Lumbar Hernia through an Iliac Crest Bone Graft Defect
Katyani Dubey1, Satyendra Tiwari1, Puneet1, Ajay Kumar Khanna1, Soumya Khanna2
2.Department of Anatomy, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India.
Citation :Dubey K, Tiwari S, Puneet, Khanna AK, Khanna S. Lumbar Hernia through an Iliac Crest Bone Graft Deffect. Clin J Surg 2018;1(1):1-3.
The most common source for autologous bone graft in orthopedics practice is the iliac crest. This technique may be associated with various complications such as arterial injury, nerve injury, ureteral injury, ileus, hematoma, pelvic instability, fracture, and herniation. Herniation through an iliac crest defect is a very rare but major complication of this procedure. The incidence of lumbar hernia after iliac crest bone graft harvesting is estimated to be 5-9%. This disease is unique for its anatomic specialty and for its rarity, since most surgeons do not have exposure to such a problem. Surgery is recommended as there is risk of 25% incarceration and 10% risk of strangulation with this hernia. We present two cases of lumbar incisional hernia following iliac bone harvesting which was repaired using polypropylene mesh which was fixed to iliac bone with screw.
Bone harvesting, mesh, oblique, polypropylene, strangulation.
INTRODUCTION
The most common source for autologous bone graft in orthopedics is the iliac crest. It may be harvested from the anterior or the posterior iliac crest [1]. Reported complications include arterial injury, nerve injury, ureteral injury, ileus, hematoma, pelvic instability, and fracture [2]. A rare but major complication of this procedure is herniation through an iliac crest defect.
Anatomically, lumbar hernias are bound above by the 12th rib, below by the iliac crest, the erector spinae muscle medially and laterally by the external oblique muscle. The incidence of lumbar hernia after iliac crest bone graft harvesting is estimated to be 5-9% [3,4]. This disease is unique for its anatomic specialty and for its rarity, since most surgeons do not have exposure to such a problem.
Hence, surgery is recommended secondary to the 25% risk of incarceration and 10% risk of strangulation with lumbar hernias [5]. We present two cases of lumbar incisional hernia repair using prosthetic mesh which was fixed to iliac bone with cortical screw.
CASE REPORT
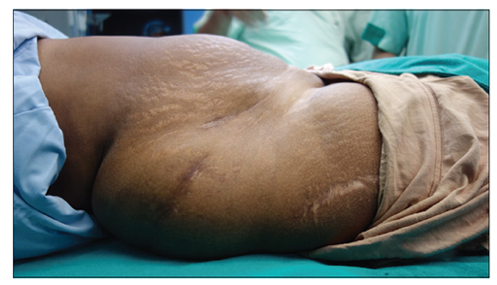
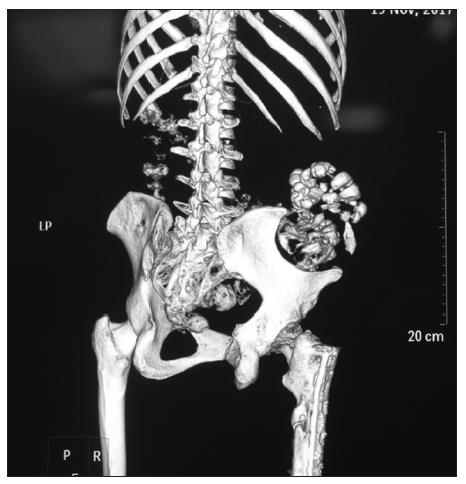
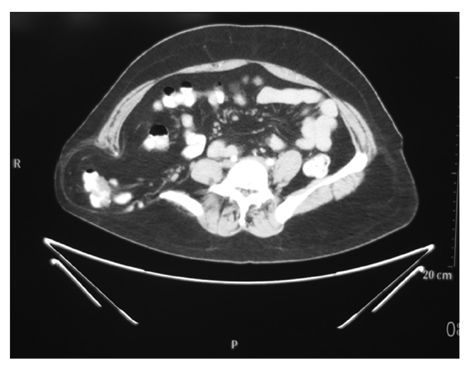
A 38 years female presented with complain of swelling in the right flank for 1 year associated with dull aching pain. She has a history of femur fracture for which iliac bone grafting was done 3 years back. On physical examination, there is a horizontal scar present on the right side from midclavicular line to midaxillary line at the level of iliac crest. Swelling was reducible with a cough impulse present [Figure 1]. On palpation, five fingers defect present with content as bowel. The patient was diagnosed to have incisional hernia. Hematological and biochemical investigations were unremarkable. Computed tomography scan was suggestive of the right lower anterolateral abdominal wall hernia with a defect of 49 mm in the right iliac crest with herniation of large and small bowel loops along with mesenteric fat [Figures 2-4]. Surgery was performed with an oblique incision, to perform reduction of abdominal content by closing the defect with adjacent fascia. The surgery site was reinforced with the placement of a 15 cm X 15 cm polypropylene mesh which was fixed to the iliac bone with a cortical screw [Figure 5] and drain was placed. The patient has been followed up without any recurrence of the disease.


