Disorganized Diseases: Are they a Simple Explosion of Random Energy and therefore Meaningless? A Cases Series Study in Family Medicine
Jose Luis Turabian1
Citation : Turabian JL. Disorganized Diseases: Are they a Simple Explosion of Random Energy and therefore Meaningless? A Cases Series Study in Family Medicine. J Community Prev Med 2018;1(1):1-11.
The study has two objectives: (1) To determine the prevailing characteristics of a given set of patients with "disorganized disease" and (2) to determinate the prevailing outcomes for these patients in family medicine to assess their
implications for decision-making.
A qualitative, longitudinal, and retrospective cases series
study based on a single cohort was carried out. Analyses based on a retrospective study of case records from June to
October 2017, in a family medicine office in the Health Center Santa Maria de Benquerencia, Toledo, Spain. A convenience
sample was selected consisting of patients who consulted during that period and who met the criteria for entering the study.
These cases were considered in the epidemiological term as index cases, which means that beyond these the study should
be expanded. Hence, in addition, using a technique of snowball "mental" or "astute clinical observation" others patients
attended previously were included until the saturation of the data. The cases were described in short case reports. An analysis
of the content of these reports was carried out, defining categories of qualitative data. The results were interpreted, and
a generalization was drawn from these cases.
There were 22 cases, 9 men (6<65 years and 3=65 years), and 13
women (10<65 years and 3=65 years). The age range was from 30 to 71 years. The categories obtained after reading the
clinical cases were: (1) Multiple symptoms of many organs and systems (100%), (2) psychological symptoms (100%), (3)
psychosocial factors (100%), (4) frequent attenders (100%), (5) symptom of pain (95%), (6) digestive and genitourinary
symptoms (82%), and (7) a triggering or aggravating factor (77%, often psychosocial, accident or complications of
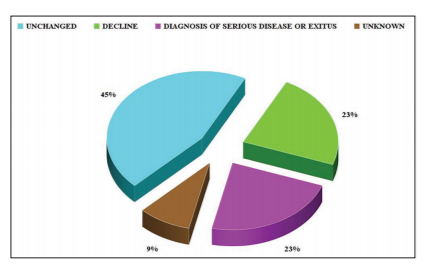
multimorbidity and polypharmacy). Evolution was: (1) Unchanged (45%), (2) decline (23%), and (3) serious diagnoses
(23%), these especially in cases of multimorbidity and polypharmacy. In 11 of the 22 cases (50%), there was a moderate or
severe degree of polypharmacy. 28% had severe multimorbidity.
Family doctor should learn to coexist with
that "disorganization," he must detect and manage psychosocial symptoms, pain, and digestive, and genitourinary symptoms,
he must be alert to the triggers (psychosocial, accident, or complications of multimorbidity and polypharmacy), and he must
make as far as possible, early diagnosis, and to avoid complications and adverse effects. There is a misconception about
the disorganized disease in family medicine that considers they are mere unorganized explosions of random energy, and
therefore, meaningless. However, presentation of disorganized disease in family medicine should be appreciated because it
offers more data than it seems.
Communication, complexity, diagnostic techniques, family practice, physician-patient relations, procedures, symptom assessment
"The painter Jackson Pollock was not an uncontested genius during his lifetime. The critic Robert Coates once derided a number of Pollock's works as "mere unorganized explosions of random energy, and therefore meaningless".
INTRODUCTION
Family medicine presents special characteristics that differentiate it from other medical specialties. In family medicine, it is necessary to evaluate the presentation of the symptoms, in addition to the symptoms themselves. That is, the reason for the consultation begins or emphasizes important issues for the patient, and not just symptoms, in a context of communication [1,2].
Thus, although with differences according to different ways of classifying the types of consultations that a general practitioner makes, according to different perspectives, family doctor can see in a normal day of work between 20% and 30% of patients "without disease" (when the person presenting himself as a patient does not have a situation suggestive of illness; such as preventive visits, pre- and postnatal visits, vaccinations, and health examinations), and other 65% of patients with self-limited diseases that do not require any intervention. Further, others patients have symptoms without the disease. There could also be near to 20% of patients with chronic diseases and multimorbidity, and 15% with acute diseases. On the other hand, it has been reported that between 50 and 70% of the patients treated in family medicine present, at any time, disorganized symptoms or diseases; therefore, account for the majority of patients cared for in family medicine [3].
Patients of the general practitioner do not fit adequately into the traditional diagnostic categories. The general practitionerm finds that many, if not most of his patients do not fit adequately into the traditional diagnostic categories, and it is not easy to choose the right treatment so that many general practitioners are frustrated by their inability to "do something" for these people. Family doctors see patients who experience and live their symptoms in a personal way. In textbooks, the symptoms are conceived as expressions of defined organic alterations. Doctors learn to recognize illness by becoming familiar with patient prototypes, but family physicians never see symptoms that correspond exactly to those prototypes, but symptoms that are experienced by humans trying to communicate their discomfort or concern with signs that start from their bodies [3,4].
