Neutrophil Cell Population Data biomarkers for Acute Bacterial Infection
Eloisa Urrechaga1*, Oihane Boveda1, Urko Aguirre2, Susana Garcia2, Esther Pulido3
2.Department of Research Unit, REDISSEC, Health Services Research on Chronic Patients Network, Hospital Galdakao-Usansolo, Galdakao Vizcaya, Spain.
3.Department of Emergency, Servicio de Urgencias, Hospital Galdakao-Usansolo, Galdakao Vizcaya, Spain.
Citation : Urrechaga E, Boveda O, Aguirre U, Garcia S, Pulido E. Neutrophil Cell Population Data Biomarkers for Acute Bacterial Infection. J Pathol Infect Dis 2018;1(1):1-7.
Cell population data (CPD) reported by Sysmex XN analyzer provide quantitative information on morphological and functional characteristics of leukocytes. We aimed to evaluate the value of CPD in the clinical decision-making in patients with fever and to assess the clinical value for the early diagnosis of acute bacterial infection, in comparison with classical markers.
A total of 215 consecutive patients with fever (bacterial or viral) and 212 healthy subjects without alterations in the hemogram were studied. The analysis was performed within 24-36 h from the onset of fever. Mann-Whitney U-test and Kruskal-Wallis ANOVA were applied to detect statistical differences of group, statistically significant P < 0.05. Receiver operating characteristic (ROC) curve analysis was utilized to establish the diagnostic performance of CPDs in the diagnosis of bacterial infection in a group of patients with fever.
The values of neutrophil granularity intensity and neutrophil reactive intensity showed increasing values from healthy, viral, to bacterial infections. NEUT-WY was the CPD with the best performance for the diagnosis of bacterial infection. Area under curve (AUC) 0.916 (95 % confidence interval 0.883-0.942) for a cutoff >616 the sensitivity was 87.1 % and the specificity was 85.4 %. This AUC presented no differences with those of percentage of neutrophils (P = 0.4451) nor neutrophil/lymphocyte ratio (0.2769).
NEUT-WY reflects an increase in the nucleic acid content of neutrophils in response to bacteria, and it is a reliable test for the diagnosis of acute bacterial infection and could aid in discriminating the etiology of fever.
Leukocytes, Neutrophil function, Sysmex
INTRODUCTION
Bacterial infections are a major cause of morbidity and mortality. The correct and timely diagnosis is critical for proper patient management [1].
The laboratory tests most often ordered are cultured for bacterial microorganisms, complete blood count with differential, and often a manual count for immature granulocytes. The measurements of c-reactive protein (CRP), serum procalcitonin (PCT),[2] and CD64 expression on peripheral blood leukocytes [3,4] have shown to improve diagnostic sensitivity and specificity for bacterial infection. These tests, however, require significant technical support and are relatively expensive.
During acute bacterial infection, an increase in neutrophil production from the bone marrow is expected; leukocyte and absolute neutrophil count, percentage of neutrophils, and especially, increases in bands and other immature neutrophils have been used as a laboratory test representing acute bacterial infections.
The modern hematology analyzers are able to provide accurate, fast, and cost-effective automated leukocyte differential counts with greater quantitative reliability. Technological advances allow more in-depth information concerning the characteristics of blood cells to be obtained, and along with the five subsets of leukocytes, quantitation of immature leukocytes (IG%) is reported by Sysmex XE series analyzers (Sysmex Corporation, Kobe, Japan) [5].
Sysmex XN applies flow cytometry and fluorescence to measure individual cells: the differential leukocyte count is based on criteria of cellular granularity (side scatter light), cell volume and shape (forward scatter light), and nucleic acid/protein content of cells (fluorescent light intensity), by preincubation with unique surfactant reagents and fluorescence staining.
Cell population data (CPD) are the numerical data (mean and width of dispersion of events measured) representing volume, granularity, and complexity for each cell [6].
