A Comparison of Feulgen Stain and Acridine Orange to Stain Micronuclei in Shisha Smokers and Cigarette Smokers
Prathibha Prasad1, Mohamed Said Hamed1, Prashant Nahar2
2.Department of Oral Medicine, Pacific Dental College, Udaipur, Rajasthan, India
Citation : Prasad P, Hamed MS, Nahar P. A Comparison of Feulgen Stain and Acridine Orange to Stain Micronuclei in Shisha Smokers and Cigarette Smokers. J Clin Res Dent 2018;1(1):1-3.
Background: Micronucleus as a biomarker to assess the effects of genotoxicity has been emphasized by several geneticists.
Method: After a brief explanation of the study, and obtaining a written consent signed from the study participants, a questionnaire was administered to collect data. A buccal swab was taken from the subjects. The exfoliated cells were transferred onto 2 glass slides which were immediately fixed using a spray fixative. They were stained by DND specific stains to analyze micronuclei.
Results: Acridine orange appeared to be a much easier and faster way of identifying micronuclei and there was absolutely no confusion with any other nuclear abnormality when compared to Feulgen stain.
Acridine orange stain, feulgen stain, micronuclei,Dentistry
BACKGROUND
Micronuclei (MN) are tiny extranuclear bodies that resemble the daughter nucleus but just smaller in size. They are induced by defects in the DNA repair mechanism, accumulated DNA damages, and chromosomal aberrations. MN as a biomarker to assess the effects of genotoxicity have been emphasized by several geneticists. Various genotoxic agents might induce MN formation which is an indicator of initial stages of genomic instability[1]. As we are aware of the role of genomic instability in cancer, it is of huge significance to understand the role of MN screening in predicting and preventing these diseases. Lifestyle factors like smoking are known to affect the frequency of MN due to its toxins[2]. However, of course, host mechanism sure accounts for interindividual differences. We stained the samples from smokers (shisha and cigarette) with Feulgen and Acridine orange (AO) to screen the MN.
METHODS
The following criteria are included in the study:
1. Cigarette and sheesha smokers exclusively or in combination for more than 5 years and residing in UAE.
2. Control group will comprise non-smokers residing in UAE.
The following criteria are excluded from the study:
1. Sheesha and/or cigarette smokers for < 5 years.
2. Involuntary participation.
A total sample size of 400 was studied. 100 subjects under each category were studied: Exclusively sheesha smokers, exclusively cigarette smokers, cigarette and sheesha smokers, and non-smokers.
After a brief explanation of the study, and obtaining a written consent signed from the study participants, a questionnaire was administered to collect data. A detailed case history was taken followed by a clinical examination. A buccal swab was taken from the subjects. The exfoliated cells were transferred onto two glass slides which were immediately fixed using a spray fixative. Several researchers have shown practical ways of collecting the samples in their study. According to them, placing smear directly on the slide with two drops of saline gives a better spread of cells than washing them. Alcohol is proven to keep the cells intact until staining (Stitch et al., 1992; Burgaz et al., 1999; Lucero et al., 2000; and Cavallo et al., 2005) which might or might not depend on the stain used. The slide was then fixed using Biofix spray fixative and was allowed to dry to stain later[3]. These slides were later stained by Feulgen stain and AO to examine the MN.
The MNs assay being a valid and sensitive, yet a very simple technique was adopted as a biomarker of the genotoxicity/ genetic damage. The exfoliated cells of oral mucosa not only come in direct contact with the carcinogenic substances in the smoke but the systemic effects of the smoke will also be surely exhibited by these cells[4-7]. Slides stained by Feulgen stain were observed under compound light microscope for MN. Slides stained by AO stain were examined under the fluorescent microscope which highlights the MN. This was done to rule out other secondary nuclear deformities[8]. MN either originates from fragments of chromosome or whole chromosomes which are not included in the main daughter nuclei during nuclear division. Thus, MN assay provides us a measure of chromosome loss and chromosome breakage. It has been documented to be as sensitive as classical metaphase chromosomal analysis in serving as an indicator of chromosome damage. MN frequency was checked in 1000 cells[9,10].
RESULTS AND DISCUSSION
The MNs assay was adopted as a biomarker of the genotoxicity/ genetic damage. It is a valid and sensitive technique yet very simple. Studies carried out in several countries (Armenia, Georgia, Ukraine, and Russia) have listed the rules to be followed for MNs assay listed by Tolbert et al. Since there are many interinstitutional discrepancies in the method followed, this uniformity will ensure comparisons between the studies are valid. Our study followed them:
1. We stained the exfoliated cells collected after the history of exposure with two of the DNA-specific stains among the three given which were Feulgen and acridine range to exclude the artifacts and count MN
2. Intact cytoplasm
3. Intact nuclei with distinct and smooth perimeter
4. MN must be =1/3 the diameter of the main nucleus or less, must share the same focal plane and staining with similar texture as main nucleus