The symptoms expressed by patients in the consultation (especially in family medicine) can have different meanings: Expressions of biochemical alterations, symbolic expressions, expressions of the group context, expressions of family stress when going through developmental transactions, expressions of coping with a situation or event, expressions of "family character or style" symptoms, somatic expressions associated with mental problems and functional or psychosocial expressions associated with organic problems, or social and historical expressions [1,5]. Some physicians develop intuitive methods to deal with this problem, others simply ignore it, but few doctors feel comfortable treating patients to whom "disease-centered" medicine has little to offer [6,7]. The problem in family medicine is to assess the significance of symptoms for diagnosis [8], and theory fails to provide sufficient guidance on where the boundaries of disease [9].
In this stage, what are disorganized diseases? It is those symptoms or problems that give the doctor a feeling of confusion, disorder, uncertainty, or insecurity with respect to the traditional diagnostic categories, and that is not fully developed or open in the interview, and at the same time an expectation about its evolution [10]. Symptoms are often "disorganized", not readily recognizable, and can be presented by symbols, as does the arrangement of notes in a musical score. Perhaps the family doctor has to approach the symptoms as if they were "music": Like a mysterious constellation; seeking order in disorder, or better trying to understand some of the disorder [11]. In the hospital, medical specialists "detest" (possibly rightly, in that context) the qualitative and disorganized diseases, these notes in a mysterious musical score, the disorders with multiples connections, especially with social connections, so that these problems become the task of the family doctor.
In this context, we perform a qualitative study whose two objectives are: (1) To determine the prevailing characteristics of a given set of patients with "disorganized disease" and (2) to determinate the prevailing outcomes for these patients in family medicine to assess their implications for decision-making.
PARTICIPANTS AND METHODS
A qualitative, longitudinal, and retrospective cases series study was carried out. Analyses based on a retrospective study of case records from June to October 2017, in a family medicine office in the Health Center Santa Maria de Benquerencia, Toledo, Spain, which has a list of 2000 patients. Patients of both sexes over 14 years old were included (In Spain family doctors attend patients over 14 years old).
A convenience sample was selected consisting of patients who consulted during that period and who met the criteria for entering the study. An operational criteria definition of "disorganized disease" was considered as follow [10]:
1. Presentation of complaints in an unorganized way from the biological point of view
2. Feeling by the doctor of "inability to do something" for these people
3. The symptoms are sufficiently annoying for the patient to listen to himself and go to the doctor, although his problems do not seem to reflect a severe pathology
4. In these visits, the discomfort and the psychological regression arise from the beginning. Balance is threatened, and regression to infant models occurs when the individual is threatened by external pressures or by his internal psychopathology
5. When doctor and patient are not in agreement in a diagnosis, organic, or psychological
6. When the doctor has the intuition or feeling that there is hidden data that should come to light
7. When several medical problems are treated in a patient (e.g., peptic ulcer, anorexia, and depression), but there is no way to explore an overall diagnosis that to the whole
8. When it is not clear if the patient is who make the consultation or another member of their environment
9. When doctor-patient relationship is not oriented around the disease.
During this period of time, the doctor of the consultation (who remains in the same consultation more than 20 years), in addition to collecting the new cases presented, using a technique of snowball "mental", he reflected and tried to remember, other patients previously attended with the criteria of "disorganized diseases", that he would have attended outside that time interval, or even about patients deceased, that reminded him of this subject.
The conceptual basis of this method is as follows: The presentation of a limited number of cases indicates that these cases are probably nor unique and that a better descriptive study might or should be attempted. Such cases - cases attended during the study period - can be considered in the epidemiological term as index cases, and it means that beyond these the study should be expanded. The "astute clinical observation" was the root of case series report. Hence, this is a longitudinal and retrospective study, based on a single cohort. Repeated measurement or evaluation in this situation allows for better understanding of the clinical course of cases and their outcomes.
From the medical record, other documents such as specialist reports and physician-patient interview data, the cases were described in short case reports that were followed by a generalization that can be drawn from these cases. This was continued, including new cases detected during the time of the study, as well as from the archive of medical records when recalling any previous case, until the saturation of the data: When new clinical cases did not contribute new categories or data to the previous ones.
No ethical approval was required for the study as this was part of a normal service with the registration of the reasons for consultation in the patient's medical records.
The cases were described in short case reports. An analysis of the content of these reports of each patient included was carried out, defining codes or categories of qualitative data, relating phrases sections with categories developed during the process of collecting narratives, and carrying out this process of organizing qualitative data using Microsoft® Word [12,13].
The process was as follows: (1) The written transcripts of the case reports of disordered diseases were read by the researcher, and categories were assigned to each of them, (2) a new reading of the categories was made for each case report, re-assigning material of original data to new categories, and thus forming a file of definitive categories, and finally, (3) the results were interpreted and a generalization was drawn from these cases.
