Understanding Health-care Providers' Perspectives Toward Providing Contraceptives Services for Adolescents in Northern Nigeria
Audu Alayande1, Bahijjatu Bello-Garko1, Islamiyat A. Nuhu2, Oluwatosin Somefun1
2.College of Health Sciences, Igbinedion University, Okada, Nigeria.
Citation : Alayande A, Bello-Garko B, Nuhu IA, Somefun O. Understanding Health-care Providers' Perspectives Toward Providing Contraceptives Services for Adolescents in Northern Nigeria. J Community Prev Med 2018;1(2):1-8.
Adolescents are exposed to several reproductive health challenges including early marriage, unwanted pregnancies, unsafe abortions and sexually transmitted infections. An estimated 14 million adolescents give birth annually of which more than 90% of these occurs in developing countries. Adolescents in the Sub-Saharan Africa have low family planning utilization rates, limited knowledge of reproductive health services and very high pregnancy rates which is not unrelated to the negative attitude of some health care providers towards the provision of Sexual and Reproductive Health (SRH) services and information to adolescents.
The aim of the study was to explore the health workers attitude, practice and its socio-demographic correlates on the provision of contraceptives to adolescents. Methodology: The cross-sectional descriptive study was conducted in Kaduna, Nigeria among Health care workers from public health facilities attending a regional child-spacing conference. The data was collected using a structured self-administered questionnaire which yielded 77% response rate. It was entered and analyzed with SPSS20.
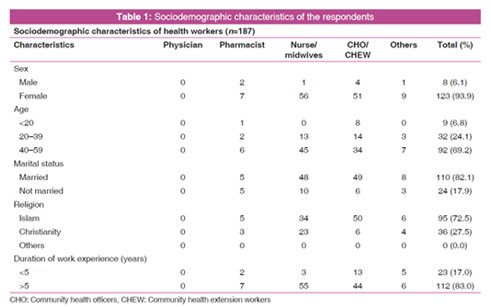
The respondents were mostly females (93.9%), Muslims (72.5%) with an average age of 42 years. Those respondents older than 40 years (67.7%), married (82.9%), of Muslims faith (72.4%) and with more than 5 years of working experience (84.4%) agreed to provide contraceptive counseling to adolescents. Also the majority of health workers that were females (91.4%), above 40 years of age (69.4%), married (84.8%), Muslims (70.1%) and had more than 5 years working experience (85.6%) agreed to provide contraceptives to unmarried adolescents. However none of the respondents wanted to provide IUD to unmarried adolescents.
The majority (83%) of public health workers in Northern Nigeria are willing to provide early contraceptive counseling and services to both married and unmarried adolescents. This findings will further guide the drive to ensure universal access to sexual and reproductive health-care services, including for family planning, information and education.
Adolescent, Contraceptive, Family planning, Early marriage.
INTRODUCTION
Adolescent is individuals between the age group of 10 and 19 years [1]. This is a period of transition from childhood to adulthood characterized by significant physiological, psychological, and social changes. About 82% of adolescent lives in the developing countries of Africa, Asia, and the Pacific [2]. They are exposed to several reproductive health challenges such as early/forced marriage, unwanted pregnancies, unsafe abortions, sexually transmitted infections (STIs including HIV/AIDS), female genital mutilation, malnutrition and anemia in pregnancy, infertility, sexual, and gender-based violence [3,4].
Globally an estimated 14 million adolescents give birth annually of which >90% of these live births occur in developing countries [5]. Conversely, adolescents in the Sub-Saharan Africa region have low family planning (FP) utilization rates, limited knowledge of reproductive health services and one of the highest adolescent pregnancy rates [6]. This is not unrelated to the negative attitude of some health-care providers toward the provision of sexual and reproductive health (SRH) services and information to adolescents [5-8].
Such an attitude had been identified as one of the barriers to service utilization by adolescents which hampers both access and utilization of SRH services, especially among unmarried adolescents.
The Nigeria, 2013, NDHS reported that 70.4% of the sexually active adolescents were never married and 14.4% of never-married adolescents had their past sexual intercourse within the past 4 weeks of the survey [9] Despite this, studies in developing countries have shown the unwillingness of parents, teachers, and health workers to provide age -appropriate SRH information and services to adolescents who had continued to fuel the poor level of SRH information among these group [6,10,11]. The unfavorable attitude displayed by healthcare workers toward the use of health services and uncertainty on what providers will do with the information provided make adolescents feel shy to discuss sensitive topics with their health-care providers [10]. On the other hand, adolescents are also treated disrespectfully and even denied service by health-care providers. This is because some health workers feel uncomfortable discussing such private issues while others belief it may encourage sexual promiscuity among adolescents - value clarification by providers [10].
