Use of Simulation- based Training for Cancer Education among Nigerian Clinicians
Kelechi Eguzo1, Chinenye Okwuosa2, Uwemedimbuk Ekanem3, Christie Akwaowo3, Enobong Mkpang4
2.Breast Without Spot, 4 Chime Avenue, Enugu, Nigeria.
3.Department of Community Health, University of Uyo Teaching Hospital,Uyo, Nigeria.
4.Department of Obstetrics and Gynecology, University of Uyo Teaching Hospital, Uyo, Nigeria.
Citation :Eguzo K, Okwuosa C, Ekanem U, Akwaowo C, Mkpang E. Use of Simulation-Based Training for Cancer Education among Nigerian Clinicians. J Clin Res Oncol 2018;1(2):1-6.
Among the many limitations of cancer control in Nigeria are lower awareness/competence and poorer training of health-care professionals (HCP). These manifest as deficiencies in advocacy, screening/diagnostic practices, and patient management. Medical simulation (MS) using models is an effective approach for sustainably improving the competence of HCP, especially regarding clinical breast examination (CBE), pelvic examination (PE), and digital rectal examination (DRE). The study evaluates the effect of MS during a Nigerian training course focusing on CBE, PE, and DRE. It answers the question: What is the immediate outcome of MS-based training, as well as the perspectives of HCP on the use of MS for cancer education?
Participants included a convenience sample of Nigerian physicians and nurses who attended the American Society of Clinical Oncology- sponsored Multidisciplinary Cancer Management Course. The intervention was MS using high-fidelity models. The models demonstrated normal anatomic and common pathologic features of the breast, cervical, and prostate. Participants cycled through MS stations (i.e., CBE, PE, and DRE). Pre- and post-training surveys with comments evaluating self- reported comfort levels were the basis for comparison. Data analysis included descriptive statistics, Wilcoxon signed-rank test, Chi-square, and thematic analysis.
A total of 51 participants completed course evaluation forms (physicians - 35 and nurses - 16), with an average number of years in practice as 8 (±5.2) years. Pre-training survey showed non-significant differences in practices patterns; 71% (22/35) of physicians rarely performed PE (P=0.92), and 93% (14/16) of nurses rarely performed DRE (P=0.07). According to some participants, "the use of simulation is quite commendable as it gives room for improvement before using a human; it is the best method of learning I have ever enjoyed."
MS-based training significantly improved the comfort levels of participants regarding CBE and PE, as well as their likelihood to perform CBE, PE, and DRE. Participants recommend widespread use of MS for continuing medical education and undergraduate training.
Medical education, medical oncology, multimedia, Nigeria, primary health care.
INTRODUCTION
Cancer-related morbidity and mortality are rising in Nigeria, largely due to improved survival from infectious diseases, increasing life expectancy, as well as rise in risk factors such as cigarette smoking, physical inactivity, and obesity [1-3]. Common cancers in Nigeria include breast, cervical, prostate, and colorectal cancers [1,2]. One of the challenges affecting the control of cancers is the relatively low awareness/competence and inadequate training of health-care professionals (HCP) in Nigeria about the disease spectrum [4-6]. Other challenges facing cancer control and Nigeria includes limited access to, and costs associated with screening mammography, Pap screening, and colon cancer screening. The inadequate competence manifests in deficient advocacy/screening practices,[7] poorer patient management outcomes,[8] and other aspects of cancer care. The need to improve the skills of HCP regarding cancers diagnosis and management has been well documented [2,4,5,7,9-11].
Mean while, simulation has been demonstrated as a reliable and sustainable approach for improving the competence of HCP. It has become an integral component of modern undergraduate, postgraduate, and continuing medical education curricula, especially in developed countries [12,13]. Medical simulations, essentially seek to imitate clinical tasks, anatomic regions or real patients, and/or to mimic the real-life circumstances in which medical services are rendered. They are valuable and necessary adjuncts to the educational experience because opportunities to learn essential clinical skills in the real patients or clinical settings setting may be insufficient. Dilaveri et al.[14]. reviewed the use of simulation training for breast and pelvic examinations (PE). They found that compared to no intervention, breast and PE simulation training was associated with moderate to large effects for skills outcomes. Breast and PE, whether performed for screening or diagnostic purposes, are important components of the general physical examination. Clinical breast examination (CBE) is often the method detecting of breast cancer in Nigeria. Similarly, PE remains an integral part of the physical diagnosis for women with vulvar, vaginal, and lower abdominal conditions. The same is applicable for digital rectal examination (DRE), given its role in the diagnosis of rectal and prostate pathologies. These are intimate examinations, which can often be challenging to master. Thus, they need to be practiced in non-clinical settings to be performed well. Although many international organizations do not support clinical or self-breast examination as diagnostic approaches, these steps are still very relevant in resource-limited settings.