Methodological triangulation.
Four sources of evidence were used:
- Documentation
- Archival records
- Interviews, direct observations
- Participant physical artifacts
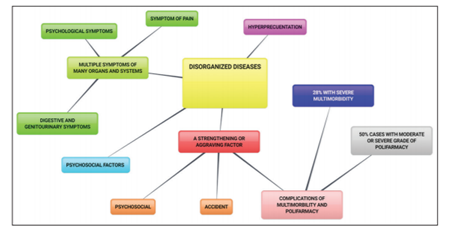
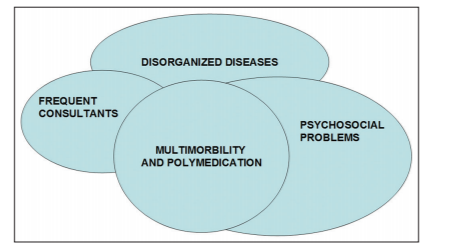
Finally, a mental map was drawn [Figure 1], not only to arrange the results in graph form but also as a qualitative technique to understand the results in an integral or global way [14-16], using the free bubbl.us® online system [17]. In addition, a Venn diagram was drawn to show the possible overlapping of concepts or factors in disorganized diseases [Figure 2].
RESULTS
There were 22 cases, 9 men (6 <65 years and 3 =65 years), and 13 women (10 <65 years and 3=65 years). The age range was from 30 to 71 years.
The categories obtained after reading the clinical cases were: (1) Multiple symptoms of many organs and systems (in different degree, in 100%), (2) psychological symptoms (in different degree, in 100%), (3) psychosocial factors (in different degree, in 100%), (4) frequent attenders (in different degree, in 100%), (5) symptom of pain (in varying degrees, in 95%), (6) digestive and genitourinary symptoms (to varying degrees, in 82%), and (7) a triggering or aggravating factor (77%, often psychosocial, accident, or complications of multimorbidity and polypharmacy).
Evolution was: (1) Unchanged (45%), (2) decline (23%), and (3) serious diagnoses (23%), these especially in cases of multimorbidity and polypharmacy.
In 11 of the 22 cases (50%), there was a moderate or severe degree of polypharmacy.
It was considered that 6.22 (28%) presented severe multimorbidity, 8.22 (36%) moderate, 6.22 (27%) light, and 2.22 (9%) no multimorbidity (which is a subjective assessment, because by the very fact of having disorganized symptoms, there were sometimes no rigorously labeled diagnoses) [Table 1 in PDF]. Figure 1 shows a mental map with these categories.
The concept of disorganized disease overlaps with other as frequent attenders and multimorbidity and polypharmacy. Figure 2 shows a Venn diagram with the overlap of these factors.
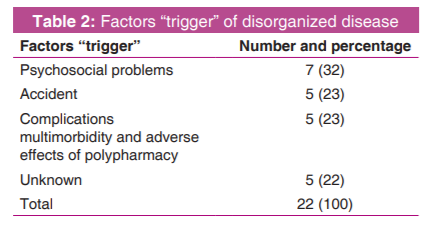
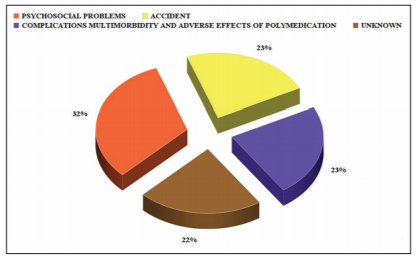
There is often a triggering or aggravating factor that is mainly a psychosocial factor (maltreatment, family crisis), and less frequently an accident, or adverse effects of polypharmacy in patients with multimorbidity [Table 2 and Figure 3].
The courses of evolution over the months or years that are observed are:
- The disorganization does not change and remains stable
- The disorganization tends to disappear more or less spontaneously without assuming any new diagnosis or significant problems
- Disorganization tends to be organized in severe or very severe pathologies, and finally, they may even ensue inthe death of the patient [Table 3 and Figure 4].

DISCUSSION
The quality approach is recommended when the level of uncertainty is high, theory and direction obscure, and situations are novel and complex [18]. These characteristics occur in "disorganized diseases", so a qualitative design of the study was decided. Case series studies are studies of "numerators" only. In addition to the "numerator focus" of case series, only one set of patients is under study. No control group or controlled assignments of patients are involved. Nevertheless, aside from these inherent limitations, case study series are often the only source of information about the problem of interest [18]. The presentation of a limited number of cases indicates that these cases are probably nor unique and that a better descriptive study might or should be attempted. Such cases can be considered in the epidemiological term as index cases, beyond the study be expanded [18]. Thus, in our study, the number of cases was expanded by means those the medical researcher recalled having previously attended.