CPD is reported together with the basic complete blood count. CPD provides quantitative information concerning the morphological and functional characteristics of neutrophils, monocytes, and lymphocytes, thus allowing a more detailed study of the cells and to detect any morphological variations (and thus functional status) in response to stimuli, such as infections.
We aimed to evaluate the value of this extended information in the clinical decision-making in patients with fever and to assess the clinical significance of CPD parameters as biomarkers for the early diagnosis of acute bacterial infection.
MATERIALS AND METHODS
WDF channel discriminates the leukocytes using flow cytometry [Figure 1].
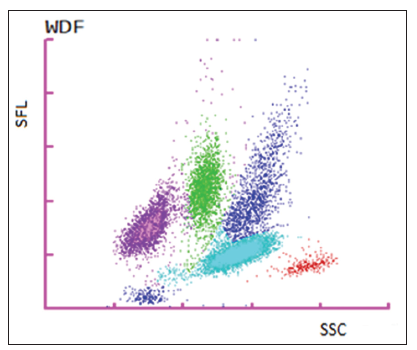
The optical signals along X-axis (side scatter) are related to the internal complexity; fluorescence along Y-axis represents nucleic acid content, while forward scatter (Z-axis) is proportional to cell size.
Mean values and standard deviation are recorded for each subset.
The width of dispersion of the values represents heterogeneous signals. Those parameters are calculated according to distribution width as it represents the range of the distribution of the major population, excluding outliers below 20% peak height in the distribution curve. The units are arbitrary of light scatter.
The following CPD is reported along the X-axis: Neutrophils complexity (NE-SSC), lymphocytes complexity (LY-X), monocytes complexity (MO-X), width of dispersion of neutrophils complexity (NE-WX), width of dispersion of lymphocytes complexity (LY-WX), and width of dispersion of monocytes complexity (MO-WX); CPD on the y-axis: Neutrophils fluorescence intensity (NE-SFL), lymphocytes fluorescence intensity (LY-Y), monocytes fluorescence intensity (MO-Y), width of dispersion of neutrophils fluorescence (NEWY), width of dispersion of lymphocytes fluorescence (LYWY), and width of dispersion of monocytes fluorescence (MO-WY); and CPD reported on the z-axis: Neutrophils size (NE-FSC), lymphocytes size (LY-Z), monocytes size (MOZ), width of dispersion of neutrophils size (NE-WZ), width of dispersion of lymphocytes size (LY-WZ), and the width of dispersion of monocytes size (MO-WZ).
Based on this technology and CPD parameters, Sysmex has introduced a set of new diagnostic parameters that support detecting and monitoring inflammatory diseases and infections. The "Extended Inflammation Parameters" are measured in the WDF channel and become diagnostic parameters with XN IPU software version 21.12.
The Extended Inflammation Parameters are a package of various clinical parameters that let one assesses the activation status of neutrophils (Neutrophil Granularity Intensity [NEUT-GI] and Neutrophil Reactive Intensity [NEUT-RI]) and lymphocytes (RE-LYMP and AS-LYMP) quantitatively. NEUT-GI corresponds with NE-SSC and NEUT-RI with NE-SFL.
Regarding the lymphocyte new parameters, RE-LYMP and AS-LYMP (reactive and antibody-secreting lymphocytes) are clinically relevant only after malignancy has been excluded, which is done by the WPC channel in a XN20. Verification of the capabilities on this channel is not included in the present study.
The observational prospective study was conducted in the Core Laboratory of the Galdakao-Usansolo Hospital, after receiving approval from the Research Ethics Committee and in collaboration with the Research Unit of the Barrualde District (Galdakao, Biscay, Spain).
The study group included 215 consecutive patients with fever (mean age 48, range 15-85 years, 48% of male, and 52% of female); exclusion criteria were hematological malignancies. 212 healthy subjects without quantitative nor morphological alterations in the hemogram were the control group with the mean age 54, range 19-63 years, 43% of male, and 57% of female.
The diagnosis of each patient was retrieved from their laboratory and medical records. The hemogram and biochemistry tests analyzed in the present study were performed within 24-36 h from the onset of fever.