Despite the benefits of simulation training, this approach in medical education has not been well developed nor utilized in Nigeria. This article describes the use and evaluation of simulation-based training on breast, pelvic, and DRE. The simulation sessions were part of the Multidisciplinary Cancer Management Course (MCMC) organized by American Society of Clinical Oncology (ASCO) and Medical Women's Association of Nigeria Akwa Ibom State (MWAN-AKS) Branch.
METHODS
The MCMC was a 3-day (March 14-17, 2017) continuing education event. It was aimed at improving the knowledge and competence of health-care providers in AKS regarding cancer screening, diagnosis, and management. The emphasis was on multidisciplinary collaboration. It built on the progress made during the Cancer Control in Primary Care course, which was previously reported [4,11]. In addition to the simulation-training, the course included didactic lectures and interactive activities. The course focused on breast, cervical, colorectal, and prostate cancers, as these among the most prevalent in Nigeria [1].
As a result of attending the MCMC, participants were expected, among other things, to:
- Improve competence clinical evaluation of suspected cancers
- Manage the most prevalent cancers of cancer in the region
- Understand multidisciplinary cancer management
- Understand better when to refer patients to specialists and how to collaborate with specialists
- Provide care to patients who are cancer survivors.
We provided high-fidelity models for breast, pelvic, and DRE. The breast model had interchangeable features demonstrating normal features and various pathologies. The pathologies include masses of various sizes, Peau D'orange, cysts, and axillary lesions. The PE model was designed to provide simulation for various aspects of gynecological education, training, and competency evaluation, including the bimanual exam, speculum exam, and cytology sampling. It featured various pathologies of the ovaries, uterus, cervix, and vagina. We also used an advanced prostate and rectal examination simulator. This model includes several types of prostate and rectal pathologies that are easily exchangeable and can be positioned in three different ways.
The course participants were divided into five streams of about 18 individuals each. They rotated among the five simulation stations, namely breast examination, PE, rectal examination, breast biopsy, and pap smear. Each individual had the opportunity to interact with the models at each station and to receive feedback from a trainer. Trainers included specialists and senior residents in relevant specialties.
Course participants were essentially physicians and nurses in AKS, especially people at the primary, secondary, and tertiary levels. These are clinicians who would perform breast, pelvic, and rectal examinations as part of their clinical roles. Participants were selected from each of the three senatorial districts in the state. Furthremore, we had participants from public, private, and faith-based organizations. A total of 92 individuals attended the course, whereas 51 completed the evaluation of the simulation-based training. Due to space considerations, we did not open the invitation to everyone who could attend. Every participant had equal opportunity to complete the survey, however, a convenience sample returned completed pre- and post-evaluation tools.
Data collection involved using surveys (pre-and-post), in the form of course evaluation. The surveys also contained open-ended questions for comments. Information collected included demographic data on profession, cancer-related clinical practice, likelihood of applying skills gained through simulation, as well as rating of the simulation experience. Survey data were analyzed using descriptive statistics, repeated measures t-test, Wilcoxon test, as well as Chi-square, where appropriate. Deductive content analysis was for the comments.
FINDINGS AND DISCUSSION
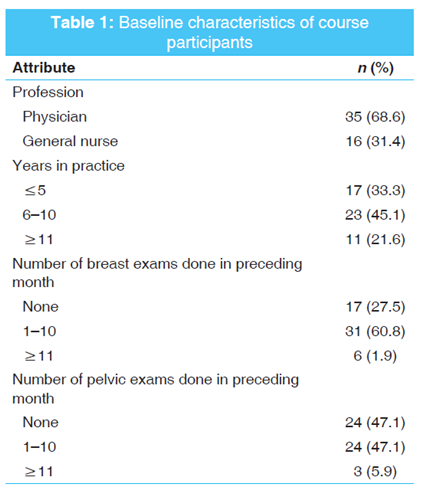
A total of 51 course evaluation forms were completed, out of 92 unique participants, giving a response rate of 55.4% (51/92). Most participants (68.6%, 35/51) were physicians. The average number of years in practice was 8 (±5.2) years. Table 1 shows the baseline characteristics of course participants.