The consultation of family medicine has high entropy: It indicates disorganization and maximum uncertainty; it is not a reversible and controllable process in all its variables, nor foreseeable in its processes, evolution, and transformation [19,20]. The "modus operandi" of the family doctor is also "dirty" or "disorganized" methods; he faces dark subjects, casual data, therapeutic tests and anecdotal observations, and relies on decisive moments. Family doctors are grateful to the tools that have given us clinical-knowledge, discipline, and drugs that sometimes work. However, he must also recognize that the center of academic medicine is a monolith of truth and knowledge construction that simultaneously reveals a dark area influenced by unknown forces and powerful biases. The achievements of family medicine are the set of chaotic and disorderly elements that pile up in clinical data [21,22]. As John Stuart Mill (about Goethe) said, the family doctor has to accept that "perhaps the greatest mistake of all is to imagine... that... the ideal of life, life itself, and the nature of every cultivated individual in it, to be rounded off and made symmetrical like a Greek temple or a Greek drama. It is only small things, or at least things uncomplex and composed of few parts, that admit of being brought into that harmonious proportion. As well might he attempt to cut down Shakespeare or a Gothic cathedral to the Greek model, as to give rounded completeness" [23].
Entropy not only gives us a relative measure of the disorder of a system in relation to another previous state but it also gives us an idea of the unpredictability of the new forms of organization that will come from the disorder and the liberation of energy. Our data indicate that in almost half of the cases of "disorganized diseases" the disorder remains stable for a long time, and thus, the family doctor has to learn to coexist with this chronic disorder, and not pretend to find or force nature to a harmonious order in all cases. On the other hand, our study shows that in almost 25% of disorganized diseases, they tend to decline spontaneously, so it may be reasonable to avoid unnecessary interventions. But also disorganization tends to be organized in severe pathologies (23%). A typical case is cancer; a messy and excessive cell growth. The trigger that causes a cell to become cancerous can be any external factor capable of destabilizing the normal functioning of the organism causing cellular stress, for example, persistent states of generalized anxiety [24]. There is much evidence, both statistical and anecdotal, that many major diseases including cancer are preceded by periods of unhappiness and disorganized disease. This, if true, adds more emphasis to the important responsibility of the general practitioner at this early stage of the disorganized disease [6].
In the patients with disorganized diseases, the characteristics of multimorbidity, polypharmacy, and frequent consultants overlap. Multimorbidity affects patients by increasing the burden of symptoms. Daily attention is strongly influenced by a growing variety of individual protocols. The result is a serious risk of polypharmacy, which is an indicator of multimorbidity and potentially inappropriate medications [25-27]. The intensity and complexity of the problems can overwhelm even experienced professionals, producing feelings of bewilderment, despair, frustration, and impotence in the family doctor and the patient [28-33]. In addition, the patients are hyper-utilizers or "difficult" patients: They are either those that have repetitive complaints, mainly without clear clinical significance, and strange unsolved complaints, or those who visit the doctor with multiple complaints or whom "everything hurts" [34-36].
Patients usually come to medical office with both mental symptoms as somatic derived from personal or relationship problems, triggered by psychosocial situations as conflicts in the family, work, school, neighbors, debts, deaths, and other serious illnesses related with the environment [37]. The circumstances of the environment in which an individual develops and the events that will facing, especially in childhood and adolescence are important factors and the basis on which constitute the identity, the development of defense mechanisms, coping strategies and social skills necessary for their development [38]. The impact that sustained threat - or chronic stress - has on the eventual development of depression through pathological changes to molecules, cells, neurocircuitry, physiology, and behavior [39]. Trauma is considered any stressful event extreme, something outside the realm of normal human experience, at least for the social group to which the individual belongs, and produces negative consequences on behavior and emotions of the individual, causing problems or symptoms seen as due to anxiety disorders or caused by stress [40,41]. The term stress refers to any requirement or encouragement that we produce a state of tension and that it requests an adaptive change on our part. Doctors have long recognized that people are more prone to diseases of all kinds when they are under great stress. Negative events, such as the death of a loved one, seem to cause enough stress to reduce the body's resistance to disease. However, positive circumstances, such as a new job or the birth of a baby at home, can also alter the normal ability of a person to resist disease [37,41], and multimorbidity is independently associated with a history of adverse childhood experiences [42].
Pain and stress share significant conceptual and physiological overlaps. Medically unexplained pain complaints are associated with underlying unrecognized mood disorders in primary care. There is a well-established comorbidity between migraine and anxiety and depression. Anxiety and depression are consistently associated with pain, regardless of anatomical site. Patients living with chronic daily headache are at risk for future chronic musculoskeletal pain, and vice versa. Chronic low back pain and upper extremity pain are increasingly recognized as often being more than simply an anatomical or physiological problem, and they must be considered as biopsychosocial problems. "Fibromyalgia syndrome" is a biopsychosocial continuum disorder [43-54]. Pathophysiology of upper gastrointestinal (GI) symptoms still is poorly understood. Psychological symptoms were found to be more common in patients with functional GI complaints. Patients with upper GI symptoms visit their family doctor more frequently for problems of any organ system, including psychosocial problems. Anxiety and somatization were significantly related to maximum pain and pain frequency, with somatization explaining more variance [55].