Bacterial infections were proven by positive culture, while positive serology or molecular tests documented viral infections.
Blood samples were collected in tubes containing K2-EDTA and processed in a Sysmex XN 9000 robotic system (two XN10 and two XN 20) (Sysmex Corporation, Kobe, Japan).
CRP and PCT were processed using a Cobas 8000 (Roche Diagnostics, Basel, Switzerland) biochemical analyzer, tests for viruses on Cobas® Liat® System or Cobas® Amplico, LightCycler (Roche Diagnostics, Basel, Switzerland).
Statistical analyses were performed using SPSS version 23.0.1 for Windows (SPSS Inc., Chicago, IL, USA) and graphs with MedCalc version 11.3.3.0 for Windows (MedCalc Software, Mariakerke, Belgium).
Kolmogorov-Smirnov test was applied to detect normal or skewed distributions.
Mann-Whitney U-test was applied to detect statistical differences between two groups and Kruskal-Wallis ANOVA (more than two groups); P < 0.05 was considered statistically significant. For post hoc comparisons of outcomes between each pair of groups, Bonferroni correction was applied.
Receiver operating characteristic (ROC) curve analysis was utilized to establish the diagnostic performance of the study parameters (CPDs and classic markers) in the diagnosis of bacterial infection in a group of patients with fever.
Correlation between CPDs with the best ROC analysis results (higher area under curve [AUCs]) and biochemical parameters was studied using Spearman's test.
RESULTS
Patients were suffered from pneumonia, urinary infections, meningitis, gastroenteritis, or pharyngitis, caused by bacteria and viral infections (mononucleosis, respiratory infections, and measles).
CPD for the three groups, healthy subjects and viral and bacterial infection, are displayed in Table 1, along with P values comparing both groups with fever; the values are presented as median and interquartile ranges due to skewed distribution.
All 18 CPDs in viral and bacterial infection patients were statistically different from healthy individuals (data not shown in Table 1, P < 0.001).
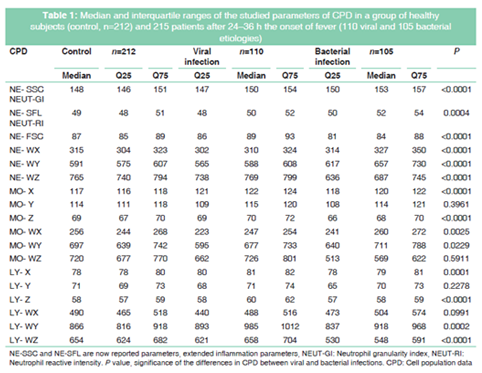
As neutrophils play the major role in the immune response to acute bacterial infections, we focused mainly on the CPD related to changes in reactive neutrophils.
In bacterial infection, IG% median was 0.8 % (25-75 quartiles 0.6-2.7%); only 10 % of the patients had IG% >5%, the criteria for manual revision of blood smears.
The values of the extended inflammatory parameters NEUT-GI and NEUT-RI showed increasing values from healthy, viral, to bacterial infections, as was expected from the biology and activation status of the cells. Despite significant differences between bacterial and viral infectious patients, the values of NEUT-GI and NEUT-RI overlapped in both groups.
The overlapping was minor for NEUT-WY [Figure 2], and thus, this parameter had better performance for the diagnosis of bacterial infection and the differential diagnosis of fever from bacterial or viral etiology. ROC analysis for 105 bacterial versus 110 viral infections is as follows:
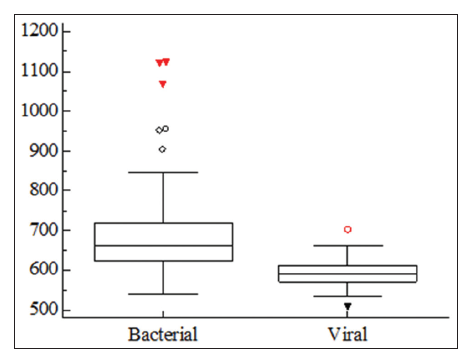
AUC 0.916 (95% confidence interval 0.883-0.942) for a cutoff >616, sensitivity 87.1%, and specificity 85.4%.
