Mixed Benign Ovarian Neoplasms: A Report of Five Cases
Chrisostomos Sofoudis1, D. Vassiliadou1, G. Georgoulias1, E. Papamargaritis1, A. Gerolymatos1
Citation : Chrisostomos Sofoudis, D. Vassiliadou, et.al, Mixed Benign Ovarian Neoplasms: A Report of Five Cases Journal of Clinical Research in Oncology 2018; 1(1): 1-7.
Benign ovarian cystic neoplasms quite unusually present with mixed histomorphology, exhibiting features of several histopathologic types. The purpose of this study is to report on five such cases who were treated at our center.
Over a period of 2 years (2015-2017), five women who underwent surgery for ovarian cysts were found to have a mixed benign neoplasm.
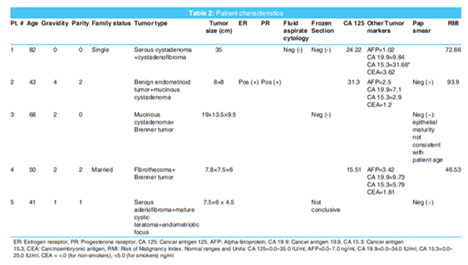
The mean age of our patients was 56.8 years. Two of them were postmenopausal, and three were premenopausal. Four patients were gravid (max gravidity = 4). Two patients presented with acute symptomatology while three of them underwent elective surgery. Tumor types per patient are presented in the table. Mean tumor dmax was 15.5 cm, and the median was 8 cm. All patients with available data composed of a normal cancer antigen 125 value leading to a risk of malignancy index that ranged from 46.53 to 93.9, with a mean of 71.03.
Mixed benign neoplasms are an uncommon histopathologic finding in patients undergoing surgery for ovarian cysts.
Benign, mixed, ovarian neoplasms.
INTRODUCTION
Ovarian masses consistof the most commonpresentations in general gynecology and are mostly cystic. Women have a 5-10% lifetime risk of developing a suspicious adnexal mass that requires surgery [1]. Ovarian cysts can be classified either as actual ovarian cystic neoplasms or as functional ovarian cysts (deriving from a disruption in normal ovulation). Ovarian cystic neoplasms are distinguished histologically depending on their cell type of origin and are grouped as epithelial tumors, germ cell tumors, sex cord-stromal tumors, and others [Table 1] [2]. Elaboration on functional cysts and ovarian malignancy is beyond the scope of this article.
Among benign ovarian neoplasms, serous and mucinous cystadenomas and mature cystic teratoma are the most common [3]. Epithelial tumors account for approximately 60-80% of all true ovarian neoplasms; serous tumors are responsible for approximately 30% and mucinous tumors for approximately 10-20% of all epithelial ovarian neoplasms. Brenner tumors account for 1-2% of primary ovarian tumors, of which more than 98% are benign. Regarding sex cordstromal tumors, the comas account for only 2% of all ovarian tumors. Mature cystic teratomas are responsible for 40-50% of all benign ovarian neoplasms [4].
Most patients with ovarian cysts are asymptomatic, with the cysts being discovered accidentally during ultrasonography. However, some patients may develop symptoms, ranging from mild abdominal discomfort, constipation, abdominal fullness, and indigestion to a more severe presentation with acute abdominal pain, even tachycardia, and hypotension when the cyst is complicated by torsion or rupture. Transvaginal ultrasound is the preferred imaging modality for the evaluation of adnexal masses [5-7]. Serum marker testing may be helpful in assessing the malignancy risk. Cancer antigen 125 (CA 125) has been the most extensively studied and the most useful so far [5]. Management of ovarian cysts depends on patient age, menopausal status, imaging features of the cyst and tumor marker values. We present a series of five patients who underwent surgical dissection for an ovarian cyst and were found to have a benign ovarian neoplasm of mixed histology.
MATERIALS AND METHODS
This is a retrospective study of patients who underwent surgery for cystic ovarian masses over a period of 2 years in a tertiary center. Five patients were reported to have a mixed benign ovarian neoplasm on histology. All patients were operated on by the same surgical team. Consent was obtained from all patients, and the study was approved by the hospital's Ethics Committee.
RESULTS
Our results are presented in Table 2. The mean age of our patients was 56.8 years. Two of them were postmenopausal, and three were premenopausal. Four patients were gravid (max gravidity = 4). Two patients presented with acute symptomatology while three of them underwent elective surgery. Tumor types per patient are presented in the table. Mean tumor dmax (maximum diameter) was 15.5 cm and the median was 8 cm. All patients with available data had a normal CA 125 value, leading to a risk of malignancy index (RMI) that ranged from 46.53 to 93.9, with a mean of 71.03.