In Nigeria, only a few studies had actually explored the perspective of service providers toward the provision of contraceptive service and information to unmarried adolescents in the Northern region of the country. This information and its application are vital to the achievement of target 3.7 of the SDG3 - by 2030, ensure universal access to SRH -care services, including for FP, information and education, and the integration of reproductive health into national strategies and programs.
This study, therefore, aim to explore the attitude, practice of various cadres of heath-care providers and sociodemographic correlates on the provision of contraceptives to unmarried adolescents in Northern Nigeria.
METHODOLOGY
The study protocol was reviewed and approved by the health Research Ethics Committee of the Kaduna State Ministry of health and human services.
This cross-sectional descriptive study was conducted among healthcare workers from the 13 States of North West (NW) and North East (NE) Nigeria and 98 local government areas attending a regional FP stakeholders seminar in Kaduna State. The study participants include nurse-midwives, pharmacists, community health officers (CHOs), community health extension workers (CHEWs), and health educators.
Data were collected using a self-administered, structured, and pre-tested questionnaire. The questionnaire consists of sociodemographic characteristics of the health workers, attitude, belief, and practice on the provision of contraceptives to adolescents and recommendations proposed by service providers and decision makers. This was developed from a review of previous literature relevant to FP. The questionnaire was pretested among 10 health workers in a nearby facility, and necessary corrections were made following the pre-test. These were distributed by the data clerk to all participants at the regional FP stakeholders seminar held in November 2017 in Kaduna. The completion and response to the self-administered questionnaire by each participant were made voluntary.
A total of 233 participants were in attendance. The questionnaires were provided to 187 health workers that agreed to participate of which 144 were completed and returned giving a response rate of 77%.
All the responses were entered by a trained data clerk into SPSS20. The data were analyzed using the same software to generate frequency statistics, tables, figures, and Spearman's rank correlation coefficient (p).
LITERATURE REVIEW
The Nigeria minimum service delivery package for Adolescent and Youth Friendly Health Service (AYFHS) allowed the provision of Information, Education and Communication on sexual abstinence, effects of early marriage, early pregnancy, and safer sex practice to adolescent [3]. It also includes counseling and provision of appropriate contraceptives methods (barrier methods, oral contraceptives, and emergency contraceptives) to sexually active young people for the prevention of early and unwanted pregnancy [3]. Nevertheless, there is the limited and irregular use of contraceptives among adolescents and youths despite increasing premarital activities [4].
The current use of any modern contraceptive method by a sexually active unmarried adolescent is 49.7% (male condom 40.7% and pills 6.4%) with an unmet need of 35.3% [5] This is much lower than was reported from Ghana in which the adolescents had 84.0% knowledge of male condom and 82.0% utilization [12]. This situation can be improved by ensuring that service providers are accessible, welcoming, and supportive of informed choices and have adequate stock of various methods [6]
Previous data on the distribution of health providers studied in South Africa showed that they were mostly nurses with age ranged from 25 to 56 years, either married or living together with their partner [7]. However, a similar study conducted in Nigeria showed that the respondents were 66.9% Nurse-midwives, 20.8% CHOs/CHEWs, with age ranged from 18 to 60 years old, 88.8% females, 81.0% Christians, and 79.0% married [10]. Another study on provider imposed restriction on contraceptives from Ibadan South-West (SW) Nigeria consist of 60.0% Nurse-midwives, 32% CHEWs, 89% females, and 69% Christians with an average age of 37 years [11]
The national standard for AYFHS stipulates that service providers should be sensitive to the needs of young people and should maintain their privacy and confidentiality in service provision [3]. It also requires skilled and motivated health providers to deliver adolescent/youth-friendly services to young people.[3] To the contrary, most service providers are often judgmental and may breach confidentiality and rights of young people due to their own innate value preposition [4]. Some nurses felt that the SRH services for adolescents they are expected to provide are sometimes in conflict with their own beliefs and values [7]. All these ensure young people have limited awareness of sexuality and contraception [4].