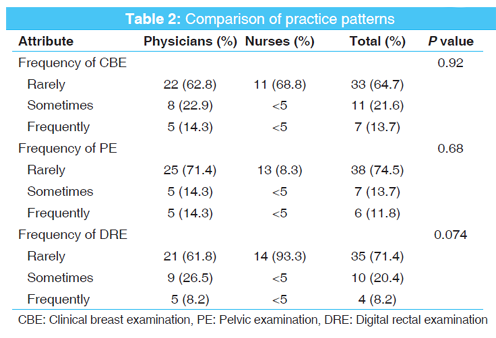
We compared the practice pattern of physicians and nurses regarding the frequency of performing relevant clinical examinations, and their self-reported comfort levels in performing the examinations. The examinations of interest were CBE, PE, and DRE. Chi-square test was used to compare the practice patterns between physicians and nurses. Cells with fewer than five observations were suppressed to protect the anonymity of the participants. There were no statistically significant differences in the frequency of performing examinations between both professions; however, more physicians (71.4%) appeared to avoid PE and more nurses appeared to avoid rectal examinations (93.3%). Table 2 describes the practice patterns.
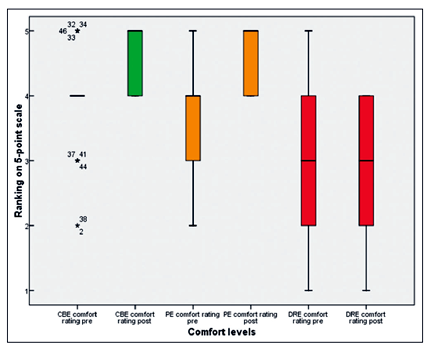
Likert-like questions were used to evaluate comfort in performing clinical exams and the likelihood of ordering the examinations. Wilcoxon signed-rank tests as used to compare the median ranking of the self-reported comfort levels. Participants demonstrated significant gain in CBE median comfort levels (pre-4 vs. post-5, P < 0.001) as well as PE median comfort levels (pre-4 vs. post 5, P < 0.001). Figure 1 is a box plot showing a comparison of the median ratings.
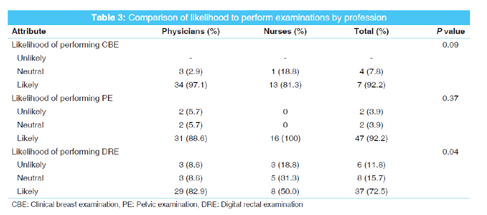
In addition, participants were asked to self-report their likelihood of using the skills in patient care going forward. There is a general trend where most participants were likely to perform PE (92.16%), CBE (92.16%), and DRE (72.55%). Table 3 compares the likelihood of performing these examinations between physicians and nurses.
The following are emergent themes from inductive analysis of open-ended comments regarding their perspectives on the use of simulation for medical education. Most important things participants learned were coded under three major headings; "effective learning (25)," "clear understanding (15)," and "collaborative learning (4)."
Some of the comments were:
"The use of simulation gives a relaxing atmosphere and may seem a necessary tool for practice. Real life simulation may be less comfortable" (#8); "the use of simulation is quite commendable as it gives room for improvement before using a human" (#24).
"It gives a visual view of organs that are not obvious. It is excellent" (#7). "simulation helps to build up confidence and increases precision before using actual patients" (#19). "simulation makes the whole session clearer" (#18).
"Interesting... using models would enable, but doctors collaborate with us (nurses) to partake any examination procedure in the hospital on pelvic exam."
Most participants (84%, 43/51) rated the course as "very good." Figure 2 shows the course rating.
According to the participants, "the use of simulation is quite commendable as it gives room for improvement before using a human" (#24); "...it is the best method of learning I have ever enjoyed" (#31).

DISCUSSION
To the best of our knowledge, this is the first published study describing the use of simulation for continuous professional development courses in the Nigerian medical community. Study participants were skewed toward physicians, due to the method of recruitment for the MCMC. It is possible that a different method of selection might change the outcome. The distribution of our sample in terms of years of clinical practice is typical for Nigeria [4,5].
It appears that more people in our sample performed limited clinical examination relating to the common cancers. For instance, almost 90% of the participants performed fewer than 10 clinical breast or PEs, in the preceding month. Considering that the average physician in Nigeria might consult about 35 patients daily,[15] this leaves much to be desired. It is possible that this observation speaks to the large patient load, long wait-times and short consultation time in Nigerian health institutions [15]. Although comparison of the practice patterns of physicians and nurses did not show a significant difference, it revealed interesting trends. Most physicians (71%) rarely performed PE while 93% of nurses rarely performed DRE. Our study was not sufficiently powered to determine if there were gender-based differences in this pattern.
The use of simulation appeared to significantly raise the comfort levels of individuals in performing a clinical breast and PEs. The median self-reported comfort levels for each of those measures were pre-4 versus post-5, P < 0.001. The impact on DRE was not quite clear. It is possible that the participants did not have sufficient interaction with the model at this station, judging from the comment of participant #15 "...More than one simulation (model) should be provided to enable all students actively involve in the clinical practice." Evidently, all participants enjoyed their experience in simulation-based continuing education. Common themes from their comments reflect the positive impact of the encounter. Participant #34 summed it up in saying "it's very educating, (and) I have really learned a lot. This will improve my practice."