Two of our patients are described here more extensively.
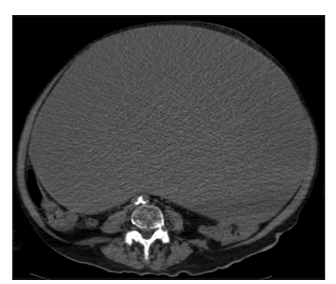
Patient #1, aged 82, gravida 0 para 0, presented at the emergency department, complaining of dyspnea, abdominal discomfort, and progressively increasing abdominal girth over the past 3 years. On admission, the patient was found to have tense ascites and underwent a diagnostic and therapeutic paracentesis, which yielded 1.3 L of fluid initially, reaching 7.5 L over the first 3 days of hospitalization. Imaging denoted, besides the ascitic collection, a cystic mass deriving from the right ovary, of dmax = 33 cm, occupying the whole of the abdominal cavity [Figure 1]. Under CT guidance, a fine needle aspiration was performed. The peritoneal fluid was sent for cytopathologic evaluation. The cytological report revealed no signs of malignancy. Tumor markers were within normal limits, except a marginal increase in the CA 15.3 value (31.66 with an upper normal value of 25.0). The patient's RMI score was 72.66. The patient underwent a subtotal abdominal hysterectomy and bilateral salpingooophorectomy. Intraoperative frozen section was negative for malignancy. Due to advanced age and medical comorbidities, the patient was admitted to the ICU for post-operative monitoring for 24 h and had an uneventful post-operative course. In the final histology report, the cyst was found to have a maximum diameter of 35 cm, was unilocular and filled with brown fluid. It also contained a solid component sized 5.5 × 4.5 × 3 cm. Microscopic examination identified the neoplasm as a mixed serous cystadenoma and cystadenofibroma.
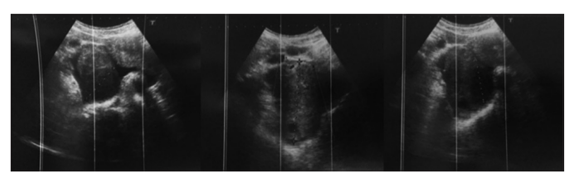
Patient #4, aged 50, gravida 2 para 2, presented at the emergency department with acute abdominal pain, especially located in the right lower quadrant. Laboratory findings were not significant, besides a mild leukocytosis. Ultrasound report was as follows: "The right adnexa appears enlarged, with a longitudinal axis of 8 cm. A wellcircumscribed cystic formation with multiple echogenic foci is noted, with a diameter of 4 cm as well as the presence of adjacent fluid. These findings are consistent with adnexal torsion" [Figure 2]. Indeed, the patient was immediately led to surgery and underwent a right salpingo-oophorectomy and the left ovary was biopsied. The patient had a prompt and uneventful recovery. Tumor markers were within normal limits and the RMI score was 46.53. The histology report of the biopsy specimen from the left ovary was negative for malignancy. Regarding the right ovary, macroscopically the neoplasm comprised a mainly solid component of white color and elastic composition, including some cysts, the larger of which had a diameter of 2 cm. Moreover, a smaller nodule was noted, situated at the ovarian hilum, of similar macroscopic features. Microscopically, it was identified that the mass actually contained two separate neoplasms, the one being a cell abundant fibrothecoma without cellular atypia and <3 mitoses/10 HPF and the other being a Brenner tumor.
DISCUSSION
When an ovarian cyst is diagnosed, a thorough medical history should be obtained, with specific attention to risk factors, protective factors and an assiduous family history of ovarian or breast cancer. The potential of pregnancy is among the first that should be evaluated in all women of reproductive age presenting with an adnexal mass. Progressively worsening unilateral pain may be due to adnexal torsion, while dysmenorrhea and dyspareunia can be attributed to an endometrioma. Special attention should be given to symptoms suggestive of malignancy, such as persistent abdominal distention, early satiety, cachexia, and increased urinary frequency. Physical examination should include abdominal and pelvic examination, as well as palpation for local lymphadenopathy.