Evidence had shown that the long-acting reversible contraceptives (LARC) are the most effective contraceptives for teenagers [13]. Unlike the condoms and pills which requires consistent and correct use by a highly motivated individual, LARC methods are effective for years once correctly inserted [13]. Compare to the condoms and pills that have failure rates of about 18% and 9%, respectively, only 1% of LARC users may become pregnant during the 1st year of its use [13].
Despite these facts, providers still exhibit a bias for prescribing appropriate contraceptive methods for certain age group and marital status which limit access by adolescents [11]. Restrictions based on marital status were lowest for condoms (7-10%) and highest for IUDs (67%) [11]. Thus, condoms are commonly dispensed by most providers without bias,[11]. while the majority (90%) of a private physician in the USA usually prescribe the pills for adolescents.[14] This may be related to the limited knowledge and skill of LARC by some providers [7].
Recent concerns regarding the high teenage pregnancy rates, school dropout rates, abortions, and STI and HIV infections among adolescents in South Africa had positively changed the attitude of providers to contraception services for adolescents [7]. Furthermore, 70.7% of health workers in a study conducted in SW Nigeria believed that adolescents should be given contraceptive counseling before they become sexually active [10]. Some of these were inspired by their own personal experiences as teenagers [7]. Some suggestions by health workers to improve contraceptive access to adolescents include the provision of a separate room or space for adolescents medical services, a youth-friendly environment, suitable clinic hours, and school based services [7].
About 86 percent of private physician in the USA are willing to provide contraceptive services to adolescent [14]. This is not the same for an unmarried adolescent for which only 59% agreed to provide such services without parental consent [14]. This decision is somewhat related to state policies [14].
In Nigeria, only a third (33.4%) of the health providers agreed that unmarried adolescents do not require parental consent before contraceptives are provided, 14.5% were undecided while more than half (52.1%) disagreed [10]. Over a third (42.7%) of the them said that unmarried adolescents should not be provided with contraceptives because the Nigerian culture does not support premarital sex [10]. More than half (57.5%) of them were of the opinion that providing contraceptives for unmarried adolescents will promote sexual promiscuity [10]. Nevertheless, one third (41.5%) of the respondents felt that contraceptive services should be provided for both married clients and unmarried adolescents [10].
The age-long tradition and gender biased norms which frown at female sexuality still exist in our society [4]. The practice by its adherent among the service providers, program managers, parents, and other gatekeepers constitute an obstacle to the availability and provision of contraceptive services [4]. Furthermore, health providers often use the fear of side effects as a reason to dissuade adolescents from the use of certain contraceptive methods [8]. More often, they provide young people with condoms, pills, or abstinence [8]. More than half (51.7%) of the providers felt it is better to tell sexually active unmarried adolescents to abstain from sex than to give them contraceptives when it is requested [10]. Times the service providers attitude are also influenced by official regulations, health system constraints, and misinformation about various contraceptive methods [6].
RESULTS
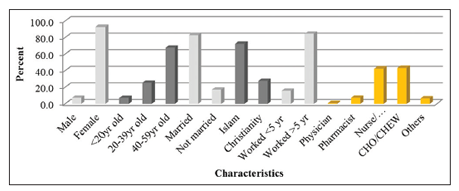
Table 1 shows that respondents were mostly females (94%, n = 123) from both the nurse/midwife (43%) and CHO/ CHEW (39%) professions. 70% of them were >40 years old, mostly married (82%), of Islamic faith (73%), from the NW (85%), and had practiced their profession for more than 5 years (83%).
Most of the respondents that agreed to provide contraceptive counseling to adolescents were females (92.7%, P + 0.18), >40 years (67.7%, P + 0.05), married (82.9%, P + 0.10), Muslims (72.4%, P + 0.05), with >5 years of working experience (84.4%, P-0.05), and mainly of the nurse/midwife (42.4%), and CHO/CHEW (43.2%) professions P-0.10.
The majority of health workers that agreed to provide contraceptives to unmarried adolescents were females (91.4%, P-0.01), >40 years of age (69.4%, P-0.06), married (84.8%, P + 0.09), and Muslims (70.1%, P-0.15), with >5 years working experience (85.6%, P-0.17) and practices nursing (45.8%) or community health (41.1%) P + 0.16. More than 50% of respondents in each cadre agreed to provide contraceptives to unmarried adolescents without parental consent, in their places of work, at the colleges/universities and senior high schools.