5. The total number of MN per 1000 cells was counted[11,12].
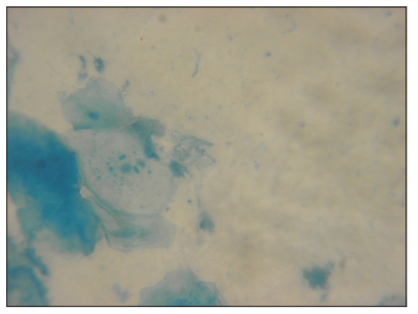
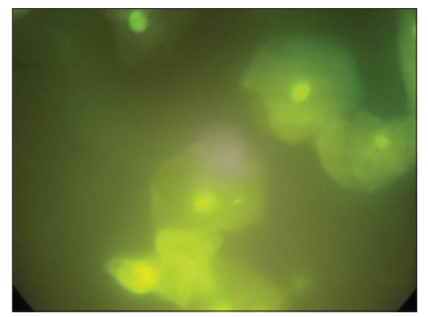
MN frequency more than 1-3 per 1000 cells was seen in smokers in a healthy population. The exfoliated cells of oral mucosa not only come in direct contact with the carcinogenic substances in the smoke but also exhibit the features due to systemic effects of the smoke. Mean MN in Feulgen was highest for sheesha + cigarette group and least for control group. Similarly, mean MN in AO was highest for sheesha + cigarette group and least for control group. This difference in mean MN in Feulgen and AO was statistically significant. With respect to MN in Feulgen [Figure 1], majority of subjects in sheesha (57%) and in cigarette group (58%) had MN of 4-12, majority in sheesha + cigarette group (71%) had MN of >12, and majority in control group had MN of 0-3. This observation was statistically significant between four groups. With respect to MN in AO, majority of subjects in sheesha (59%) and in cigarette group (60%) had MN of 4-12, majority in sheesha + cigarette group (51%) had MN of >12, and 100% in control group had MN of 0-3 [Figure 2]. This observation was statistically significant between four groups.
This proves that sheesha/hookah/WTS is as dangerous if not more dangerous than cigarette smoking, and it is exceptionally dreadful to have a habit of smoking both cigarette and sheesha.
For staining nuclei, MN, and any nuclear anomalies in oral exfoliated cells, DNA-specific stains are preferred. Misreading nuclear anomalies such as karyorrhexis, karyolysis, condensed chromatin, and binucleates as MN are higher in DNA non-specific stains. Studies reported increased false-positive results with Giemsa stain due to secondary nuclear abnormalities, keratohyalin granules and even bacteria can lead to misinterpretation. We used DNA-specific stains in our study and got good results. There was not much difficulty in distinguishing MN and other nuclear abnormalities. Ayyad et al. compared Giemsa stain and PAP stain for analyzing MN in exfoliated oral epithelial cells and concluded PAP was a better staining method[13].
According to Neresyan et al., stains which are not DNA specific leads to overestimates. AO which is DNA specific is generally used for observations with fluorescence microscopy, thereby avoiding errors introduced through counting artifacts (Lucero et al., Pastor et al., and Cavallo et al.,) which were used in our study[11]. We used AO which is a DNA-specific stain and when observed under fluorescent microscopy, MN appears very distinct and fluorescent[2]. This led to the least error in counting MN when compared to Feulgen stain. It was also a much faster method to count MN when compared to Feulgen stain as there was no way of missing the fluorescent MN, and there was absolutely no confusion with any other nuclear abnormality. Metgud studied exfoliated buccal mucosal cells of smokers and found that the mean MN score with DNA non-specific stain (Giemsa) was significantly higher and no such difference was seen in DNA-specific stains used (AO and Feulgen) in smokers. They concluded that staining procedures and duration of smoking affect the MN count[14].
CONCLUSION
Our study proves that AO could be the stain of choice for counting MN which ensures sensitivity and specificity, especially when the protocol has been followed to the T.
REFERENCES
- Luzhna L, Kathiria P, Kovalchuk O. Micronuclei in genotoxicity assessment: From genetics to epigenetics and beyond. Front Genet 2013;4:131.
- Bolt HM, Stewart JD, Hengstler JG. A comprehensive review about micronuclei: Mechanisms of formation and practical aspects in genotoxicity testing. Arch Toxicol 2011;85:861-2.
- Stich HF, Rosin MP. Micronuclei in exfoliated human cells as a tool for studies in cancer risk and cancer intervention. Cancer Lett 1984;22:241-53.
- Rosin MP. Antigenotoxic activity of carotenoids in carcinogen-exposed populations. Basic Life Sci 1990;52:45-59.
- Rosin MP. Genetic and proliferation markers in clinical studies of the premalignant process. Cancer Bull (Houston) 1991;43:507-14.
- Tucker JD, Preston RJ. Chromosome aberrations, micronuclei, aneuploidy, sister chromatid exchanges, and cancer risk assessment. Mutat Res 1996;365:147-59.
- Miller B, Albertini S, Locher F, Thybaud V, Lorge E. Comparative evaluation of the in vitro micronucleus test and the in vitro chromosome aberration test: Industrial experience. Mutat Res 1997;392:45-59, 187-208.
- Nersesyan A, Kundi M, Atefie K, Schulte-Hermann R, Knasmuller S. Effect of staining procedures on the results of micronucleus assays with exfoliated oral mucosa cells. Cancer Epidemiol Biomarkers Prev 2006;15:1835-40.
- Kirsch-Volders M. Towards a validation of the micronucleus test. Mutat Res 1997;392:1-4.
- Evans HJ. Historical perspectives on the development of the in vitro micronucleus test: A personal view. Mutat Res 1997;392:5-10.
- Nersesyan AK, Ilin AI. The micronucleus assay in exfoliated human cells: A mini-review of papers from the CIS. Tsitol Genet 2007;41:56-66.
- Agarwal M, Balaji N, Sumathi MK, Sunitha JD, Dawar G, Rallan NS. Micronuclei assay of exfoliated oral mucosal cells: A review. Ann Dent Spec 2013;1:1-3.
- Khanna S, Purwar A, Singh NN, Sreedhar G, Singh S, Bhalla S. Cytogenetic biomonitoring of premalignant and malignant oral lesions by micronuclei assessment: A screening evaluation. Eur J Gen Dent 2014;3:46-52.
- Metgud R, Neelesh BT. Effect of staining procedures on the results of micronucleus assay in the exfoliated buccal mucosal cells of smokers and nonsmokers: A pilot study. J Can Res Ther 2018;14:372-6.