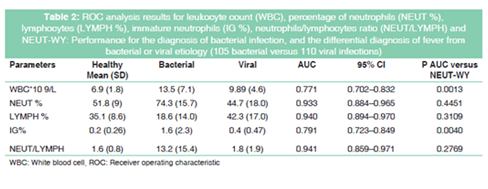
Table 2 summarizes ROC analysis results of the tests traditionally used for differential diagnosis of the etiology of fever. The AUC of NEUT%, LYMPH%, NEUT/LYMPH, and NEUT-WY presented no statistical differences and had better diagnostic performance than IG% and white blood cell.
Correlations between NEUT-WY and biochemical markers were found to be poor R=0.203 for PCT and R=0.576 for PCR.
DISCUSSION
The diagnosis of bacterial infections in an early phase remains a daily challenge. Clinical presentation of infections from different causative agents can be similar, making the correct diagnosis sometimes difficult.
Since bacterial infections are dangerous, empiric antibiotic therapy is immediately initiated when fever occurs, even before microbiological proof of an infection has been obtained. However, although untreated bacterial infections may cause serious complications, treating viral illnesses or non-infective causes of inflammation with antibiotics is not only ineffective but also contributes to the development of resistance,[7] increases costs, and adds the risks of toxicity and allergic reactions.
The combination of leukocyte count, left shift, CRP, and PCT is the most commonly employed parameters for evaluating the course of a bacterial infection but presents limitations.
Studies have concluded that the left shift is not useful for diagnosing bacterial infections because it is not observed on admission for all patients with bacterial infection. Left shift does not appear in the extremely early phase of bacterial infections but usually presents 12-24 h after onset. Using a time-series analysis (with at least two points) might increase the sensitivity and specificity of both tests for diagnosing a bacterial infection, but this means a delay in the decisionmaking process and the start of appropriate therapy [8].
Therefore, reliable and readily available parameters for the diagnosis of acute bacterial infection are necessary. An ideal biomarker should have altered values in an early phase to diagnose a bacterial infection using a one-time measurement (especially, taken on admission); in this regard, we have explored CPD, as part of the modern extended hemogram.
Neutrophils are members of the innate immune system. Their activation by cues derived from sites of inflammation results in exposure of distinct surface markers and de novo synthesis of cytokines, leading to neutrophil heterogeneity. Activated neutrophils are characterized by an increased deformability, increased motility, and increased adhesion by upregulation of membrane receptors, phagocytosis, degranulation, and release of cytokines and reactive oxygen intermediates [9].
In the present study, the values of NEUT-WY found in patients with bacterial infection indicate that this CPD reflects changes in structure and morphology of neutrophils in response to bacteria, with a marked increase in nucleic acid content. NEUT-WY was found to have the best diagnostic performance in differential diagnosis of bacterial versus viral infections, AUC 0.916.
Our results are in agreement with previous reports on the early change in NEUT-RI and NEUT-WY before IG variation in a 72-h frame time;[10] this characteristic makes this parameter of particular interest for differential diagnosis on admission of patients suffering fever.
Previous studies have brilliantly explored the utility of CPD as possible biomarkers for the early detection of infection or sepsis using Sysmex [11-13] or Coulter (Beckman-Coulter, Brea, California, USA) analyzers [14-17].
The differences in the technology of the analyzers of different manufactures explain the parameters with best diagnostic performances, volume and volume distribution width of neutrophils (Coulter), or CPD related to nucleic acid content NE-SFL (NEUT-RI) and NEUT-WY (Sysmex).
The former analyzer keeps the native shape and volume of the cells; the activated cells increase in volume, so this is the population data better reflecting the immune response. The latter applies perforation of the cell membrane with specific lysates; this chemical attack changes the cell integrity, so the volume measured is the volume after the addition of the Lysercell reagent. In this technology, activation in response to bacteria is detected by means of the increase of nucleic acid content, as a result of cytokine production in the early response of the innate immune system to infection.