The vital role of the general practitioner is in the interpretation of the unexpressed calls for help [7]. Disorganized presentations cause restlessness and excitement in the doctor. Among the symptoms or reasons for consultation, sometimes after many visits, may appear a detail, such as a sudden revelation, an illumination: The sudden mutual intuitive appreciation or recognition, shared between doctor and patient, of an important understanding, that allows focusing the total diagnosis, which could not have been achieved by other methods [10]. Symptoms in family medicine have the disposition of the notes in a musical score: A mysterious constellation. Hence, therefore, we need qualitative methods to facilitate the application of decisionmaking tools in patients with presentations of disorganized problems [28]. The hospital doctor has to justify his diagnosis by the investigation (complementary tests, analytical, tests of image, etc.). However, the general practitioner has to justify his investigations by his diagnosis [6]. The same evidence does not have the same weight for each context: It may be appropriate in one context, but not in another. Therefore, the interpretations of "true" and "false" have to be modified. A conclusion may be "sufficiently true" in one situation, but not in another [56]. In the management of patients with disorganized diseases a vicious cycle can arise: Since the evolution is uncertain, more complementary biomedical tests are carried out, which can increase anxiety and worsen the disorganization of symptoms; but also always there is the doubt of developing a serious illness, which requires closer monitoring of the patient. Physicians should be aware of this hidden psychosocial morbidity of patients and should incorporate biopsychosocial interventions into routine medical care to be more effective [57].
Case series will remain interesting because of the intrinsic importance of observation in medicine, although individual case reports should never be taken as definitive evidence. A case series without controls can inform about the fate of a group of patients. Such series may content extremely useful information about source, clinical course and prognosis of disorganized diseases but can only hint at efficacy. Case report and case series reports may be the "lowest" or the "weakest" level of evidence "of a cause", but they often remain the first line of evidence of what happened; this is where everything begins [18].
CONCLUSION
Disorganized disease tends to be "organized" in three possible senses: (1) Unchanged or decline (these are the courses that seems to predominate), (2) in a psychosocial organized course; disorganized disease appears to be an expression of problem or psychosocial illness, and (3) a path toward serious illness or serious risk; disorganized disease appears to be the prior expression of a severe occult disorder, specialty in multimorbidity, and polypharmacy. Family doctor should learn to coexist with that "disorganization", he must detect and manage psychosocial symptoms, pain, and digestive and genitourinary symptoms, he must be alert to the triggers (psychosocial, accident, or complications of multimorbidity and polypharmacy), and he must make as far as possible, early diagnosis, and to avoid complications and adverse effects. Significant psychosocial factors, accidents and the presence of multimorbidity and polypharmacy should alert the family doctor as potential factors for the appearance of disorganized diseases. There is a misconception about disorganized disease in family medicine that considers they are "mere unorganized explosions of random energy and therefore meaningless", just as some art critics think about the painter Pollock works: That they do not mean anything [58]. However, about Pollock art and about the presentation of disorganized disease in family medicine we should appreciate that there is more in it than it seems.
References
- Rosendal M, Jarbol DE, Pedersen AF, Andersen RS. Multiple perspectives on symptom interpretation in primary care research. BMC Fam Pract 2013;14:167.
- Rudebeck CE. The clinical method of general practice. Scand J Prim Health Care 1991;supple 1:30-9. Available from: http:// www.tandfonline.com/doi/abs/10.3109/02813439209014088. [Lats accessed on 2017 Nov 10].
- Turabian JL. Family and Community Medicine Notebooks. An Introduction to the Principles of Family Medicine. Madrid: Diaz de Santos; 1995. Available from: http://www.amazon.co.uk/ Cuadernos-medicina-familia-y-comunitaria/dp/8479781920. [Lats accessed on 2017 Nov 10].
- Turabian JL. Is the meaning of symptoms the same in women and men? J Women's Health Care 2017;6:376. Available from: https:// www.omicsgroup.org/journals/is-the-meaning-of-symptomsthe- same-in-women-and-men-2167-0420-1000e129. php?aid=90235. [Lats accessed on 2017 Nov 10].
- Turabian JL, Franco BP. The symptoms in family medicine are not symptoms of disease, they are symptoms of life. Aten Primaria 2012;44:232-6. Available from: http://www.elsevier. es/es/revistas/atencion-primaria-27/los-sintomas-medicinafamilia- no-son-sintomas-90119927-articulo-especial-2012. [Lats accessed on 2017 Nov 10].
- Browne K, Freeling P. The Doctor-Patient relationship. New York: Churchill Livingstone; 1976.
- Hopkins P, editor. Patient-Centred Medicine. Based on the First International Conference of Balint Society in Gran Britain on "The Doctor, His Patient and the Illness", held on 23rd-25th March, 1972 al the Royal College of Physicians, London. London: Regional Doctor Publications Limited; 1972.
