardless of TLOSHOSP (to assess primary outcome), intraoperative and post-operative complications which included organ failure and infections, repeat surgery, number of days spent in the intensive care unit and in the hospitalization ward, total number of days spent in hospital, and number of days spent under mechanical ventilation (to assess secondary outcome). Factors that could influence primary and secondary outcomes were collected: Age, prematurity, type of surgery, comorbidities, American Society of Anesthesiologists Score (ASA score), emergency surgery, number of units of blood products administered (PRBC units, FFP units, and CPU), pre-operative and post-operative hemoglobin, and platelet levels. The ASA score (I-V) is a scale used in anesthesia to assess patient severity physical status - ASA I: Normal healthy patient, ASA II: Patient with mild systemic disease, ASA III: Patient with severe systemic disease, ASA IV: Patient with severe systemic disease which is constantly threatening life, and ASA V: Moribund patient who is not expected to survive without surgery. Missing data concerning patient weight, intraoperative blood loss and fluid therapy with crystalloids and colloids, and coagulation analysis such as international normalized ratio, activated partial thromboplastin time, and fibrinogen blood levels which could influence blood transfusion were not taken into account since they were not always available. XLSTAT 2018.3 software was used for statistics. Statistical tests included Student's test to compare parametrical variables, Chi-square, or Fischer's exact test to compare category variables. Logistic and log-linear regressions were used for multivariate analysis. Variables are expressed in mean values with standard deviation (±SD) or in median values with the interquartile interval (q1-q3) or in proportions. We considered significant a P = 0.05. We first identified risk factors with univariate analysis. Second, we proceeded with multivariate analysis with logistic and log-linear regressions to access for predictive risk factors [4].
Six risk factors were identified (ASA score, emergency surgery transfusion (units of blood products administered PRBC + FFP + CUP), age, prematurity and type of surgery) and correlated to the number of deaths (mortality) during hospitalization, number of patients with intraoperative and post-operative complications (complications), repeat surgery, number of days spent in the intensive care unit (LOSICU), in the hospitalization ward (LOSHOSP), total number of days spent in hospital (ICU plus hospitalization ward, TLOSHOSP), and the number of days spent under mechanical ventilation (LMV). Hemoglobin and platelet levels were not taken into account for analysis since some of the data was not available.
RESULTS
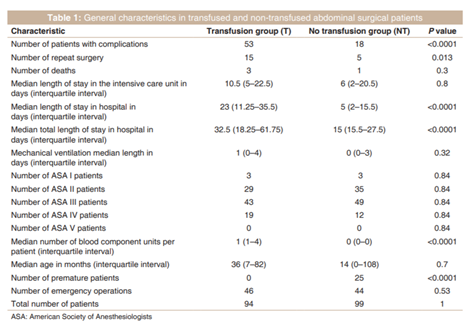
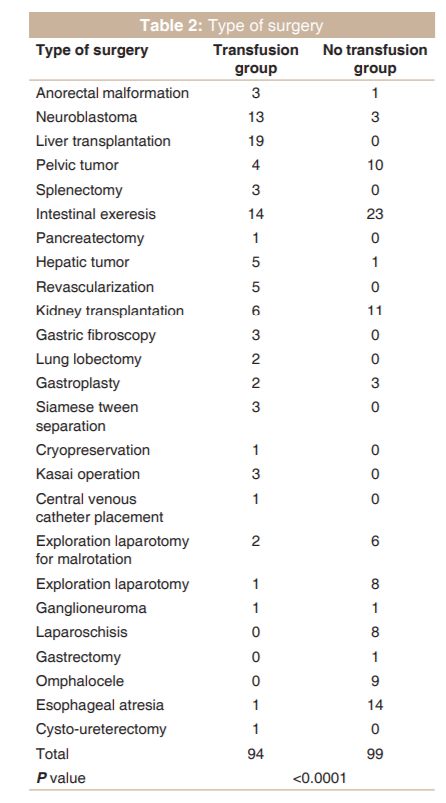
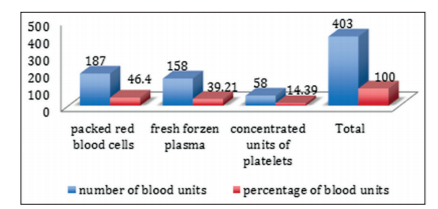
In univariate analysis [Table 1], the number of patients with complications, repeat surgery, median LOSHOS, median TLOSHOSP was significantly higher in the transfusion group. Age, the number of deaths, LOSICU, median LMV, ASA score status, and the number of emergency operations were not different between the two groups. There were 25 premature patients in the no transfusion group, and there were no premature patients in the transfusion group. Table 2 shows the type of surgery. In the transfusion group, the most common surgery was liver transplantation (19 cases over 94 patients), followed by intestinal exeresis (14 patients) and neuroblastoma (13 patients). In the no transfusion group, the most common surgery was intestinal exeresis (23 patients of the 99) followed by esophageal atresia (14 patients) and by kidney transplantation (11 patients). Figure 1 illustrates the blood components administered in the transfusion group. Red blood cells were the most administered blood products (187 units of the 403 units) followed by FFP (158 units) and by platelets (58 units).