NEUT-GI presented statistical differences among the three groups of patients; the values obtained are in concordance with the well-known morphologic changes of reactive neutrophils (toxic granulation, vacuolization, and Dohle bodies in the cytoplasm) in case of bacterial infection and can provide important diagnostic information.
Although microscopic evaluation of a peripheral blood smear can detect those morphologic changes, it is labor intensive, time-consuming, and expensive, as it requires manual examination by a trained professional. In addition, the results are subjective leading to imprecision [14]. The introduction of digital cell morphology devices has represented a true improvement for the examination of blood smears, but there is still a need for reclassification of cells, and the criteria of an experience professional remain mandatory.
Neutrophil CPD by Coulter counters and Granularity Index of the SYSMEX XE-5000 analyzer have been postulated to replace the manual microscopic revision, in certain clinical settings [18,19]. In an era of general shortage of budgets, the introduction of numerical data supporting cell morphology could be a possible solution.
A limitation of this study is that we have not evaluated the impact of introducing NEUT-GI (NE-SSC) in our algorithm for slide revision.
The improvement of the laboratory workflow and the reduction in turnaround time, due to reduction of the number of smears manually revised, deserve future investigation.
The support for differentiating between infection and inflammation, monitoring of infections, and the distinction of acute phase versus recovery phase of an infection are also topics to be extensively evaluated.
Some considerations must be taken into account when, based on the published data, a laboratory professional decides to use CPD as complementary tests in daily routine.
CPD are morpho-functional parameters, reflecting cell activation status of cells, so the effect of a delay in processing samples on results is a relevant matter.
Mecca et al. demonstrated that the stability of CPD depends on the parameter considered, time, and storage temperature; when stored at 4°C, NEUT-RI (NE- SFL), NEUT-GI (NE-SSC), MO-Y, MO-Z, LY -WX, and -LY WZ were stable until at least 8 h, while NE-WY, NE-WZ, and MO-WZ up to 4 h. The maximum stability of CPD when stored at room temperature is about 4 h [20].
NEUT-GI and NEUT-RI are now reported parameters (XN IPU software version 21.12), but all others CPD are research parameters, and no quality control (IQC) materials with assigned target values are available.
A "sensitivity adjustment" procedure, similar to the calibration and IQC procedure used in the reporting of routine tests, can be provided by the XN-instrument and are performed before reporting CPD items [12].
Moreover, the QC Module includes the X-Bar which provides a daily patient moving average that is configurable by the customer and by measure. These procedures should be useful in monitoring analyzer performances over the time and the concordance of results among all of them [21]. Including average of normal into the daily QC becomes more important when control materials are lacking [22,23].
In summary, we conclude that NEUT-WY could be a reliable test for the diagnosis of acute bacterial infection and, in conjunction with clinical and analytical data, can aid in discriminating the etiology of fever.
REFERENCES
- World Health Organization (WHO).WHO Report on Infectious Disease: Removing Obstacles to Healthy Development. Geneva: WHO; 1999.
- Simon L, Gauvin F, Amre DK, Saint-Louis P, Lacroix J. Serum procalcitonin and C-reactive protein levels as markers of bacterial infection: A systematic review and meta-analysis. Clin Infect Dis 2004;39:206-17.
- Hoffmann JJ. Neutrophil CD64: A diagnostic marker for infection and sepsis. Clin Chem Lab Med 2009;47:903-16.
- de Jong E, de Lange DW, Beishuizen A, van de Ven PM, Girbes AR, Huisman A, et al. Neutrophil CD64 expression as a longitudinal biomarker for severe disease and acute infection in critically ill patients. Int J Lab Hematol 2016;38:576-84.
- Ansari-Lari MA, Kickler TS, Borowitz MJ. Immature granulocyte measurement using the sysmex XE-2100.Relationship to infection and sepsis. Am J Clin Pathol 2003;120:795-9.