Tumor marker testing is a helpful modality in the management decision. CA 125 has been so far the most widely used marker associated with epithelial ovarian malignancies. However, CA 125 levels may also be elevated in other malignancies, as well as in benign and physiologic conditions. Such malignant conditions include, besides epithelial ovarian carcinoma: Endometrial carcinoma, endocervical adenocarcinoma, pancreatic carcinoma, breast carcinoma, lymphoma, lung carcinoma, colorectal carcinoma, and squamous cervical or vaginal carcinoma. Benign conditions with an elevated CA 125 value include: Endometriosis, cirrhosis, acute peritonitis, acute pancreatitis, acute pelvic inflammatory disease, first trimester of pregnancy, as well as a small percentage of healthy individuals [8]. If a cutoff of 30 IU/ml is used, the test has a sensitivity of 81% and specificity of 75% [9]. While the American College of Obstetricians and Gynecologists suggests the measurement of levels of beta - human chorionic gonadotrophin, lactate dehydrogenase, alpha-fetoprotein or inhibin if a less common ovarian histopathology is suspected,[5] the Royal College of Obstetricians and Gynecologists stipulates that neither these markers nor human epididymis protein 4 (HE4), carcinoembryonic antigen, CDX2, cancer antigen 72-4 (CA72-4), and cancer antigen 19-9 (CA19-9) should be routinely employed to assess the risk of malignancy [7].
Transvaginal ultrasound is the most commonly used imaging modality for the evaluation of pelvic masses. The ultrasound examination should provide information about the size andcomposition of the mass (cystic, solid, or mixed), about its laterality and about the presence or absence of septations, mural nodules, papillary excrescences, or free fluid in the pelvis. Doppler ultrasonography is useful to evaluate the vascular features of the lesion;[5] however, it should not be used routinely to differentiate benign from malignant ovarian cysts, as their use has not been associated with significant improvement in diagnostic accuracy [7]. Computed tomography and magnetic resonance imaging are not recommended in the initial evaluation of adnexal masses [5], but should be employed in the assessment of more complex lesions. The society of radiologists in ultrasound concluded that asymptomatic simple cysts 3-5 cm in diameter do not require to follow-up, cysts 5-7 cm require to follow-up, and cysts more than 7 cm in diameter should be considered for either further imaging or surgical intervention [10].
The RMI was first described by Jacobs in 1990 [9], and it still remains the most widely used model. The RMI menopausal status to calculate a score: RMI = U × M × CA125; U = 0 (for ultrasound score of 0); U = 1 (for ultrasound score of 1); and U = 3 (for ultrasound score of 2-5). Ultrasound scans are scored one point for each of the following characteristics: Multilocular cyst, evidence of solid areas, evidence of metastases, presence of ascites, and bilateral lesions. The menopausal status (M) is scored as 1 = premenopausal and 3 = postmenopausal. CA125 is serum CA125 measurement in IU/ml. The RMI has proven to be the most effective index in diagnosing ovarian malignancy. The pooled sensitivity and specificity in the prediction of ovarian malignancies were 78% and 87%, respectively, for an RMI cutoff of 200 [11].
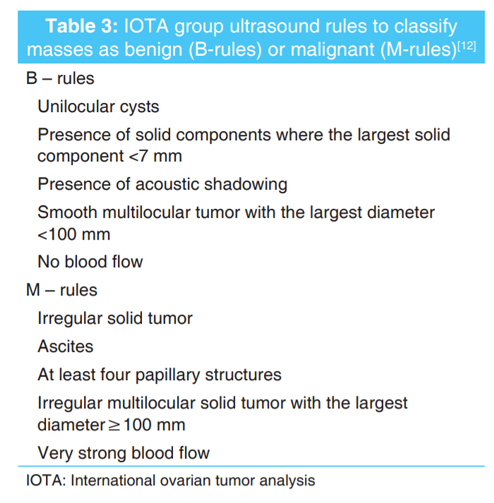
Other ways to predict malignancy include the international ovarian tumor analysis (IOTA) rules, OVA1 and risk of malignancy algorithm (ROMA). The IOTA Group has issued simple ultrasound rules that differentiate benign (B-rules) and malignant (M-rules) ovarian masses [Table 3]. The reported sensitivity of these rules is 95% and specificity 91% [12]. OVA1 is a quantitative assay measuring five serum proteins (CA 125, transthyretin, Apolipoprotein A1, beta-2-microglobulin, and transferrin) and combining them into a numerical score (range 0-10). A value higher than 4.4 is indicative of a high risk of malignancy in postmenopausal women. Although OVA1 has a high sensitivity, it shows a lower specificity and positive predictive value than the RMI [7,13]. ROMA is a quantitative test using CA125, HE4 concentration, and menopausal status to calculate the risk of ovarian cancer. A numerical score is obtained based on an algorithmic equation calculation, with a cutoff value of 2.27 representing a high risk of malignancy. Overall, it has a sensitivity of 89% and a specificity of 75% [7,14].
Ovarian cyst aspiration for diagnostic purposes is usually avoided, because of possible intraperitoneal dissemination of malignancy.