- Morrel D. The Art of General Practice. Oxford: Oxford University Press; 1991.
- Doust J, Walker MJ, Rogers WA. Current dilemmas in defining the boundaries of disease. J Med Philos 2017;42:350- 66. Available from: https://www.researchers.mq.edu.au/en/ publications/current-dilemmas-in-defining-the-boundaries-ofdisease. [Lats accessed on 2017 Nov 10].
- Turabian JL. Presentation and approach of disorganized disease in family medicine. J Fam Med Forecast 2017;1:1-4.
- Turabian JL. Relatos clinicos musicales de medicina de familia. Desarrollando las Capacidades Humanisticas de los Medicos de Familia Mediante el arte. Saarbrucken, Deutschland: Editorial Academica Espanola; 2016. Available from : https://www.eaepublishing. com//system/covergenerator/build/25840. [Lats accessed on 2017 Nov 10].
- Bowling A. Research methods in health. Investigating health and health services. New York, NY: Open University Press; 2000.
- Burnard P, Gill P, Stewart K, Treasure E, Chadwick B. Analysing and presenting qualitative data. Br Dental J 2008;204:429-32. Available from: http://www.academia.edu/709185/Analysing_ and_presenting_qualitative_data. [Lats accessed on 2017 Nov 10].
- Buzan T. Use both sides of your brain. New Mind-Mapping Techniques to Help you Raise all of Your Intelligence and Creativity-Based on the Latest Discoveries about the Human Brain. New York: Plume Book; 1991.
- Burnard P. A method of analysing interview transcripts in qualitative research. Nurse Educ Today 1991;11:461-6. Available from: http://www.sciencedirect.com/science/article/ pii/026069179190009Y. [Lats accessed on 2017 Nov 10].
- Whiting M, Sines D. Mind maps: Establishing trustworthiness in qualitative research. Nurs Res 2012;20:21-7.
- Bubbl.us®. Available from: https://www.bubbl.us. [Lats accessed on 2017 Nov 10].
- Jenicek M. Clinical case reporting in Evidence-based Medicine. London: Arnold; 2001.
- Diaz E. Pedagogia del Caos. Available from: http://www. estherdiaz.com.ar/textos/pedagogia.htm. [Lats accessed on 2017 Nov 10].
- Freud S. De la historia de una neurosis infantil y otras obras. Obras completas Sigmund Freud. Volumen 17. Buenos Aires, Argentina: Amorrortu Editores. Available from: http://www. bibliopsi.org/docs/freud/17%20-%20Tomo%20XVII.pdf. [Lats accessed on 2017 Nov 10].
- Loxterkamp D. Saving Fred: What family practice means to medicine. BMJ 2000;321:1567-8. Available from: http://www. bmj.com/content/bmj/321/7276/1567.full.pdf. [Lats accessed on 2017 Nov 10].
- Turabian JL, Perez-Franco B. The Family Doctors: Images and Metaphors of the Family Doctor to Learn Family Medicine. New York: Nova Publishers; 2016. Available from: https://www.novapublishers.com/catalog/product_info. php?products_id=58346. [Lats accessed on 2017 Nov 10].
- Mill JS. Diary. 1854. February 6. In: John Stuart Mill, The Collected Works of John Stuart Mill, Volume XXVII. Online Library of Liberty. [Homepage on Internet]. in the Letters of John Stuart Mill, ed. Hugh S.R. Elliot, 2 vols. (London: Longmans, Green, 1910), Vol. II, pp. 357-86. http://oll. libertyfund.org/titles/mill-the-collected-works-of-john-stuartmill- volume-xxvii-journals-and-debating-speeches-part-ii.
- Melendez-Hevia E. Cancer. Instituto del Metabolismo Celular; 2011. Available from: http://www.metabolismo.biz/web/ cancer. [Lats accessed on 2017 Nov 10].
- Marengoni A, Onder G. Guidelines, polypharmacy, and drug-drug interactions in patients with multimorbidity. BMJ 2015;350:h1059. Available from: http://www.bmj.com/ content/350/bmj.h1059?etoc=. [Lats accessed on 2017 Nov 10].
- Muth C, van den Akker M, Blom JW, Mallen CD, Rochon J, Schellevis FG, et al. The Ariadne principles: How to handle multimorbidity in primary care consultations. BMC Med 2014;12:223. Available from: http://www.biomedcentral. com/1741-7015/12/223. [Lats accessed on 2017 Nov 10].
- Turabian JL, Franco BP. Helping "Dr. Theseus" Leaves the Labyrinth of Multiple Drug Interactions. BMJ 2015;350:h1059. Available from: http://www.bmj.com/content/350/bmj.h1059/ rr-0. [Lats accessed on 2017 Nov 10].
- Turabian JL, Franco BP. A way of helping "Mr. Minotaur" and "Ms. Ariadne" to exit from the multiple morbidity labyrinth: The "master problems. Semergen 2016;42:38-48.