More than 70% of the respondents in each cadre had a positive attitude toward the provision of early contraceptive counselling and services to both married and unmarried adolescents. Furthermore, more than 50% of respondents in each profession agreed to provision of contraceptives to unmarried adolescents without parental consent, in their places of work, at the colleges/universities and at senior high schools. About half of the CHO/CHEW and others agreed not to provide contraceptives to unmarried adolescents due to cultural limitation on premarital sex while more than half of the pharmacist will rather preach abstinence to unmarried adolescents.
All the cadres agreed to provide condoms (42.9-58.3%), pills (14.3%-37.5%), and injectables (10.4%-14.3%) to unmarried adolescents except the nurse/midwives groups.
Only the nurse/midwives (20.4%) and CHO/CHEW (12.5%) agreed to provide implants to unmarried adolescents. No respondent wants to provide IUD to unmarried adolescents.
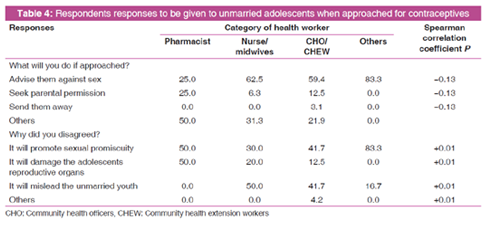
More than 50% of those that will not provide contraceptives to unmarried adolescents (nurse/midwives 63%, CHO/CHEW 59.4%, and others 83.3%) will rather advise them against premarital sex if approached. They think the provision of contraceptives to unmarried adolescents will promote sexual promiscuity (15%), will mislead the unmarried adolescents (12%), and will damage their reproductive organs (5.1%). More than half of the pharmacist will rather preach abstinence to unmarried adolescents.
FINDINGS AND DISCUSSION
The findings of this study contrary to general perception showed that 92.8% of health workers were willing to provide contraceptive counseling to all adolescent and 83.0% were willing to provide contraceptives services to unmarried adolescents. This is a great improvement in the attitude and practice of health providers to the provision of contraceptives to adolescents. The remaining constraints are based on their marital status which is not included in the WHO medical eligibility criteria for contraceptive [15] and also contrary to the Nigeria National Standards and Minimum Service Package for Adolescent and Youth-Friendly Health Services [3]. The dominance of the respondents in Table 1 by mostly females (94%) that were either nurse/midwife (43%) or CHO/ CHEW (39%) reflects the pattern of the health workforce in these states. The sociodemography of the respondents depicts the local reality of Northern Nigeria. Furthermore, 70% of the respondents were >40 years old, 82% were married, 73% were of Islamic faith, 85% hailed from the NW, and 83% had practiced their profession for >5 years. This was because the seminar was attended by senior health officers mostly from the Muslim majority NW States in which the provision of reproductive health and FP are seen as purely a female women affair. This findings aligned with previous studies in terms of the cadre, gender, average age, and marital status of the respondents [7,10,11]. Nevertheless, there were more nurses and mainly of the Christian faith in the previous studies [10,11]. due to the influence of European Christian missionaries and the higher educational attainments in South Africa and SW Nigeria. These are important factors in molding beliefs and practices related to SRH.
Majority (83%) of the health cadres are in support of providing appropriate contraceptive counseling access to adolescents [Figure 1]. These respondents were mainly females (92.7%), > 40 years (67.7%), married (82.9%), of Muslims faith (72.4%), with more than 5 years of working experience (84.4%), mainly of the nurse/midwife (42.4, and CHO/CHEW (43.2%) cadre. This is a great improvement over the previous study in SW Nigeria in which 70.7% of the health workers supported contraceptive counseling for adolescent before they become sexually active [10]. This positive trend was also observed among private physician in the USA in which 86% were willing to provide contraceptive services to adolescents [14]. This may be related to their personal life experience being females, having gone through the adolescent stage and possibly witnessed some affected adolescent during their years of medical practice. The influence of personal experience on providers disposition had been documented in previous studies [7].
It is worthy of note that more than half of various cadre of health workers are willing to provide contraceptives to unmarried adolescents even without parental consent [Figure 2]. Those willing to provide contraceptives to unmarried adolescents were mostly females (91.4%), >40 years (69.4%), and married (82.9%) with more than 5 years of working experience (85.6%).