One of the limitations of this study is that we did not have a large sample size (n = 51) to perform more detailed analysis. This reduces the generalizability of our findings. Our findings reflect their self-reported perception of comfort based on what their experience. This makes it difficult to measure actual knowledge change with accuracy.
CONCLUSION
Simulation-based education is an emerging field that has increasingly improved the competence and confidence of clinicians globally. This is the first study to demonstrate this potential in a Nigerian population. Participants at the MCMC have shown that providing simulation-based training can be achieved in Nigeria and that people appreciate it. Further research with a larger number of participants is required to further understand how best to implement simulation-based education in Nigeria. Findings from this project have been previously presented as an abstract [16].
The evaluation data used to support the findings of this study may be released on application to the corresponding author, who can be contacted at keguzo@gmail.com.
ACKNOWLEDGMENT
The authors would like to acknowledge the contributions made by members of the MCMC planning committee, Staff of MWAN (AKS Branch), Staff of Methodist General Hospital, Ituk Mbang, and professional organizations toward the success of the MCMC course. The authors acknowledge the partial presentation of the manuscript as an abstract that the 2018 Annual Meeting of the ASCO.
CONFLICT OF INTEREST
Kelechi Eguzo has research relationship with Pfizer Inc, but this did not influence this research.
REFERENCES
- Jedy-Agba E, Curado MP, Ogunbiyi O, Oga E, Fabowale T, Igbinoba F, et al. Cancer incidence in Nigeria: A report from population-based cancer registries. Cancer Epidemiol 2012; 36:e271-8.
- Eguzo K, Camazine B. Beyond limitations: Practical strategies for improving cancer care in Nigeria. Asian Pac J Cancer Prev 2013; 14:3363-8.
- Love RR, Ginsburg OM, Coleman CN. Public health oncology: A framework for progress in low- and middle-income countries. Ann Oncol 2012;23:3040-5.
- Ekanem U, Eguzo K, Akwaowo C, Kremzier M, Eyo C, Abraham E. Cancer education in Nigeria: Findings from a community-based intervention by a physicians' association. Cancer Oncol Res 2017;44:73-7.
- Nwogu C, Mahoney M, George S, Dy G, Hartman H, Animashaun M, etal. Promoting cancer control training in resource limited environments: Lagos, Nigeria. J Cancer Educ 2014; 29:14-8.
- Ogboli-Nwasor E, Makama J, Yusufu L. Evaluation of knowledge of cancer pain management among medical practitioners in a low-resource setting. J Pain Res 2013;6:71-7.
- Anorlu RI, Ribiu KA, Abudu OO, Ola ER. Cervical cancer screening practices among general practitioners in Lagos Nigeria. J Obstet Gynaecol 2007;27:181-4.
- Nwankwo KC, Anarado AN, Ezeome ER. Attitudes of cancer patients in a university teaching hospital in Southeast Nigeria on disclosure of cancer information. Psychooncology 2013; 22:1829-33.
- Anyebe EE, Opaluwa SA, Muktar HM, Philip F. Knowledge and practice of cervical cancer screening amongst nurses in Ahmadu Bello university teaching hospital Zaria. Res on Hum Soc Sci 2014;4:33-40.
- Eguzo K, Umezurike C, Jacobs C, Camazine B. Where There is No Oncologist: Manual of Practical Oncology in Resource-Limited Settings. Texas: Earthwide Surgical Foundation; 2012. p. 53.
- Eguzo K, Akwaowo C, Ekanem U, Eyo C, Abraham E. Cancer education in Nigeria: Reflections on a community-based intervention by a physicians'association. Cancer Stud Ther J 2016; 1:1-4.
- Lane J, Slavin S, Ziv A. Simulation in medical education: A review. Simul Gaming 2001;32:297-314.
- Scalese RJ, Obeso VT, Issenberg SB. Simulation technology for skills training and competency assessment in medical education. J Gen Intern Med 2008;23 Suppl 1:46-9.
- Dilaveri CA, Szostek JH, Wang AT, Cook DA. Simulation training for breast and pelvic physical examination: A systematic review and meta-analysis. BJOG 2013;120:1171-82.
- Oche M, Adamu H. Determinants of patient waiting time in the general outpatient department of a tertiary health institution in North Western Nigeria. Ann Med Health Sci Res 2013; 3:588-92.
- Eguzo KN, Okwuosa C, Ekanem US, Akwaowo CD, Mkpang ED. Use of medical simulation for cancer education in Nigeria. J Clin Oncol 2018;36:11011.