- Turabian JL. "Ariadne and the Minotaur". Qualitative tools to address multimorbidity in family medicine. BMC Med 2014;12:223. Available from: https://www.bmcmedicine. biomedcentral.com/articles/10.1186/s12916-014-0223-1/ comments. [Lats accessed on 2017 Nov 10].
- Turabian JL, Franco BP. Album of models for qualitative tools in the Family Medicine decision making. Other maps to describe a country. Semergen 2014;40:415-24. Available from : http://www.elsevier.es/es-revista-semergen-medicinafamilia- 40-articulo-lbum-modelos-las-herramientascualitativas- S1138359314003827. [Lats accessed on 2017 Nov 10].
- Prados-Torres A, del Cura-Gonzalez I, Prados-Torres JD, Leiva-Fernandez F, Lopez-Rodriguez JA, Calderon- Larranaga A, et al. Multimorbidity in general practice and the Ariadne principles. A person-centred approach. Aten Primaria 2017;49:300-7.
- Ie K, Felton M, Springer S, Wilson SA, Albert SM. Multimorbidity and polypharmacy in family medicine residency practices. J Pharm Technol 2017;33:219-24. Available from: http://www.journals.sagepub.com/doi/ full/10.1177/8755122517725327. [Lats accessed on 2017 Nov 10].
- Farmer C, Fenu E, O'Flynn N, Guthrie B. Clinical assessment and management of multimorbidity: Summary of NICE guidance. BMJ 2016;354:i4843. Available from: http://www. bmj.com/content/354/bmj.i4843. [Lats accessed on 2017 Nov 10].
- Steinmetz D, Tabenkin H. The 'difficult patient' as perceived by family physicians. Fam Pract 2001;18:495-500.
- Haas LJ, Leiser JP, Magill MK, Sanyer ON. Management of the Difficult Patient. Am Fam Physician 2005;72:2063-8. Available from: http://www.aafp.org/afp/2005/1115/p2063. html. [Lats accessed on 2017 Nov 10].
- Smits F, Brouwer H, ter Riet G, van Weert H. Epidemiology of frequent attenders: A 3-year historic cohort study comparing attendance, morbidity and prescriptions of one-year and persistent frequent attenders. BMC Public Health 2009;9:36. Available from: https://www.bmcpublichealth.biomedcentral. com/articles/10.1186/1471-2458-9-36. [Lats accessed on 2017 Nov 10].
- Suarez Cuba MA. The importance of the analysis of stressful life events in clinical practice 2010;16. Available from: http://www.scielo.org.bo/scielo.php?script=sci_ arttext&pid=S1726-89582010000200010. [Lats accessed on 2017 Nov 10].
- Sanz Rodriguez LJ, Garcia de la Pedrosa MG, Almendro Marin MT, Rodriguez Campos C, Izquierdo Nunez AM, Sanchez del Hoyo P. Family structure, stressful life events and psychopathology in the teenager. Rev Asoc Esp Neuropsiq 2009;29.Available from: http://www.scielo.isciii.es/scielo. php?script=sci_arttext&pid=S0211-57352009000200015. [Lats accessed on 2017 Nov 10].
- Ross RA, Foster SL, Ionescu DF. The Role of Chronic Stress in Anxious Depression. Chronic Stress. Available from: http:// www.journals.sagepub.com/doi/full/10.1177/2470547016 689472?utm_source=Adestra&utm_medium=email&utm_ content=The%20Role%20of%20Chronic%20Stress%20in%20 Anxious%20Depression&utm_campaign=701877&utm_ term=. [Lats accessed on 2017 Nov 10].
- Bokanowski T. Variations on the concept of traumatism: Traumatism, traumatic, trauma. Int J Psychoanal 2005;86:251- 65. Available from: http://www.onlinelibrary.wiley.com/ doi/10.1516/PPLT-H9DR-DW3A-X1XU/abstract. [Lats accessed on 2017 Nov 10].
- Cabre M. The psychoanalytic conception of trauma in Ferenczi and the question of temporality. Am J Psychoanal 2008;68:43-9. Available from: http://www.link.springer.com/ article/10.1057%2Fpalgrave.ajp.3350051. [Lats accessed on 2017 Nov 10].
- Sinnott C, Mc Hugh S, Fitzgerald AP, Bradley CP, Kearney PM. Psychosocial complexity in multimorbidity: The legacy of adverse childhood experiences. Fam Pract 2015;32:269-75.
- Aguera L, Failde I, Cervilla JA, Diaz-Fernandez P, Mico JA. Medically unexplained pain complaints are associated with underlying unrecognized mood disorders in primary care. BMC Fam Pract 2010;11:17. Available from: http://www. biomedcentral.com/1471-2296/11/17/abstract. [Lats accessed on 2017 Nov 10].