About 70.1 percent of health worker of Muslim faith and 41.1 percent of the CHO/CHEW cadre were willing to provide contraceptive service to unmarried adolescents than was reported in previous studies [10]. Although the established linear relationship between the professional cadre and the provision of services was weak (P = +0.16), this finding is surprising especially in a predominantly Muslim area where premarital sex is frowned at [4]. This is contrary to other report from South Western Nigeria in which between 42.7% and 57.5% disagreed with the provision of contraceptive to unmarried adolescents for cultural reasons or fear of encouraging promiscuity [10]. They would rather preach abstinence (51.7%) or request for parental consent (66.6%) before the service [10]. The change in opinion could be attributed to the implementation of several reinforcing ASRH strategy which has improved understanding and acceptability of the need to address adolescent sexuality [3]. This is an encouraging development for the advancement of the health and development of the adolescent.
As shown in Table 2, all cadres of health providers agreed to provide condoms (42.9-58.3%) and pills (14.3-37.5%) to unmarried adolescent but mostly with preference for condoms. This finding is in line with previous reports from within and outside Nigeria [8, 11,14]. which may be due to restrictions based on provider bias, [11] fear of side effect, [8] or limited knowledge and skill of LARC [7]. The latter reason can be substantiated with the fact that only the nurse/midwives (20.4%) and CHO/ CHEW (12.5%) agreed to provide implants to unmarried adolescents. These cadres had been largely trained on LARC over the years.
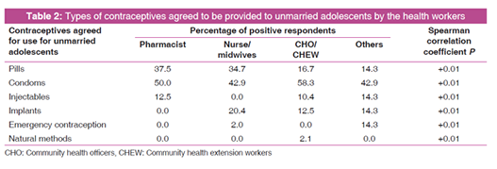
In this study, none of the health cadres is willing to provide IUD to unmarried adolescents. This being an invasive procedure for which the fear of its side effect may deter the providers. Nevertheless, evidence had shown that the LARC are the most effective contraceptives for teenagers [13]. It requires no further effort after the initial insertion and is more effective for prevention of pregnancy [13].
As depicted in Figure 1 and Table 3, >70% of the respondents in each profession had a positive attitude toward the provision of early contraceptive counseling and services to both married and unmarried adolescents. This is much higher than 41.5% reported from SW Nigeria 4 years ago [10]. Furthermore, some (>50%) health workers further agreed to provide contraceptive service to unmarried adolescents without parental consent, in their places of work, at the colleges/universities and at senior high schools. This again substantiates a total shift in paradigm in attitude of health providers to adolescents' access to ASRH services and information [4,7,11] Of importance is the increase in the proportion of providers willing to give services without parental consent which in itself is an obstacle to access [10]. In general, recent evidences, concerns and policy changes had contributed to this positive attitude of service providers to adolescents access to contraceptive information and services [7].
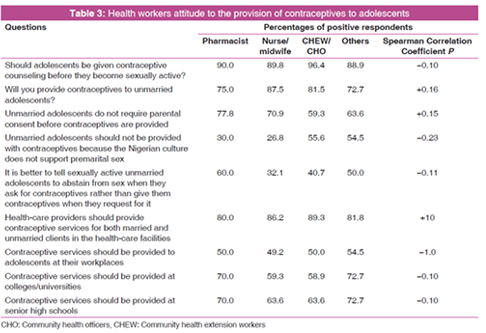
In general, less than a third of the respondents indicated that they will not provide contraceptives to unmarried adolescent [Table 3]. This value varies by cadre and by reasons. Objections to the provision of contraceptives to unmarried adolescents are lower among the frontline health providers. This may be related to their daily experience with adolescents and knowledge of contraceptives. About half of the CHO/CHEW and others agreed not to provide contraceptives to unmarried adolescents due to cultural restriction on premarital sex. As indicated in Table 4, much more of each cadre (nurse/midwives 63%, CHO/ CHEW 59.4%, and others 83.3%) will rather advice against premarital sex if approached. They are of the opinion that the provision of contraceptives to unmarried adolescents will promote sexual promiscuity (15%), will mislead the unmarried adolescents (12%), and will damage their reproductive organs (5.1%). More than half of the pharmacist will rather preach abstinence to unmarried adolescents. These indicate that most of these decisions are rather based on value preposition and beliefs rather than scientific facts [7] Nevertheless, these were not significantly different from previous studies conducted 4 years ago in SW Nigeria [10].
The need for health workers to be more professional rather than being judgmental base on their own socio-cultural belief cannot be overemphasized.