A 65-year-old female presented with swelling in the left lumbar region for 6 years. She was operated on 6 years back, during which a bone graft was taken from her left iliac crest for a knee replacement. The patient also had dull aching pain at the site of the hernia. A physical examination revealed reducible swelling in the left lumbar region at the site of the left iliac crest.
The patient was diagnosed with an incisional hernia through the defect in iliac crest. Laboratory investigations were within normal limits. A computerized tomography (CT) scan showed a defect in the left iliac crest with a herniation of abdominal content. Surgery was performed with an oblique incision, to perform reduction of abdominal content by closing the defect with adjacent fascia and onlay mesh repair by polypropylene mesh was done. The patient has been on follow up for more than 5 years without any recurrence.
DISCUSSION
A lumbar hernia following an iliac crest bone graft harvesting is a rare complication which is more frequent in females than males [1] The incidence of hernia following iliac crest bone graft harvesting is approximately 5-9% [2]. A lumbar hernia usually occurs when the full thickness of the iliac bone graft has been removed or when there is a substantial defect after the bone graft harvesting.
Patients can develop symptoms within a few days of the primary bone graft harvest to many years after the surgery. The lumbar area is a space bounded by: The lower edge of the 12th rib superiorly, the iliac crest inferiorly, the erector spinae muscle and the lumbar spinous processes medially, and the external oblique muscle laterally. This area is divided into two compartments: Superior (Grynfeltt hernia) and inferior triangle (Petit hernia) [3]. The superior lumbar triangle is bordered superiorly by the 12th rib, the lumbocostal ligament, and the serratus posterior inferior muscle, laterally by the internal oblique muscle, and medially by the erector spinae muscle. The inferior lumbar triangle includes the iliac crest inferiorly, the external oblique muscle laterally, and the latissimus dorsi muscle medially. In our patient, the hernia developed through the inferior lumbar triangle.
After an iliac crest bone graft harvest, the lumbar hernia may present with swelling over the iliac crest, as well as some discomfort. This may be associated with signs of intestinal obstruction. A CT scan is commonly used to confirm the diagnosis and also to delineate the anatomy [3]. Repairing such hernias can be done by patching up the soft tissue, or by reinforcing the soft tissue with fascial flaps, bone transfer, or mesh. The tension-free mesh repair can be performed with a laparoscopic, retroperitoneal, or transabdominal approach. Attaching the mesh to the iliac bone is facilitated by suture bone anchors or corkscrew anchors. Another technique of soft tissue transfer involves using the transversalis fascia, abdominal musculature, and tensor fascia lata. Alternatively, the anterior superior iliac spine can be moved inferiorly and posteriorly to cover the defect in the iliac bone. We chose to repair the hernia of the iliac crest defect using an extraperitoneal approach with an onlay mesh.
Lumbar hernia is a rare complication following iliac bone graft harvest [4]. Various surgical methods have been recommended to prevent such hernia. Ideally, harvesting the full thickness of the bone graft should be avoided. Instead, a partial thickness bone graft should be done if possible, to achieve similar results. Alternatively, the primary defect created following harvesting should be closed with mesh to prevent a lumbar hernia. The hernia developed in the postoperative period can be successfully repaired with mesh [5].
REFERENCES
- Dimitriou R, Mataliotakis GI, Angoules AG, Kanakaris NK, Giannoudis PV. Complications following autologous bone graft harvesting from the iliac crest and using the RIA: A systematic review. Injury 2011;42 Suppl 2:S3-15.
- Fowler BL, Dall BE, Rowe DE. Complications associated with harvesting autogenous iliac bone graft. Am J Orthop (Belle Mead NJ) 1995;24:895-903.
- Auleda J, Bianchi A, Tibau R, Rodriguez-Cano O. Hernia through iliac crest defects. A report of four cases. Int Orthop 1995;19:367-9.
- Forrest C, Boyd B, Manktelow R, Zuker R, Bowen V. The free vascularised iliac crest tissue transfer: Donor site complications associated with eighty-two cases. Br J Plast Surg 1992;45:89-93.
- Woodward AM, Flint LM, Ferrara JJ. Laparoscopic retroperitoneal repair of recurrent postoperative lumbar hernia. J Laparoendosc Adv Surg Tech A 1999;9:181-6.