Hepatic transplantation and hepatic tumor patients were the most transfused patients with 12.36 ± 2.5 and 12.5 ± 6.73 blood units per patient, respectively, followed by pelvic tumor patients with 6 ± 3.68 blood units per patient [Table 3]. Table 4 illustrates comorbidities, the most important comorbidity was taken into account when a patient had more than one comorbidities. In the transfusion group, the most common comorbidity was hepatic failure (25 cases), followed by cancer (12 patients). In the no transfusion group, the most common comorbidity was cancer (15 patients) followed by prematurity (13 patients), hemorrhagic diathesis (10 patients), and chronic kidney failure (10 patients).
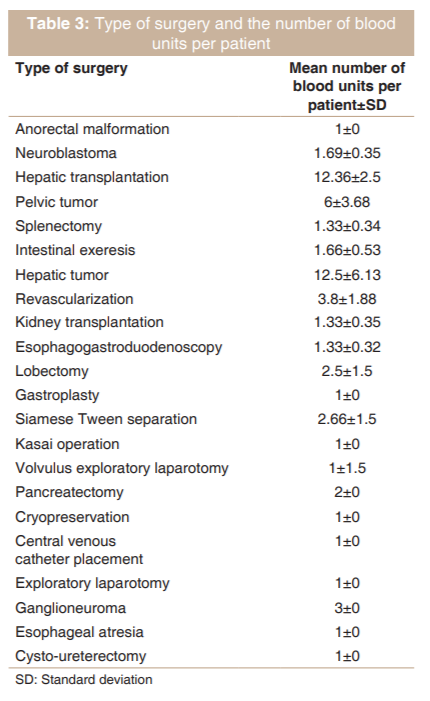
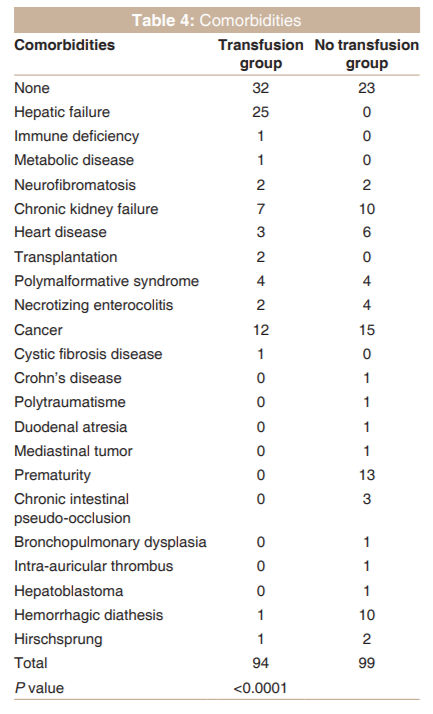
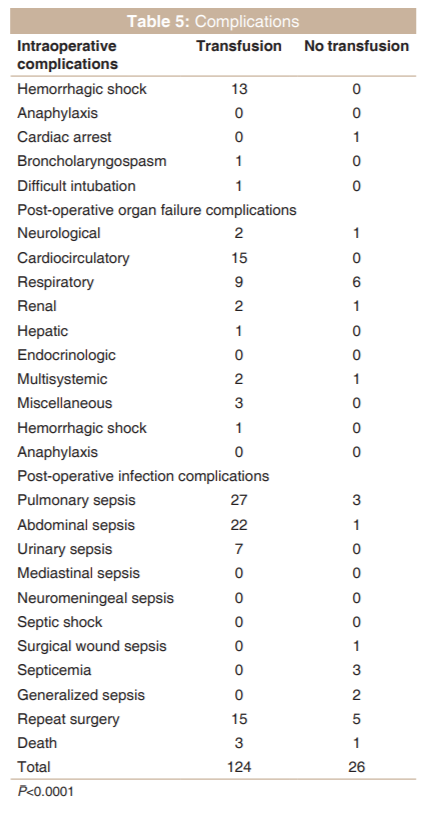
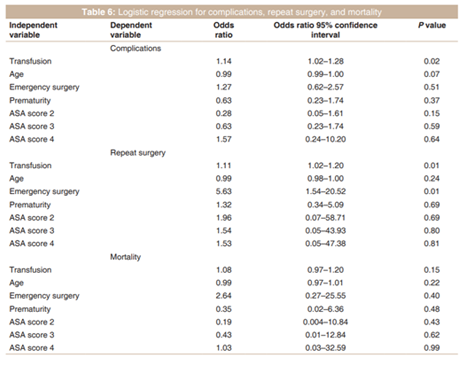
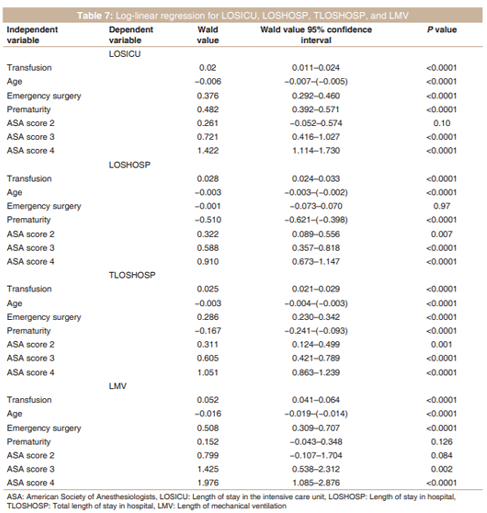
Table 5 shows the number of complications in the two groups. There were significantly more complications in the transfused group. The most intraoperative complication in the transfusion group was hemorrhagic shock (13 patients), the most common post-operative organ failure complication was cardiocirculatory failure (15 patients), followed by respiratory failure (9 patients), and the most common post-operative infection complication was pulmonary sepsis (27 patients) followed by abdominal sepsis (22 patients). After logistic regression, transfusion was the independent predictive risk factor for post-operative complications and an independent predictive risk factor for repeat surgery [Table 6]. Emergency surgery was an independent predictive risk factor for repeat surgery [Table 6]. There was no independent predictive risk factor found for mortality among the explanatory variables analyzed in this cohort [Table 6]. After log-linear regression [Table 7], transfusion, age, prematurity, emergency surgery, and ASA score were independent predictive risk factors for LOSICU and TLOSHOSP. Transfusion, age, emergency surgery, and ASA score were independent predictive risk factors for LMV [Table 7].