CONCLUSIONS
Majority of healthcare workers in this study were willing to counsel and provide contraceptives to unmarried adolescent. However, the unwillingness of all respondents in this study to provide IUD may limit the available method mix and choices. This calls for continuous orientation of service providers on the WHO eligibility criteria. The findings from this study debunk some of these previous positions and will further guide adolescents about the types of contraceptives available and the profile of service providers that are willing to provide the services.
The information generated from this study and its application is vital to the achievement of target 3.7 of the SDG3 - by 2030, ensure universal access to SRH -care services, including for FP, information and education, and the integration of reproductive health into national strategies and programs.
ETHICAL APPROVAL
Ethical approval for the study was obtained from the health Research Ethics Committee of the Kaduna State Ministry of health and human services. The informed consent of each respondent was sought before administration of the questionnaires. Participation in the study was voluntary.
ACKNOWLEDGMENT
A-A conceived and prepared the paper. B-B-G developed the data collection tool. O-S was the internal reviewer of the final paper. I-A-N searched for the references and typed the final submission. All authors read and approved the final manuscript.
DECLARATION OF CONFLICTS OF INTEREST
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper. This work was funded entirely by contributions from the authors.
REFERENCES
- Encyclopedia Britannica. Available from: https://www. britannica.com/science/adolescence. [Last cited on 2018 Sep 27].
- United Nations. World Population Monitoring. Adolescents and Youth. A Concise Report; 2012.
- FGoN. FMOH. Nigeria National Standards and Minimum Service Package for Adolescent and Youth-Friendly Health Services; 2018. Available from https://www.mindbank.info/ item/6143. [Last cited on 2018 Oct 03].
- Tu X, Cui N, Gao E. Attitudes of Family Planning Workers on the Provision of Sexual and Reproductive Health Services to Unmarried Young Adults in China. Available from: https://www.pdfs.semanticscholar.org/3c38/ dfdb1c3df554f6ee766a08384290152ce3a9.pdf. [Last accessed on 2018 Feb 02].
- Tilahun M, Mengistie B, Egata G, Reda AA. Health workers' attitudes toward sexual and reproductive health services for unmarried adolescents in Ethiopia. Reprod Health 2012;9:19.
- Radovich E, Dennis ML, Wong KLM, Ali M, Lynch CA, Cleland J, et al. Who meets the contraceptive needs of young women in Sub-Saharan Africa? J Adolesc Health 2018;62:273-80.
- Jonas K, Crutzen R, Krumeich A, Roman N, van den Borne B, Reddy P. Healthcare workers' beliefs, motivations and behaviours affecting adequate provision of sexual and reproductive healthcare services to adolescents in Cape Town, South Africa: A qualitative study. BMC Health Serv Res 2018;18:109.
- Provider Bias in the Provision of Contraceptives to Adolescent's Girls and Young Women in South West Nigeria. Available from: https://paa.confex.com/paa/2017/mediafile/ ExtendedAbstract. [Last accessed on 2018 Aug 19].
- National Population Commission, Federal Republic of Nigeria, Abuja, Nigeria. Nigeria Demographic and Health Survey 2013. Rockville (MD): ICF International; 2014.
- Ahanonu EL. Attitudes of healthcare providers towards providing contraceptives for unmarried adolescents in Ibadan, Nigeria. J Fam Reprod Health 2014;8:33-40.
- Hilary MS, Ilene SS, Meghan C. Contraceptive service provider imposed restrictions to contraceptive access in urban Nigeria. BMC Health Serv Res 2017;17:268.
- Boamah EA, Asante KP, Mahama E, Manu G, Ayipah E, Adeniji E, et al. Use of contraceptives among adolescents in Kintampo, Ghana: A cross-sectional study. Open Access J Contracept 2014;5:7-15.
- Duhaime-Ross A. The Best Contraceptives for Teens are IUDs and Implants, CDC says They are Safe and Appropriate for Teens. CDC; 2015. Available from: https://www.theverge. com/2015/4/7/8364721/best-teen-birth-control-iud-implant-cdc. [Last cited on 2018 Aug 22].
- Orr MT. Private physicians and the provision of contraceptives to adolescents. Fam Plan Perspect 1984;16:83-6.
- WHO. 2015 Medical Eligibility Criteria for Contraceptive Use. 5th ed. Geneva: WHO Press.