- Marlow RA, Kegowicz CL, Starkey KN. Prevalence of depression symptoms in outpatients with a complaint of headache. J Am Board Fam 2009;22:633-7. Available from: http://www.jabfm.org/content/22/6/633.abstract. [Lats accessed on 2017 Nov 10].
- Abdallah CG, Geha P. Chronic pain and chronic stress: Two sides of the same coin? Chronic Stress. Thousand Oaks; 2017. Available from: http://www.journals.sagepub.com/doi/full /10.1177/2470547017704763?utm_source=Adestra&utm_ medium=email&utm_content=Chronic%20Pain%20and%20 Chronic%20Stress%3A%20Two%20Sides%20of%20the%20 Same%20Coin%3F&utm_campaign=701877&utm_term=. [Lats accessed on 2017 Nov 10].
- Vargas-Hitos JA, Sabio JM, Martinez-Egea I, Jimenez- Jaimez E, Rodriguez-Guzman M, Navarrete-Navarrete N, et al. Influence of psychological stress on headache in patients with systemic lupus erythematosus. J Rheumatol. Available from: http://www.jrheum.org/cgi/content/abstract/ jrheum.130535v1?papetoc. [Lats accessed on 2017 Nov 10].
- Ligthart L, Gerrits MM, Boomsma DI, Penninx BW. Anxiety and depression are associated with migraine and pain in general: An investigation of the interrelationships. J Pain 2013;14:363-70.
- Jancin B. Chronic musculoskeletal pain travels with chronic daily headache. Oruen 2012. Available from: http://www. oruen.com/cns/chronic-musculoskeletal-pain-travels-withchronic- daily-headache. [Lats accessed on 2017 Nov 10].
- Deyo RA. Biopsychosocial care for chronic back pain. BMJ 2015;350:h538. Available from: http://www.bmj.com/ content/350/bmj.h538?etoc=. [Lats accessed on 2017 Nov 10].
- Ramond-Roquin A, Pecquenard F, Schers H, Van Weel C, Oskam S, Van Boven K. Psychosocial, musculoskeletal and somatoform comorbidity in patients with chronic low back ain: Original results from the Dutch Transition Project. Fam Pract 2015;32:297-304.
- Hauser W, Schmutzer G, Brahler E, Glaesmer H. A cluster within the continuum of biopsychosocial distress can be labeled "Fibromyalgia Syndrome"-Evidence from a Representative German Population Survey. J Rheumatol 2009;36:2806-12. Available from: http://www.jrheum.org/content/36/12/2806. abstract. [Lats accessed on 2017 Nov 10].
- Williams AE, Czyzewski DI, Self MM. Shulman RJ. Are child anxiety and somatization associated with pain in painrelated functional gastrointestinal disorders? J Health Psychol 2015;20:69-379. Available from: http://www.hpq.sagepub.com/content/20/4/369?etoc. [Lats accessed on 2017 Nov 10].
- Bair MJ, Robinson RL, Katon W, Kroenke K. Depression and pain comorbidity. A literature review. Arch Intern Med 2003;163:2433-45. Available from: https://www.jamanetwork. com/journals/jamainternalmedicine/fullarticle/216320. [Lats accessed on 2017 Nov 10].
- Jensen JC, Haahr JP, Frost P, Andersen JH. The significance of health anxiety and somatization in care-seeking for back and upper extremity pain. Fam Pract 2011;29:86-95. Available from: https://www.academic.oup.com/fampra/ article/29/1/86/525890. [Lats accessed on 2017 Nov 10].
- Broker LE, Hurenkamp GJ, ter Riet G, Schellevis FG, Grundmeijer HG, van Weert HC. Upper gastrointestinal symptoms, psychosocial co-morbidity and health care seeking in general practice: Population based case control study. BMC Fam Pract 2009;10:63. Available from: https://www. medpagetoday.com/upload/2009/9/9/1471-2296-10-63.pdf. [Lats accessed on 2017 Nov 10].
- Turabian JL, Franco BP. Responses to Clinical Questions: Specialist-Based Medicine vs. Reasonable Clinic in Family Medicine. Integr J Glob Health 2017;1:1. Available from: http://www.imedpub.com/articles/responses-to-clinicalquestions- specialistbased-medicine-vs-reasonable-clinic-infamily- medicine.pdf. [Lats accessed on 2017 Nov 10].
- Loeb DF, Bayliss EA, Candrian C, deGruy FV, Binswanger IA. Primary care providers' experiences caring for complex patients in primary care: A qualitative study. BMC Fam Pract 2016;17:34. Available from: http://www.bmcfampract. biomedcentral.com/articles/10.1186/s12875-016-0433-z. [Lats accessed on 2017 Nov 10].
- Mcelroy S. If it's so easy, why don't you try it. N.Y. Region, Spotlight, Jackson Pollock. The New York Times; 2010. Available from: http://www.nytimes.com/2010/12/05/ nyregion/05spotli.html. [Lats accessed on 2017 Nov 10].