In reproductive age women, many ovarian cysts can be managed conservatively. Functional or simple ovarian cysts (thin-walled cysts without internal structures) which are <5 cm in diameter usually regress over two or three menstrual cycles without intervention. However, ovarian cysts that persist or increase in size are unlikely to be functional and may warrant surgical management [6]. In the premenopausalpatient, the risk of a symptomatic ovarian cyst being malignant is 1 in 1000 [15]. Age is the most important independent risk factor for ovarian malignancy, with its incidence increasing significantly after menopause [16]. Although most adnexal masses in postmenopausal women are benign, the risk of malignancy is greater than in premenopausal women.[17] Under certain circumstances, even postmenopausal women can be managed expectantly: (1) Sonographic evidence of a thin-walled, unilocular cyst, (2) cyst diameter <5 cm, (3) no cyst enlargement during surveillance, and (4) normal CA 125 level [18]. A repeat evaluation should be performed at 4 to 6 months [7].
Cysts presumed to be benign can be excised, or the whole ovary may be removed. The decision for the appropriate management depends on the size of the cyst, patient's age, wish for fertility preservation, and intraoperative findings. Accordingly, laparoscopy is the appropriate route when benign disease is suspected, while larger cysts with a higher risk of malignancy are best to be managed by laparotomy, through a midline vertical incision. According to the Royal College of Obstetricians and Gynecologists, postmenopausal women with a RMI score of <200 are suitable for laparoscopic management. Operation of choice in postmenopausal women is bilateral salpingooophorectomy rather than cystectomy [7].
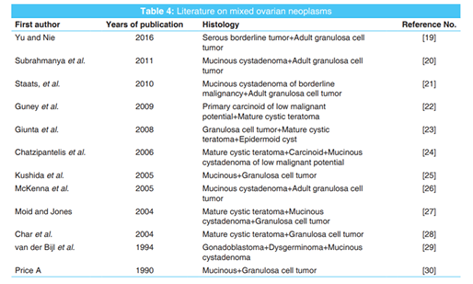
There have been so far only a few reports of mixed ovarian neoplasms in the literature and are presented in Table 4.
The authors declare that there are no conflicts of interest regarding the publication of this article.
CONCLUSION
Mixed benign neoplasms are an uncommon histopathologic finding in patients undergoing surgery for ovarian cysts. As with all ovarian neoplasms, careful pre-operative assessment should be undertaken, to exclude the possibility of malignancy. Transvaginal ultrasound and CA 125 value are the most significant indices that influence the decision for conservative or operative management.
REFERENCES
- American College of Obstetricians and Gynecologists. ACOG practice bulletin. Management of adnexal masses. Obstet Gynecol 2007;110:201-14.
- World Health Organization. In: Kurman RJ, editor. WHO Classification of Tumours of Female Reproductive Organs. 4th ed. Lyon: Agency for Research on Cancer; 2014.
- Pantoja E, Noy MA, Axtmayer RW. Complications of dermoid tumors of the ovary. Obstet Gynecol 1975;45:89-94.
- Tzadik M, Purcell K, Wheeler JE. Benign disorders of the ovaries and oviducts. In: De Cherney A, Nathan L, editors. Current Diagnosis and Treatment Obstetrics and Gynecology. 10th ed. New York: McGraw-Hill Companies, Incorporated; 2006.p. 654-60.
- American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 174: Evaluation and Management of Adnexal Masses. Obstet Gynecol 2016;128:e210-26.
- Royal College of Obstetricians and Gynaecologists. Management of Suspected Ovarian Masses in Premenopausal Women (Green-top Guideline No. 62); 2011.
- Royal College of Obstetricians and Gynaecologists, Ovarian Cysts in Postmenopausal Women (Green - Top Guideline No. 34); 2016.
- King GG, Leighton JC, Staros EB. CA 125, Medscape Laboratory Medicine; 2015. Available from: http://www. emedicine.medscape.com/article/2087557-overview#a2.
- Jacobs I, Oram D, Fairbanks J, Turner J, Frost C, Grudzinskas JG, et al. A risk of malignancy index incorporating CA 125, ultrasound and menopausal status for the accurate preoperative diagnosis of ovarian cancer. Br J Obstet Gynaecol 1990;97:922-9.
- Levine D, Brown DL, Andreotti RF, Benacerraf B, Benson CB, Brewster WR, et al. Management of asymptomatic ovarian and other adnexal cysts imaged at US: Society of radiologists in ultrasound consensus conference statement. Radiology 2010;256:943-54.