- Linssen J, Aderhold S, Nierhaus A, Frings D, Kaltschmidt C, Zanker K, et al. Automation and validation of a rapid method to assess neutrophil and monocyte activation by routine fluorescence flow cytometry in vitro. Cytometry B Clin Cytom 2008;74:295-309.
- World Health Organization (WHO). WHO Report on Infectious Disease: Overcoming Antimicrobial Resistance. Geneva: WHO; 2000.
- Honda T, Uehara T, Matsumoto G, Arai S, Sugano M. Neutrophil left shift and white blood cell count as markers of bacterial infection. Clin Chim Acta 2016;457:46-53.
- Silvestre-Roig C, Hidalgo A, Soehnlein O. Neutrophil heterogeneity: Implications for homeostasis and pathogenesis. Blood 2016;127:2173-81.
- Cornet E, Boubaya M, Troussard X. Contribution of the new XN-1000 parameters NEUT-RI and NEUT-WY for managing patients with immature granulocytes. Int J Lab Hematol 2015;37:e123-6.
- Luo Y, Lin J, Chen H, Zhang J, Peng S, Kuang M, et al. Utility of neut-X, neut-Y and neut-Z parameters for rapidly assessing sepsis in tumor patients. Clin Chim Acta 2013;422:5-9.
- Park SH, Park CJ, Lee BR, Nam KS, Kim MJ, Han MY, et al. Sepsis affects most routine and cell population data (CPD) obtained using the sysmex XN-2000 blood cell analyzer: Neutrophil-related CPD NE-SFL and NE-WY provide useful information for detecting sepsis. Int J Lab Hematol 2015;37:190-8.
- Buoro S, Seghezzi M, Vavassori M, Dominoni P, Apassiti Esposito S, Manenti B, et al. Clinical significance of cell population data (CPD) on sysmex XN-9000 in septic patients with our without liver impairment. Ann Transl Med 2016;4:418.
- Chaves F, Tierno B, Xu D. Quantitative determination of neutrophil VCS parameters by the coulter automated hematology analyzer: New and reliable indicators for acute bacterial infection. Am J Clin Pathol 2005;124:440-4.
- Chaves F, Tierno B, Xu D. Neutrophil volume distribution width: A new automated hematologic parameter for acute infection. Arch Pathol Lab Med 2006;130:378-80.
- Bagdasaryan R, Zhou Z, Tierno B, Rosenman D, Xu D. Neutrophil VCS parameters are superior indicators for acute infection. Lab Hematol 2007;13:12-6.
- Park DH, Park K, Park J, Park HH, Chae H, Lim J, et al. Screening of sepsis using leukocyte cell population data from the coulter automatic blood cell analyzer dxH800. Int J Lab Hematol 2011;33:391-9.
- Neal A, Simon-Lopez R, Barella S. Use of neutrophil cell population data for the detection of neutrophil hyper granulation and other neutrophil inclusions as dohle bodies, cytoplasm vacuolation. Blood 2014;124:4966.
- Zimmermann M, Cremer M, Hoffmann C, Weimann K,Weimann A. Granularity index of the SYSMEX XE-5000 hematology analyzer as a replacement for manual microscopy of toxic granulation neutrophils in patients with inflammatory diseases. Clin Chem Lab Med 2011;49:1193-8.
- Mecca T, Seghezzi M, Gherardi P, Resmini S, Napolitano G, Parimbeli M, et al. Assessment of the analytical performance of novel parameters on automates blood count on sysmex XN-9000. Biochim Clin 2016;40:217-24.
- Simon-Lopez R, Buoro S, Pacioni A, Seghezzi M, Manenti B. Quality control of structural paremeters (CELL POPULATION DATA) of sysmex XN series. Blood 2016;128:4887-8.
- Cembrowski GS, Chandler EP, Westgard JO. Assessment of "Average of normals" quality control procedures and guidelines for implementation. Am J Clin Pathol 1984;81:492-9.
- Kazmierczak SC. Laboratory quality control: Using patient data to assess analytical performance. Clin Chem Lab Med 2003;41:617-27.