DISCUSSION
Our study has shown that in this pediatric retrospective cohort study, perioperative and post-operative morbidity is determined by multiple factors. We focused on some of these factors: Transfusion, ASA score, emergency surgery, age, and prematurity. Studies in pediatric cardiac surgery and critically ill pediatric patients have reported the role of transfusion as an independent morbimortality factor [1-3]. This survey concerned pediatric patients from the intraoperative and the post-operative period to discharge from hospital. There were no significant independent risk factors for mortality in this pediatric abdominal surgical cohort. Transfusion was an independent risk factor for perioperative complications, repeat surgery, LOSICU, LOSHOSP, TLOSHOSP, and LMV. Patients who needed transfusion had more comorbidities and were exposed to hemorrhagic surgery (liver transplantation, hepatic tumor resection, and pelvic tumor resection). Emergency surgery was an independent risk factor for repeat surgery, LOSICU, TLOSHOSP, and LMV. Age and ASA score were independent predictive risk factors for LOSICU, TLOSHOSP, and LMV. Our study highlighted some factors which were only the visible part of the iceberg since perioperative and post-operative morbidity is multifactorial. Other factors that could influence patient outcome such as hemoglobin concentration, weight, fluid therapy with colloids and crystalloids, blood loss, type of anesthesia (all patients had general anesthesia in this study), and organizational aspects were not analyzed here. LOSICU, LOSHOSP, TLOSHOSP, and LMV depend on several factors and those analyzed in our study are far from being exhaustive, but they can help to understand some aspects implicated in morbidity.
Patient outcome can be improved by reducing the above-mentioned morbidity risk factors. Since ASA score was an independent morbidity risk factor in this study, perioperative management of high ASA score patients should be adapted to patient status and surgery. Studies in adult surgery have demonstrated patient outcome improvement in surgical patients when a goal-directed therapy protocol was used intraoperatively [5,6], studies concerning this participant are rare in pediatric surgery [7] and anesthesia, and focus should be directed in developing prospective goal-directed protocol studies in children to demonstrate whether the outcome is upgraded. Optimizing transfusion strategies could improve patient outcome. Studies have reported the physiopathology underlying some transfusion-related complications [8,9]. Exposure to blood products can be reduced by applying restrictive transfusion strategies [10-12], using transfusion protocols based on bedside viscoelastic methods to guide blood components administration during hemorrhagic surgery such as liver transplantation, hepatic tumor resection, and pelvic tumor resection [13,14]. A study in adult liver transplantation demonstrated that ROTEM-guided transfusion protocol reduced intraoperative blood loss, red blood and fresh frozen [13] plasma transfusion, and hospitalization costs [13]. A Cochrane meta-analysis of 17 randomized studies concerning 1493 patients (of which 2 were pediatric cardiac studies with 131 pediatric patients) showed that when viscoelastic methods (ROTEM or TEG) were used in hemorrhagic surgeries in adults (cardiac surgery and liver transplantation), there were a 48% reduction in global mortality, a 14% reduction in red blood cell, 43% reduction in FFP, and 25% reduction in platelet transfusions, a decrease in repeat surgery and a decrease in extrarenal replacement therapy in adult patients. Reduction of mortality was not demonstrated in children and this can be explained by the small number of patients (131 pediatric patients in 2 pediatric studies were concerned) [15].
Larger prospective randomized studies are needed in children to demonstrate that mortality and morbidity can be reduced in high-risk hemorrhagic surgery when point-of-care viscoelastic methods are used to guide transfusion. Emergency surgery is an independent risk factor for morbidity, urgent interventions should be realized during emergency periods, and non-urgent operations realized electively. One study showed that complications are higher in emergency surgery than in elective surgery [16].
Age is also an independent factor for morbidity. A recent prospective multicenter study reported the importance for the management of pediatric patients under a certain age in specialized centers, the importance of a good training, and supervision environment [17]. Our survey analyzed transfusion and morbidity factors in critically ill pediatric patients in abdominal surgery. Not all morbidity risk factors were analyzed in our study but only some of those factors which were accessible and thus analyzable. Identifying morbidity factor is one of the first steps toward patient outcome improvement. Once these factors are identified, preventive measures can be applied.
Our study had limits, it was retrospective, monocenter, and some data concerning factors which could influence outcome was missing. Larger prospective randomized studies are needed to complete retrospective surveys to have recommendations to improve post-operative patient outcome in the pediatric population.
