Magnetic Resonance Imaging Findings in Autoimmune Pancreatitis and
Cholangitis
Ouijdane Zamani1, Rachida Saouab2
2.Radiology Unit, Faculty of Medicine and Pharmacy of Marrakech, Mohammed V Military Teaching Hospital, Cadi Ayyad University, Rabat-Morocco.
Citation : Zamani O, Saouab R. Magnetic Resonance Imaging Findings in Autoimmune Pancreatitis and Cholangitis. J Clin Res Radiol 2018;1(2):1-2.
Autoimmune pancreatitis (AIP) is a distinct form of chronic pancreatitis. The presentation and clinical image findings of AIP
sometimes resemble those of several pancreatic malignancies, but the therapeutic strategy differs appreciably. The purpose of this article is to discuss its various pancreatic and extrapancreatic imaging finding especially on MRI.
Autoimmune pancreatitis, cholangitis, MRI
INTRODUCTION
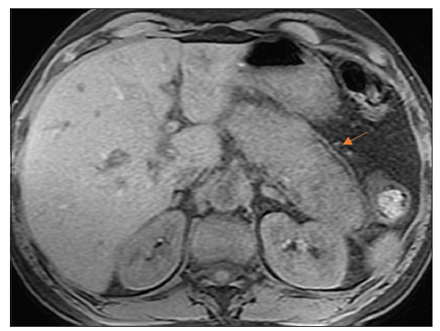
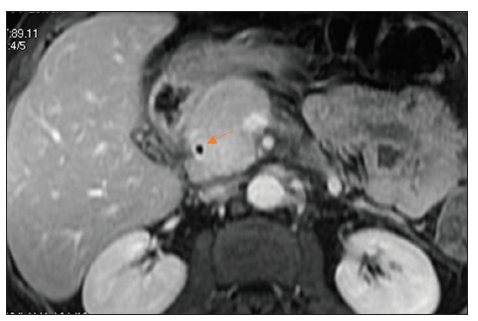
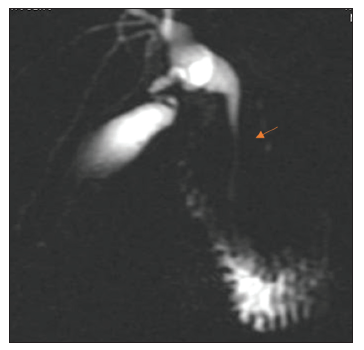
A52-year-old non-alcoholic man, with no medical history, presented to our hospital with epigastric pain, jaundice, and 5 kg weight loss. Vital signs were stable. Serum analyses revealed an elevated total bilirubin, direct bilirubin, aspartate aminotransferase, alanine aminotransferase, and a normal level of lipase (35 u/L). Ultrasound examination showed a moderately dilated intrahepatic and extrahepatic bile ducts with enlarged and heterogeneous head of the pancreas. Magnetic resonance imaging revealed diffuse parenchymal enlargement with effacement of the lobular contour of the pancreas and a capsule like was noted as a halo which is hypointense on both T1- and T2-weighted images [Figure 1, arrow]. The common bile duct (CBD) wall showed an enhancement during the late phase of contrast [Figure 2, arrow] consistent with cholangitis. On magnetic resonance cholangiopancreatography (MRCP), there was a mild dilatation of the intrahepatic bile ducts and a regular distal CBD stricture [Figure 3, arrow]. Therefore, the diagnosis of autoimmune pancreatitis (AIP) was suspected and a dosage of immunoglobulin (IgG4) antibody was requested and returned high. The patient was started on high-dose prednisone with significant improvement in his symptoms.