- Geomini P, Kruitwagen R, Bremer GL, Cnossen J, Mol BW. The accuracy of risk scores in predicting ovarian malignancy: A systematic review. Obstet Gynecol 2009;113:384-94.
- Timmerman D, Ameye L, Fischerova D, Epstein E, Melis GB, Guerriero S, et al. Simple ultrasound rules to distinguish between benign and malignant adnexal masses before surgery: Prospective validation by IOTA group. BMJ 2010;341:c6839.
- Fung ET. A recipe for proteomics diagnostic test development: The OVA1 test, from biomarker discovery to FDA clearance. Clin Chem 2010;56:327-9.
- Moore RG, Brown AK, Miller MC, Skates S, Allard WJ, Verch T, et al. A novel multiple marker bioassay utilizing HE4 and CA125 for the prediction of ovarian cancer in patients with a pelvic mass. Gynecol Oncol 2009;112:40-6.
- Farahani L, Datta S. Benign ovarian cysts. Obstet Gynaecol Reprod Med 2016;26:271-5.
- Howlader N, Krapcho M, Miller D, Brest A, Yu M, Ruhl J, et al. SEER Cancer Statistics Review, 1975-2013, Based on November 2015 SEER Data Submission, Posted to the SEER Web Site. Bethesda, MD: NCI; 2016.
- Kinkel K, Lu Y, Mehdizade A, Pelte MF, Hricak H. Indeterminate ovarian mass at US: Incremental value of second imaging test for characterization--meta-analysis and Bayesian analysis. Radiology 2005;236:85-94.
- Nardo LG, Kroon ND, Reginald PW. Persistent unilocular ovarian cysts in a general population of postmenopausal women: Is there a place for expectant management? Obstet Gynecol 2003;102:589-93.
- Yu J, Nie X. Composite serous borderline tumor and adult granulosa cell tumor-like area: Is it a true neoplastic AGCT or tumor-like proliferation? Int J Gynecol Pathol 2016;35:25-9.
- Subrahmanya NB, Kapadi SN, Junaid TA. Mucinous cystadenoma coexisting with adult granulosa cell tumor in the ovary: Is it a composite tumor or heterologous mucinous elements in a granulosa cell tumor? Int J Gynecol Pathol 2011;30:386-90.
- Staats PN, Coutts MA, Young RH. Primary ovarian mucinous cystic tumor with prominent theca cell proliferation and focal granulosa cell tumor in its stroma: Case report, literature review, and comparison with Sertoli-Leydig cell tumor with heterologous elements. Int J Gynecol Pathol 2010;29:228-33.
- Guney N, Sayilgan T, Derin D, Ozcan D. Primary carcinoid tumor arising in a mature cystic teratoma of the ovary: A case report. Eur J Gynaecol Oncol 2009;30:223-5.
- Giunta P, Patriarca C, Crepaldi E. Cystic mature teratoma and epidermoid cyst associated with granulosa cell tumour: A rare ovarian scenario. Two case reports and review of the literature. Pathologica 2008;100:485-8.
- Chatzipantelis P, Mavrogiorgis A, Kairi-Vassilatou E, Pafiti A. Ovarian neoplasm composed of an insular carcinoid tumor and a borderline mucinous cystadenoma arising in a mature cystic teratoma: A case report. Eur J Gynaecol Oncol 2006;27:636-7.
- Kushida Y, Haba R, Kadota K, Doi T, Ishikawa M, Hirakawa E, et al. Composite mucinous and granulosa cell tumor of the ovary. Pathol Int 2005;55:797-801.
- McKenna M, Kenny B, Dorman G, McCluggage WG. Combined adult granulosa cell tumor and mucinous cystadenoma of the ovary: Granulosa cell tumor with heterologous mucinous elements. Int J Gynecol Pathol 2005;24:224-7.
- Moid FY, Jones RV. Granulosa cell tumor and mucinous cystadenoma arising in a mature cystic teratoma of the ovary: A unique case report and review of literature. Ann Diagn Pathol 2004;8:96-101.
- Char G, Ramjit C, Fletcher H, Harvey W. Granulosa cell tumour of the ovary with bilateral mature cystic teratomas. A case report. West Indian Med J 2004;53:135-7.
- van der Bijl AE, Fleuren GJ, Kenter GG, de Jong D. Unique combination of an ovarian gonadoblastoma, dysgerminoma, and mucinous cystadenoma in a patient with Turner's syndrome: A cytogenetic and molecular analysis. Int J Gynecol Pathol 1994;13:267-72.
- Price A, Russell P, Elliott P. Composite mucinous and granulosacell tumor of ovary: Case report of a unique neoplasm. Int J Gynecol Pathol 1990;9:372-8.