References
- Willemse A, Van Lerberghe C, Gonsette K, De Ville A, Melot C, Hardy JF, et al. The indication for perioperative red blood cell transfusion is a predictive risk factor for severe postoperative morbidity in children undergoing cardiac surgery. Eur J Cardiothorac Surg 2014;45:1050-7.
- Kneyber MC, Hersi MI, Twisk JW, Markhorst DG, Plotz FB. Red blood cell transfusion in critically ill children is independently associated with increased mortlity. Intensive Care Med 2007;33:1414-22.
- Rajasekeran S, Kort E, Hacbarth R, Davis AT, Sanfilippo D, Fitzgerald R, et al. Red cell transfusion as an independent risk for mortality in crtically ill children. J Intensive Care 2016;4:2.
- Melot C. Les analyses multivariables. Rev Mal Respir 2005;22:687-90.
- Calvo-Vecino JM, Ripolles-Melchior J, Mythen MG, Harrison D, Rowan K. Effect of Goal-directed haemodynamic therapy on postoperative complications in low moderate risk surgical patients: A multicentre randomized controlled trial. BJA 2018. DOI: 10.1016/j.bja.2017.12.018.
- Ripolles-Melchior J, de Fuenmayor Varela ML, Criado Camargo S, Jerez Fernandez P. Enhanced recovery after surgey protocol versus conventional perioperative care in colorectal surgey. A single center cohort study. Rev Bras Anestesiol 2018;30:30.
- Rove K, Edney J, Brockel M. Enhanced recovery after surgery in children: Promising evidence-based multidisciplinary care. Pediatr Anaesth 2018;28:482-92.
- El Kenz H, Van der Linden P. Transfusion-related acute lung injury. Eur J Anaesthesiol 2013;30:1-6.
- Mulder HD, Augustijn QJ, van Woensel JB, Bos AP, Juffermans NP, Wosten-van Asperen RM, et al. Incidence, risk factors, and outcome of transfusion-related acute lung injury in critically ill children: A retrospective study. J Crit Care 2015;30:55-9.
- Lacroix J, Hebert PC, Hutchison JS, Hume HA, Tucci M, Ducruet T, et al. Transfusion strategies for patients in pediatric intensive care units. N Engl J Med 2007;356:1609-19.
- Kozek-Langenecker SA, Afshari A, Albaladejo P, Santullano CA, De Robertis E, Filipescu DC, et al. Management of severe perioperative bleeding: Guidelines from the European society of anaesthesiology. Eur J Anaesthesiol 2013;30:270-382.
- Kloesel B, Kovatsis PG, Faraoni D, Young V, Kim HB, Vakili K, et al. Incidence and predictors of massive bleeding in children undergoing liver transplantation: A single-center retrospective analysis. Paediatr Anaesth 2017;27:718-25.
- Smart L, Mumtaz K, Scharpf D, Gray NO, Traetow D, Black S, et al. Rotational thromboelastometry or conventional coagulation tests in liver transplantation: Comparing blood loss, transfusions, and cost. Ann Hepatol 2017;16:916-23.
- Nacoti M, Corbella D, Fazzi F, Rapido F, Bonanomi E. Coagulopathy and transfusion therapy in pediatric liver transplantation. World J Gastroenterol 2016;22:2005-23.
- Wikkelso A, Wetterslev J, Moller AM, Afshari A. Thromboelastography (TEG) or thromboelastometry (ROTEM) to monitor haemostatic treatment versus usual care in adults or children with bleeding. Cochrane Database Syst Rev 2016;3:CD007871.
- de Graaff JC, Sarfo MC, van Wolfswinkel L, van der Werff DB, Schouten AN. Anesthesia-related critical incidents in the perioperative period in children; A proposal for an anesthesia-related reporting system for critical incidents in children. Paediatr Anaesth 2015;25:621-9.
- Habre W, Disma N, Virag K, Becke K, Hansen TG, Johr M, et al. Incidence of severe critical events in paediatric anaesthesia (APRICOT): A prospective multicentre observational study in 261 hospitals in europe. Lancet Respir Med 2017;5:412-25.