AIP was first described by Yoshida et al.,[1] in 1995, as a form of chronic pancreatitis associated with autoimmune manifestations. It is a rare but important differential diagnosis from pancreatic cancer (PC) [2]. The disease can occur as alone or in association with autoimmune disorders including sclerosing cholangitis, rheumatoid arthritis, primary biliary cirrhosis, inflammatory bowel disease, hypothyroidism, sarcoidosis, and Sjogren's syndrome [3]. AIP is a form of chronic pancreatitis characterized by frequent presentation with obstructive jaundice, simultaneous or metachronal occurrences of extrapancreatic lesions, histology of lymphoplasmacytic infiltrates with fibrosis, and a dramatic response to corticosteroids [4]. AIP is also known by other names including lymphoplasmacytic sclerosing pancreatitis with cholangitis, idiopathic duct destructive pancreatitis, primary inflammatory pancreatitis, and non-alcoholic duct destructive chronic pancreatitis. Clinical features and biological data often resemble those of PC. This is why the differential diagnosis must be carried out carefully [5]. The imaging characteristics of CT and MR are essential for retaining the diagnosis of AIP and ruling out other potential etiologies, particularly PC. Imaging data that are relatively specific to AIP include diffuse pancreatic hypertrophy, the presence of a hypoattenuating capsule edge, and delayed parenchymal enhancement [6]. The most frequent extrapancreatic lesions occur in the biliary tree with asymptomatic liver test abnormalities or jaundice [7]. On imaging, biliary involvement commonly appears as multifocal biliary strictures similar to primary sclerosing cholangitis. Enhancement of the common biliary duct wall may be present in patients with AIP as it has been the case in our patient. The most sensitive and specific serum markers for AIP type 1 are IgG4 (≥135 mg/dL, sensitivity: 86%, specificity for AIP against PC: 96%), their level is elevated in AIP type 1 and normal in AIP type 2 [8]. AIP can be treated with steroids and does not require surgery. Due to the similar characteristics with PC, sometimes, unnecessary surgical resection is performed. In these cases, the lymphoplasmacytic infiltrate characteristic of AIP has been observed in about 1/3 of the cases making it possible to correct the diagnosis [9].
REFERENCES
- Yoshida K, Toki F, Takeuchi T, Watanabe S, Shiratori K, Hayashi N, et al. Chronic pancreatitis caused by an autoimmune abnormality. Proposal of the concept of autoimmune pancreatitis. Dig Dis Sci 1995;40:1561-8.
- Hayakawa T, Naruse S, Kitagawa M, Kondo T. Clinical aspects of autoimmune pancreatitis in sjogren's syndrome. JOP 2001;2:88-92.
- Schneider A, Steih J, Mosler D, Pfutzer RH, Lohr JM, Singer MV. Frequency of autoimmune pancreatitis (AIP) in patients with acute and chronic pancreatitis from Germany.Pancreatology 2009;9:454-5.
- Okazaki K, Uchida K, Matsushita M, Takaoka M. How to diagnose autoimmune pancreatitis by the revised Japanese clinical criteria. J Gastroenterol 2007;42 Suppl 18:32-8.
- Matsubayashi H, Matsunaga K, Uesaka K, Fukutomi A, Sasaki K, Furukawa H, et al. A case of pancreatic carcinoma with suspected autoimmune pancreatitis. Clin J Gastroenterol 2009;2:59-63.
- Takahashi N. CT and MR Features of Autoimmune Pancreatitis. Pancreapedia: Exocrine Pancreas Knowledge Base; 2013.
- Takahashi N, Fletcher JG, Fidler JL, Hough DM, Kawashima A, Chari ST, et al. Dual-phase CT of autoimmune pancreatitis: A multireader study. AJR Am J Roentgenol 2008;190:280-6.
- Okazaki K, Uchida K, Ohana M, Nakase H, Uose S, Inai M, et al. Autoimmune-related pancreatitis is associated with autoantibodies and a th1/Th2-type cellular immune response. Gastroenterology 2000;118:573-81.
- Finkelberg D, Sahani D, Deshpande V, Brugge W. Autoimmune pancreatitis. N Eng J Med 2006;355:2670-6.